
Recommended
More Related Content
What's hot
What's hot (19)
Similar to Parkinson's disease
Similar to Parkinson's disease (20)
More from M Ridhwan Abd Razak
More from M Ridhwan Abd Razak (20)
Recently uploaded
Recently uploaded (20)
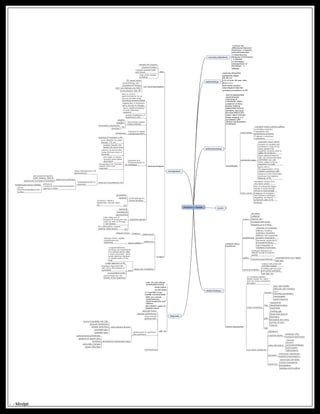
Parkinson's disease
- 1. Parkinson's disease Learning objectives: Know the differences between Parkinson ’s disease and parkinsonism Describe the features of Parkinson ’ s disease Principles management of Parkinson ’ s disease epidemiology majority idiopathic symptoms begin 55-60 yrs 1% of over 60 year olds M:F=1.5:1 2nd most common neurological disorder greatest prevalence in US pathophysiology loss of pigmentted dopaminergic neurones in substantia niagra presence of lewy bodies withing pigmented neuron 60-80% neurones are lost before the motor signs emerge braak staging 1-6 correlates with clinical manifestation of disease scientifically basal ganglia =caudate nucleus+globus pallidus controlling voluntary movements and establishing postures if altered->unwanted movements substantia niagra important motor centre projects to caudate and putamen(2 nuclei of the basal ganglia that together comprise what is called the striatum) these NIGROSTRIATAL cells use neurotransmitter DOPAMINE and cells within niagra produce dopamine normally lesion site in PD-degeneration of the melanin-containing cells absence of the transmitter produces the crippling features of PD motor circuit modulates output from the motor cortex loss of substantia niagra results in dysfunctional stimuli to basal ganglia imbalance of excitatory and inhibitory pathways regulating movement--> symptoms seen in PD Subtopic causes clinical findings cardinal motor symptoms tremor pill rolling unilateral rapid at rest increased with stress frequency of 4-5 Hertz bradykinesia slowness of movement difficulty initiating voluntary movement difficulty with sequential complex movements decreased amplitude of movement(writing) rapid fatigability of repetitive movements rigidity increased resistance of relaxed muscle to passive stretch commonly asymmetrical cogwheel(tremor and rigidity lead pipe postural instability balance well preserved until later stages shuffling gait and poor arm swing contribute high falls risk clinical assessment on reviewing patients always assess for motor and non motor symptoms and signs motor symptoms function poor bed mobility diffuculty with transfers poor dexterity/coordination micrographia painful dystonia face hypophonia dysphagai/drooling hypomimia gait shuffling gait flexed axial posture festination decreased arm swing turning 'en bloc' freezing falls non motor symptoms depression cognitive decline dementia~30% executive dysfunction sleep disturbance insomnia daytime somnolence/fatique vivid dreams hallucinations sensation orthostatic hypotension impaired proprioception autonomic seborrhoeic dermatitis urinary incontinence constipation sweating abnormalities diagnosis med. Hx and clinical examination(triad) observation no lab tests CT and MRI brain usually unremarkable MRI can outrule multi-infarcts, hypdrocephalus and wilsons PET/SPECT useful in atypical cases diff. Dx essential tremor vascular parkinsonism drug-induced parkinsonism parkinsonism in parkinson plus syndrome multi systems atrophy postural instability with falls postural hypotension bladder dysfuntion pyramidal signs cerebellar signs progressive supranuclear palsy parkinsonism(symmetrical) paralysis of upward gaze dementia personality changes speech difficulties thyrotoxicosis management aims educate and support preserve function maintain general health and fitness treat other medical problems non-pharmacological PD supprt group physiotherapy and occupational therapy SALT and dietician and MSW communication with GP pharmacological aims to control signs/symptoms for as long as possible while minimising adverse effects replacement of dopamine def is the key to therapy aim to stable stimulation of brain dopamine receptors prevent breakdown of dopamine in CNS monoamine oxidase inhibitor(MOAB) selgiline rasagiline S/E orthostatic hypotension insomnia Catechol-O-methyl transferase(COMT)entacopone Levodopa and DCI(benserazide or carbidopa) mainstay of treament in PD most effective for initial therapy >70 yrs greatest benefit with fewest S/E short term restore normal function using minimum dose of levodopa pre meals on empty stomach gives better absorption domperidone for transient nausea when start treatment long term troublesome S/E motor fluctuation(on-off phenomenon) dyskinesia(chorea or dystonia) peak dose dyskinesia add dopamine agonist, COMT inhibitor, MAO-B slowly lower the dose of levodopa refractory symptoms-apomorphine(dopamine agonist is useful britajet(subacute as needed) subcut infusion(hospitalised prior to this) anticholinergic for tremor/drooling procyclidine biperidin S/E confusion, memory impairment, blurred vision etc dopamine agonist ropinerole pramipexole apomorphine helps delay use of levodopa in young pts and useful as add-on therapy in late disease S/E OH, hallucination, nausea, oedema, sleep attacks surgery thalamotomythalamusreduces tremor pallidotomy globus pallidus reduces tremor, rigidity, bradykinesia and dyskinesia deep brain stimulation surgical treatment involving the implantation of a medical device called a brain pacemaker, which sends electrical impulses to specific parts of the brain need a clear diagnosis of PD levodopa responsive pts with motor fluctuations or dyskinesia no psychiatric probs good insight into risk benefit of this treatment - - Mindjet