
Recommended
Recommended
More Related Content
Similar to A NATIONAL SURVEY OF FAMILY PHYSICIANSPERSPECTIVES ON COLLA.docx
Similar to A NATIONAL SURVEY OF FAMILY PHYSICIANSPERSPECTIVES ON COLLA.docx (20)
More from ransayo
More from ransayo (20)
Recently uploaded
Recently uploaded (20)
A NATIONAL SURVEY OF FAMILY PHYSICIANSPERSPECTIVES ON COLLA.docx
- 1. A NATIONAL SURVEY OF FAMILY PHYSICIANS: PERSPECTIVES ON COLLABORATION WITH MARRIAGE AND FAMILY THERAPISTS Rebecca E. Clark Lifespan Family Healthcare, Newcastle, Maine Deanna Linville University of Oregon Karen H. Rosen Virginia Polytechnic Institute and State University Recognizing the fit between family medicine and marriage and family therapy (MFT), members of both fields have made significant advances in collaborative health research and practice. To add to this work, we surveyed a nationwide random sample of 240 family physicians (FPs) and asked about their perspectives and experiences of collaboration with MFTs. We found that FPs frequently perceive a need for their patients to receive MFT- related care, but their referral to and collaboration with MFTs were limited. Through responses to an open-ended question, we gained valuable information as to how MFTs could more effectively initiate collaboration with FPs. Despite the success of medical family therapists in providing integrative, collaborative
- 2. healthcare, we know little about how commonly family physicians (FPs) and marriage and fam- ily therapists (MFTs) collaborate in routine patient care. To our knowledge, there have been no studies published from the perspective of the FP that describe the extent to which FPs seek the collaboration of MFTs, the degree to which they are aware of MFT as a field, their per- ceived need for their patients to receive MFT, or their attitude toward MFT as a potential resource for patient treatment. Leaders in family medicine and MFT recognize the common occurrence of mental health concerns arising in a medical visit. In fact, it has been estimated that more than 60% of patient visits to primary care physicians (PCPs) include mental health concerns (Moon, 1997), and many of these concerns may not be the presenting complaint (Jackson & Tisher, 1996; Schurman, Kramer, & Mitchell, 1985). Several MFT ⁄ FP teams have developed models for col- laboration (Doherty & Baird, 1983; Dym & Berman, 1986; Hepworth & Jackson, 1985; Sea- burn, Lorenz, Gunn, Gawinski, & Mauksch, 1996). Other researchers and practitioners have written books that serve as a guide to other mental health practitioners for how to be effective collaborators with other healthcare practitioners (e.g., Seaburn et al., 1996). The specialty of family medicine, which arose in the 1960s, embraces a systemic, biopsy- chosocial perspective to illness that stresses the importance of caring for the whole person within his or her family, social context, and life cycle stage
- 3. (Chung, 1996; Fischetti & McCutchan, 2002). It is not surprising that FPs regularly treat their patients’ mental health problems. By definition of their specialty, FPs are trained to integrate behavioral science con- cepts with their biomedical training (AAFP, 2000; Seaburn et al., 1996) as well as to manage Rebecca E. Clark, MS, Lifespan Family Healthcare, Newcastle, Maine; Deanna Linville, PhD, Couples and Family Therapy Program, Department of Counseling Psychology and Human Services, University of Oregon; Karen H. Rosen, EdD, Marriage and Family Therapy Program, Department of Human Development, Virginia Polytechnic Institute and State University, Northern Virginia Center. Address correspondence to Rebecca Clark, Lifespan Family Healthcare, 80 River Road, Newcastle, Maine 04553; E-mail: [email protected] Journal of Marital and Family Therapy April 2009, Vol. 35, No. 2, 220–230 220 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009 psychotropic medication. The American Academy of Family Physicians (AAFP, 2000) recom- mended curriculum guidelines delineate how family medicine residents must understand the
- 4. individual in the context of his or her family, as well as the emotional impact of illness, and be able to evaluate and diagnose mental health disorders from a biopsychosocial perspective. For decades, authors in family medicine and collaborative healthcare journals have published literature regarding the use of MFT techniques such as family systems thinking, the use of gen- ograms, meeting with the entire family, brief therapy techniques, and when to refer patients for family therapy (Bader, 1990; Bloom & Smith, 2001; Bullock & Thompson, 1979; Christie-Seely, 1981; Davis, 1988; Frank, 1985; Lang et al., 2002; Mayer et al., 1996; Tomson & Asen, 1987). Additionally, organizations such as the Collaborative Family Healthcare Association (CFHA; see http://www.cfha.net) and the Society for Teachers of Family Medicine (STFM; see http:// www.stfm.org) continue to promote research, education, and practice in collaborative health- care. Given family medicine’s emphasis on family systems, the family as the unit of care, and biopsychosocial perspective, it seems that MFTs would be a logical, and even sought-after, complement to FPs in providing comprehensive patient care. As a specialty of MFT, medical family therapy (MedFT) has already made significant advances in this area. Particularly helpful for chronic illness, MedFT has enabled MFTs to skillfully integrate the biopsychosocial-spiritual perspective, a systemic integration of physical and emotional health, familial ⁄ social relationships, and spiritual belief systems, with a family systems framework (McDaniel, Hepworth, & Doherty, 1992a; Rolland, 1994; Weihs, Fisher, &
- 5. Baird, 2002). Specifically trained medical MFTs have effectively collaborated with medical prac- titioners to provide care for families struggling with chronic medical illnesses such as infertility (Burns, 1999; McDaniel, Hepworth, & Doherty, 1992b), cancer (Yeager et al., 1999), childhood asthma and diabetes, cardiovascular and neurological disorders (Campbell & Patterson, 1995), obesity (Campbell & Patterson, 1995; Flodmark, Ohlsson, Ryden, & Sveger, 1993), somatoform disorder (McDaniel, Hepworth, & Doherty, 1995), dual diagnosis (Harkness & Nofziger, 1998), and anorexia nervosa (Dare & Eisier, 1995). Roadblocks to Identifying and Managing Patient Psychosocial Concerns There is a range of limitations to the quantity and quality of psychosocial care FPs can deliver to their patients. Researchers have identified lack of training (Christie-Seely, 1981; Fosson, Elam, & Broaddus, 1982), time (Glied, 1998; Rost, Humphrey, & Kelleher, 1994; Tomson & Asen, 1987), patient reluctance (Kainz, 2002; Williams et al., 1999), managed care (DeGruy, 1997; Fisher & Ransom, 1997), and lack of confidence (Gerdes, Yuen, & Frey, 2001; Williams et al., 1999) as roadblocks to FPs and other PCPs identifying and treating patient mental health needs. Roadblocks to referral. Regardless of to whom they refer, physicians identify several road- blocks when referring patients to mental health professionals. These have included patient reluctance, the unavailability of appropriate mental health
- 6. professionals in rural communities, lack of affordability of mental health, significant lag time between referral and appointment availability, lack of adequate feedback from mental health professionals, the stigma patients attach to mental healthcare, and poor communication from the mental health professional (Kainz, 2002; Kushner et al., 2001; McCulloch et al., 1998; Reust, Thomlinson, & Lattie, 1999; Rost et al., 1994; Williams et al., 1999). The purpose of this exploratory study was to discover FPs’ views of MFTs as potential collaborators on the healthcare team. Specifically, this study seeks to answer three research questions: (1) Do FPs view MFTs as a resource for patients with psychosocial needs? (2) Are FPs interested in collaborating with MFTs? (3) What would make MFTs more helpful collaborators? April 2009 JOURNAL OF MARITAL AND FAMILY THERAPY 221 METHODS This study was a national survey of 240 FPs. A questionnaire was mailed to 240 board cer- tified FPs who were randomly selected from the AAFP directory. The inclusion criteria were engagement in the practice of family medicine, graduation from a U.S. medical school, comple- tion of residency after 1969, and residence within a U.S. zip
- 7. code. Participants and Procedures After obtaining IRB approval, a randomly selected mailing list was obtained from the AAFP. Questionnaires were mailed along with an introductory letter describing the study, a brightly colored sticky note with a brief hand-written note, and a self-addressed stamped envelope. Each questionnaire was numbered to enable a follow- up mailing to nonrespondents. During the first wave, 104 questionnaires were returned. After 4 weeks the same material was re-mailed to nonrespondents. After two mailings we received 153 responses, representing a 64% response rate. Of those responses, 16 questionnaires were excluded from analyses because respondents were no longer practicing family medicine full time. Consequently, there were a total of 137 usable questionnaires (57%). We received responses from FPs in 37 out of 42 states as well as an FP in Puerto Rico and a deployed military FP. Respondents had been in practice for an average of 12 years and were an average age of 46. Table 1 depicts demo- graphic data such as gender and geographical distribution of respondents. The four major census regions of the United States as well as U.S. territories and military were represented in the sample. Based on the AAFP 2002 census of their members (AAFP, 2003), the sample appears representative of both the gender and regional distribution of FPs throughout the United States.
- 8. Table 1 Demographics Variable Percentage of respondents Percentage of random sample Percentage of 2002 National AAFP Censusa Region Northeast 15 13 15 South 35 33 33 Midwest 27 33 28 West 21 20 21 U.S. territory ⁄ Army Post Office 2 2 3 Gender Male 66 71b Female 34 29b Note. n = 137. aMembership (U.S., U.S. Territories, and Military; AAFP, 2003). bActive AAFP members (this percentage includes 138 Canadian members and 350 foreign members that were not part of the sampled population). AAFP = American Academy of Family
- 9. Physicians. 222 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009 The questionnaire, which contained both closed and open-ended questions, was based on a review of literature and in consultation with MFTs and FPs. In the development phase, the questionnaire was administered to five FPs and revised based on their feedback. Analysis Quantitative data analyses were completed using SPSS for Windows, v10.0 (Norusis, 2000). Qualitative data were analyzed using a modified version of the constant comparative method described by Strauss and Corbin (1990). Each segment of the written responses to the open- ended questions was coded independently by both authors to identify and name major themes. Once a list of major themes was developed, content analysis (Patton, 2002) was used to deter- mine how frequently each theme was mentioned by respondents. RESULTS In this section, each research question is addressed in turn. When qualitative data gene- rated noteworthy themes, the themes are identified and quotes provided for illustration. Do FPs View MFTs as a Resource for Patients With
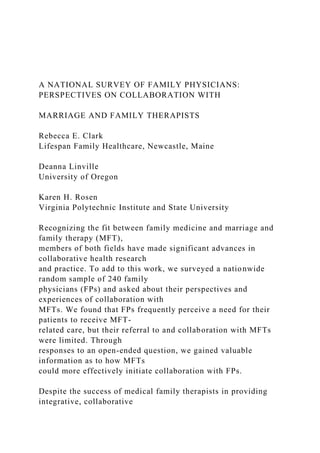
- 10. Psychosocial Needs? This research question was addressed by five questions on our questionnaire. Respondents were asked to estimate the percentage of their patients with identified psychosocial concerns who they believed could benefit from marital and ⁄ or family therapy. Respondents were also asked to estimate their referral practices. On average, respondents estimated that 48% of their patients could benefit from marital and ⁄ or family therapy and that they referred 12% of their patients for mental health services. However, respondents estimated that they referred 5% of their patients specifically for marital and ⁄ or family therapy– related care. We specified marital and ⁄ or family therapy–related care rather than MFT because at that time several states did not license MFTs (three of the states represented in this survey did not). Additionally, respondents were asked to check all that applied from a list of potential roadblocks encountered when referring patients for MFT-related care. As can be seen in Figure 1, ‘‘Patient reluctance’’ was checked by 85% of the respondents, ‘‘HMO ⁄ Insurance’’ by 65%, ‘‘unavailability of appropriate therapists’’ by 40%, ‘‘time’’ by 34%, ‘‘lack of awareness of appropriate therapists’’ by 33%, and ‘‘don’t feel this type of therapy is helpful’’ by 4%. Although 24 respondents provided written answers in response to ‘‘other please specify,’’ no new categories of roadblocks to referral emerged. Figure 1. Roadblocks encountered by FPs when referring
- 11. patients for marriage and family therapy–related care (n = 136). April 2009 JOURNAL OF MARITAL AND FAMILY THERAPY 223 Finally, respondents were asked if they were aware that MFTs are licensed mental health professionals ‘‘trained in psychotherapy and family systems and licensed to diagnose and treat mental and emotional disorders within the context of marriage, couples, and family systems.’’ While 83% of respondents checked ‘‘yes’’ to this question, 64% reported that prior to receiving our survey they did not recognize the initials ‘‘LMFT’’ as credentials for a Licensed Marriage and Family Therapist. Are FPs Interested in Collaborating With MFTs? This research question was addressed by five questions on our questionnaire. Respondents were asked, ‘‘Have you ever consulted with a mental health professional regarding a patient case?’’ All of the respondents checked ‘‘yes’’ to this question. When respondents were asked whether or not they had ever consulted with an LMFT regarding a patient or family, 47% of the respondents checked ‘‘yes,’’ while 53% of the respondents indicated they either had not or were not sure if they had consulted with an LMFT. Additionally, respondents were given a list of collaborative modes and asked to check all
- 12. that applied to their experience of collaborating with MFTs or comparable mental health pro- fessionals in their community. ‘‘Infrequently receive reports’’ was checked by 49% of the FPs, ‘‘phone call ⁄ email with a MFT’’ by 43%, ‘‘informal consultation with a MFT’’ by 40%, ‘‘no patient-care contact with MFTs’’ by 20%, ‘‘regularly receive reports’’ by 19%, and ‘‘regular meetings with MFTs’’ by 3%. Respondents were asked to describe how helpful they found patient-care consults with MFTs. The collaborative interactions with MFTs were indicated by 82% of the respondents to be either ‘‘very helpful’’ or ‘‘somewhat helpful.’’ Five percent checked either ‘‘somewhat unhelpful’’ or ‘‘very unhelpful,’’ while 12% checked ‘‘not applicable.’’ Finally, respondents were asked to describe their interests in collaborating with LMFTs or comparable mental health professionals when identifying patients’ psychosocial needs by check- ing all that applied from a list of collaborative approaches. The mode of collaboration pre- ferred by most of the respondents was ‘‘referral out with continuing collaborative communication’’ (84%). Some respondents also indicated that they would be interested in ‘‘inviting a family therapy provider to a patient’s appointment’’ (15%) or ‘‘meeting regularly with a MFT regarding complex patients’’ (11%). Only 7% of the respondents indicated they were ‘‘not interested’’ in collaborating with MFTs. What Would Make MFTs More Helpful Collaborators?
- 13. This research question was addressed by an open-ended question. Respondents were asked to ‘‘briefly describe what would make MFT providers a more helpful resource when treating patients with psychosocial issues, OR if you don’t consult with an MFT, why not?’’ Eighty-nine respondents (65% of sample) answered this question, offering a total of 141 coded responses. A content analysis produced six primary themes: (a) ideal collaborative practices, (b) barriers to referral, (c) MFT specialty awareness, (d) let us know who you are, (e) barriers to collaboration, and (f) attitudes toward MFTs. Quotes are included to better illustrate the themes and subthemes. Ideal collaborative practices. Fifty-four responses were coded as relating to collaborative practices that would make MFTs more helpful resources. These included proximity (‘‘I wish I had a family therapist in my office’’), ease of referral (‘‘Be available to my patients within 2 weeks of the request’’), collaborative communication (‘‘More communication after [patient] evaluation,’’ ‘‘Regular feedback’’), topical ⁄ specialty information (‘‘Suggestions on what I can do to help further the therapeutic goals,’’ ‘‘A specialist who could incorporate issues related to aging’’), and religious ⁄ faith-based (‘‘Faith-based, a plus!’’ ‘‘I would like to work with a Christian marriage and family therapist’’). 224 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009
- 14. Barriers to referral. We coded 33 comments as barriers respondents face when making referrals to MFTs, including patient reluctance (‘‘Difficulty convincing patients that therapy can help them and sometimes even that there is a problem’’), managed care (‘‘Many patients don’t have mental health coverage,’’ ‘‘I do use other therapists when driven by insurance’’), do not know the therapist (‘‘hard to refer when don’t know therapist’’), and lack of availability (‘‘Ther- apists not available in my rural area,’’ ‘‘If one were more readily available, this would be an excellent resource’’). Only one of the responses indicated that the respondent encountered no barriers to referral. MFT specialty awareness. We coded 15 responses as relating to respondents’ awareness of MFT as a specialty. Many of these respondents indicated they were either completely unaware of MFT as a distinct field or were unclear about the professional role of an MFT (‘‘I didn’t know there was a family ⁄ marriage therapy specialist’’). Other respondents asked for more infor- mation about MFTs and the types of services they provide. Some indicated that they had not differentiated between the various mental health professionals with whom they worked (whether they be MFTs, social workers, or psychologists). Let us know who you are. We coded 14 responses as indicating respondents wanted to be able to identify the MFTs in their communities. Responses placed in this category suggested
- 15. that respondents were either unaware of MFTs, had no professional contact with MFTs in their communities, or were less likely to work with therapists they had not met (‘‘Probably meeting face to face [would be helpful]’’). Barriers to collaboration. We coded 13 responses as describing barriers to collaboration. Subcategories of this theme are the following: time (‘‘Unfortunately we seem to have less time to [collaborate]’’), managed care (‘‘HMO . . . typically listed an 800# to call . . . made commu- nication very difficult between the anonymous therapist and I’’), lack of therapist feedback (‘‘Helpful to get reports back from therapists, but it often doesn’t happen’’), and interest (‘‘I like to refer but don’t necessarily feel I need to receive reports’’). Attitudes toward MFTs. We coded 12 responses as relating to FPs’ attitudes regarding MFTs. Seven responses had positive overtones (‘‘They are already a helpful resource for me—I can’t think of any way to improve this presently’’). Two responses suggested an uncertain or even negative mind-set toward MFTs (‘‘most of the MFT people only have a Master’s . . . for more complex cases, I might choose psychiatry or doctoral psychology background’’). Three responses made reference to the importance of a philosophical fit. DISCUSSION The primary theme emerging from this study is that FPs are interested in referral and col-
- 16. laboration, in some form, but face barriers. This theme is illustrated by the quantitative and qualitative data. The data suggest that there is a considerable gap between the percent of patients FPs identified as potentially needing MFT (48%) and the percent of patients actually referred for MFT (5%). This may, in part, be understood by the roadblocks to referral (e.g., patient reluctance, HMO restrictions, unavailability of appropriate therapist, and time) faced by FPs in this study as well as in previous research studies (Kainz, 2002; Orleans, George, Houpt, & Brodie, 1985; Rosenthal, Shiffner, & Panebianco, 1990; Rost et al., 1994; Williams et al., 1999). Secondly, FP respondents in this study reported that they are often unaware of MFTs in their community or unfamiliar with the discipline of MFT. Likewise, Kainz (2002) found that physicians would be more likely to refer to the mental health providers with whom they had met and developed a good relationship or of whom they had heard a good report from either colleagues or patients. It may be that FPs are also uncertain of the scope of MFTs’ training and practice. April 2009 JOURNAL OF MARITAL AND FAMILY THERAPY 225 Thirdly, the FPs in this study appeared receptive to referring to and collaborating with MFTs, but collaboration is limited in its occurrence. In this
- 17. study, HMOs, time limitations, and lack of therapist-initiated communication have been identified as significant barriers to col- laboration. These barriers that were identified by FPs are similar to the collaboration barriers identified by MFTs. Research articles and books written on collaboration give considerable attention to the issues around HMO-related barriers (e.g., DeGruy, 1997; McCulloch et al., 1998; Seaburn et al., 1996). Other potential barriers to collaboration may be attributed to patient reluctance to accepting a mental health referral. Reust et al. (1999) found that patient- identified barriers to following through with a physician- initiated mental health referral are comparable to the barriers identified by FPs in this study. Finally, FP respondents reported that they want feedback from MFTs to whom they refer a patient. This finding is consistent with the findings of other studies on collaboration (Kainz, 2002; Rosenthal et al., 1990; Rosenthal, Shiffner, Lucas, & DeMaggio, 1991) which have identi- fied regular feedback to be essential, with the majority describing this feedback ideally to be a brief intake report or progress note. With these themes in mind, we make suggestions for enhancing collaboration between FPs and MFTs. Suggestions for MFTs Specific training in MedFT will facilitate MFTs’ ability to collaborate and provide compre- hensive, biopsychosocial care in conjunction with a client’s FP or other medical practitioner (McDaniel et al., 1992a). As with any relationship, it is
- 18. important to take a learning stance in order to begin forging collaborative relationships with FPs. Researchers and practitioners in healthcare collaboration underscore the importance of understanding how the cultural and structural differences between the two professions present unique challenges for collaboration (McDaniel et al., 1992a; Patterson, Peek, Heinrich, Bischoff, & Scherger, 2002). Knowledge of the culture of family medicine or other medical specialties will add to MFTs’ abilities to approach collaboration with sensitivity and confidence. To build mutual respect, MFTs should communicate a desire to understand the needs of FPs and their patients. Overall, constant investments of time, communication, respect, and goal clarification are important for develop- ing successful collaborative relationships (McDaniel et al., 1992a; Seaburn et al., 1996). We found that some FPs are either unaware of MFT as a unique discipline within the mental health field or unaware of MFTs’ availability in their community. In response to this finding, MFTs might introduce themselves to local FPs, especially those whose patients they are already counseling. Recognizing that it may be intimidating to make the initial contacts, McDaniel et al. (1992a) suggested finding venues for introduction such as through another medical colleague or inviting the medical practitioner to lunch. At this time it may be helpful to offer a business card, rolodex insert, and brochure describing areas of specialty in order to facilitate future contact or referral from the FP.
- 19. As MFTs learn about the types of patient psychosocial concerns that FPs commonly encounter, it may be helpful to create fact sheets addressing these concerns, offer brief work- shops, or even participate on grand rounds in local hospitals. FPs in this study suggested that information on specific psychosocial issues would be helpful. They most commonly requested suggestions for reducing patient reluctance to MFT care. MFTs might consider American Asso- ciation for Marriage and Family Therapy (AAMFT) brochures addressing specific mental health issues as a resource to offer FPs or referred patients. These brochures have a space for professional contact information and are available for purchase from AAMFT (see http:// www.aamft.org/store/shop/category.asp?catid=9). Also, MFTs can regularly participate on healthcare teams by obtaining releases from clients to exchange information with the referring physician. If a client declines to release his or her information, the MFT may want to send a brief note acknowledging and thanking the FP for the referral and discuss with the client the goals and potential benefits of a team approach. 226 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009 Beyond the routine collaborative communication, MFTs can look for ways to maintain con- tact and develop the relationship. For instance, MFTs might locate current journal articles or other brief materials for FPs that may pertain to collaboration,
- 20. mental health issues, or behavioral health techniques. Due to the demands of patient care, FPs have limited time for researching issues in mental health and may appreciate this collaborative gesture (E. Ng, MD, personal communication, December 3, 2003). Experienced collaborators underscore the importance of the long-term efforts necessary to maintain collaborative relationships. MFTs may also be interested in joining a collaborative healthcare organization such as the CFHA (which includes a subscrip- tion to the journal Families, Systems, and Health) or participating in other like-minded events such as the Conference on Families and Health sponsored by the STFM and CFHA. Implications for Clinical Training and the MFT Field Professionals in the field of MFT must continue to look for ways to bridge the gap between these two compatible fields. Based on our findings, it seems that MedFT and collabo- rative training programs offer skills necessary to collaborate with FPs in comprehensive, systemic care. These trainings are offered in academic settings, in fellowship training programs, professional associations, professional journals, and community interactions (for information on training programs, see www.cfhcc.org/pages/education-and- training/; see also a list of pro- grams in Seaburn et al., 1996, pp. 270–272). It may be necessary for MFT training programs to add collaboration training or MedFT to their curriculum. William Doherty (personal communi- cation, March 22, 2003) stated that professionals most often collaborate with whom they train
- 21. or know personally. Since most MFTs do not have the opportunity to know FPs personally, a collaborative component early in MFT training would offer an opportunity for students to interact with health professionals from other disciplines and for medical health professionals in the community to learn about MFT and meet future MFTs. Students could be encouraged to seek internships in medical settings or to conduct research relevant to both fields and to publish in family medicine journals. Numerous associations (such as the AAFP, AAMFT, Health Psychology Division of the American Psychology Association, CFHA, and STFM) offering workshops and conferences provide additional opportunities for MFTs and FPs to interact and increase their collaboration skills. As MFTs learn to connect with FPs, it is possible that MFTs and FPs will find ways to work together to promote marketing and to advocate for managed care policy change. Man- aged care corporations may respond to pressure placed on them by organized, collaborating FPs and MFTs to ensure reimbursement for mental healthcare. Limitations When interpreting the results of the study, it is important to be mindful of the following limitations. First, the questionnaire has not been tested for reliability or validity. While the sur- vey method is an efficient mode for data collection, questionnaires are self-administered tools in uncontrolled settings. Thus, it is possible for the participants to misinterpret questions. To
- 22. address these limitations, this survey was scrutinized by several FPs, and qualitative questions were included to add depth and clarity to the findings. Secondly, although the size of our sample is sufficient to produce a confidence interval of about ±6% (Rea & Parker, 1997), it is still a relatively small sample compared to a population of over 53,000 FPs. Readers are encouraged to consider the margin of error when interpreting results. However, this study’s response rate (64%) is remarkable when compared with physician response rates to other surveys with and without incentives (VanGeest, Wynia, Cummins, & Wilson, 2001). Suggestions for Future Research More research is needed to enhance our understanding of what increases the likelihood of successful collaboration between FPs and MFTs. One approach to this may be for researchers April 2009 JOURNAL OF MARITAL AND FAMILY THERAPY 227 to examine collaborative relationships that are working. What types of training in an MFT program or FP residency are linked to increased collaboration? What current practices of col- laboration are most effective and why? Additionally, another member of the collaborative triad, the patient, could be a valuable source of information about the helpfulness of FP ⁄ MFT col- laboration. The patient’s perspective of the risks ⁄ benefits of
- 23. his or her FP and MFT working together may be useful in establishing a link between psychosocial care and cost-effective healthcare that would interest managed care companies. Despite the barriers and limitations to FP ⁄ MFT collaboration identified in this study, our findings suggest that FPs think many of their patients could benefit from MFT and are inter- ested in collaborating with MFTs. It is our hope that this study will encourage interdisciplinary discussion that continues to bridge the gap between FPs and MFTs and ultimately promote more effective care for the patient ⁄ client. REFERENCES American Academy of Family Physicians (2000). Skills. Human behavior and mental health. Retrieved February 3, 2004, from http://www.aafp.org/x16550.xml. Updated February 7, 2009, from http://www.aafp.org/online/ etc/medialib/aafp_org/documents/about/rap/curriculum/mentalh ealth.Par.0001.File.tmp/Reprint270.pdf American Academy of Family Physicians (2003). Membership in the American Academy of Family Physicians, January 1, 2002 (Tables 134, 135). Retrieved March 23, 2003, from http://www.aafp.org/x950.xml and http://www.aafp.org/x949.xml. Current census data available at http://www.aafp.org/online/en/home/ aboutus/specialty/facts.html
- 24. Bader, E. (1990). Working with families. Australian Family Physician, 19, 525–527. Bloom, M., & Smith, D. (2001). Brief mental health interventions for the family physician (1st ed.). New York: Springer-Verlag. Bullock, D., & Thompson, B. (1979). Guidelines for family interviewing and brief therapy by the family physi- cian. Journal of Family Practice, 9, 837–841. Burns, L. H. (1999). Genetics and infertility: Psychosocial issues in reproductive counseling. Families, Systems & Health, 17, 87–110. Campbell, T. L., & Patterson, J. M. (1995). The effectiveness of family interventions in the treatment of physical illness. Journal of Marital & Family Therapy, 21, 545–583. Christie-Seely, J. (1981). Teaching the family system concept in family medicine. Journal of Family Practice, 13, 391–401. Chung, M. K. (1996). Editorials: Why alternative medicine? American Family Physician, 54, 773–779. Dare, C., & Eisier, I. (1995) Family therapy. In G. Szmuller & C. Dare (Eds.), Eating disorders (pp. 333–349). Chichester, England: Wiley.
- 25. Davis, C. (1988). Family therapy. The Practitioner, 232, 1377– 1378. DeGruy, F. (1997). Mental health care in the primary care setting: A paradigm problem. Family Systems and Health, 15, 3–26. Doherty, W. J., & Baird, M. (1983). Family therapy and family medicine: Towards the primary care of families. New York: Guilford. Dym, B., & Berman, S. (1986). The primary health care team: Family physician and family therapist in joint practice. Family Systems Medicine, 4, 9–21. Fischetti, F., & McCutchan, F. (2002). A contextual history of the behavioral sciences in family medicine revis- ited. Families, Systems & Health, 20, 113–129. Fisher, L., & Ransom, D. C. (1997). Developing a strategy for managing behavioral health care within the context of primary care. Archives of Family Medicine, 6, 324– 333. Flodmark, C. E., Ohlsson, T., Ryden, O., & Sveger, T. (1993). Prevention of progression to severe obesity in a group of obese schoolchildren treated with family therapy. Pediatrics, 5, 880–884.
- 26. Fosson, A. R., Elam, C. L., & Broaddus, D. A. (1982). Family therapy in family practice: A solution to psycho- social problems? Journal of Family Practice, 15, 461–465. Frank, S. H. (1985). The unit of care revisited. Journal of Family Practice, 21, 145–148. Gerdes, J. L., Yuen, E. J., & Frey, C. M. (2001). Assessing collaborative patterns and strength between primary care and mental health providers. Families, Systems & Health, 19, 429–444. 228 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009 Glied, S. (1998). Too little time? The recognition and treatment of mental health problems in primary care. Health Services Research, 33(4 Pt. 1), 891–910. Retrieved February 7, 2009, from http://www.pubmedcentral. nih.gov/pagerender.fcgi?artid=1070292&pageindex=1#page Harkness, J. L., & Nofziger, A. (1998). Medical family therapy casebook. Training in a collaborative context: What we did not know then . . . we know now. Families, Systems & Health, 16, 443–450. Hepworth, J., & Jackson, M. (1985). Health care for families: Models of collaboration between family therapists
- 27. and family physicians. Family Relations, 34, 123–127. Jackson, L., & Tisher, M. (1996). Family therapy for general practitioners. Australian Family Physician, 8, 1269– 1271. Kainz, K. (2002). Barriers and enhancements to physician- psychologist collaboration. Professional Psychology: Research and Practice, 33, 169–175. Kushner, K., Diamond, R., Beasley, J. W., Mundt, M., Plane, M. B., & Robbins, K. (2001). Primary care physi- cians’ experience with mental health consultation. Psychiatric Services, 52, 838–840. Lang, F., Marvel, K., Sanders, D., Waxman, D., Beine, K. L., Pfaffly, C., et al. (2002). Interviewing when family members are present. American Family Physician, 65, 1351– 1354. Mayer, R., Graham, H., Schuberth, C., Launer, J., Tomson, D., & Czauderna, J. (1996). Family systems ideas in the 10-minute consultation: Using a reflecting partner or observing team in a surgery. British Journal of General Practice, 46(405), 229–230. McCulloch, J., Ramesar, S. & Peterson, H. (1998). Psychotherapy in primary care: The BATHE technique. Amer- ican Family Physician, 57, 2131–2134. Available at
- 28. http://www.aafp.org/afp/980501ap/mcculloch.html McDaniel, S., Hepworth, J., & Doherty, W. J. (1992a). Medical family therapy: A biopsychosocial approach to families with health problems. New York: Basic Books. McDaniel, S., Hepworth, J., & Doherty, W. J. (1992b). Medical family therapy with couples facing infertility. American Journal of Family Therapy, 20, 101–122. McDaniel, S. H., Hepworth, J., & Doherty, W. J. (1995). Commentary. Medical family therapy with somaticizing patients: The co-creation of therapeutic stories. Family Process, 34, 349–361. Moon, J. R. (1997). Partnerships with primary care physicians: Reinventing gatekeeper relationships. In N. A. Cummings, J. L. Cummings, & J. N. Johnson (Eds.), Behavioral health in primary care: A guide for clinical integration (pp. 305–323). Madison, CT: Psychosocial. Norusis, M. J. (2000). SPSS 10.0 guide to data analysis. Englewood Cliffs, NJ: Prentice Hall. Orleans, C. T., George, L. K., Houpt, J. L., & Brodie, H. K. (1985). How primary care physicians treat psychiat- ric disorders: A national survey of family practitioners. American Journal of Psychiatry, 142, 52–57. Patterson, J., Peek, C. J., Heinrich, R. L., Bischoff, R. J., &
- 29. Scherger, J. (2002). Mental health professionals in medical settings: A primer. New York: W.W. Norton. Patton, M. Q. (2002). Qualitative research and evaluation methods. Thousand Oaks, CA: Sage. Rea, L. M., & Parker, R. A. (1997). Conducting survey research: A comprehensive guide. San Francisco: Jossey- Bass. Reust, C. E., Thomlinson, R. P., & Lattie, D. (1999). Keeping or missing the initial behavioral health appoint- ment: A qualitative study of referrals in a primary care setting [Electronic version]. Families, Systems & Health, 17, 399–411. Rolland, J. S. (1994). Families, illness, and disability: An integrative treatment model (pp. 127–164). New York: Basic Books. Rosenthal, T. C., Shiffner, J. M., Lucas, C., & DeMaggio, M. (1991). Factors involved in successful psychother- apy referral in rural primary care. Family Medicine, 23, 527– 530. Rosenthal, T. C., Shiffner, J., & Panebianco, S. (1990). Physician and psychologist beliefs influencing referral of patients for psychotherapy. Family Medicine, 22, 38–41.
- 30. Rost, K., Humphrey, J., & Kelleher, K. (1994). Physician management preferences and barriers to care for rural patients with depression. Archives of Family Medicine, 3, 409– 414. Schurman, R., Kramer, P., & Mitchell, J. B. (1985). The hidden mental health network: Treatment of mental illness by nonpsychiatrist physicians. Archives of General Psychiatry, 42, 89–94. Seaburn, D. B., Lorenz, A. D., Gunn, W. B., Jr., Gawinski, B. A., & Mauksch, L. B. (1996). Models of collabo- ration: A guide for mental health professionals working with health care practitioners (1st ed.). New York: Basic Books. Strauss, A. L., & Corbin, J. M. (1990). Basics of qualitative research. Grounded theory: Procedures and techniques. Newbury, CA: Sage. April 2009 JOURNAL OF MARITAL AND FAMILY THERAPY 229 Tomson, P. R. V., & Asen, E. (1987). Can general practitioners be taught family therapy methods? Family Systems Medicine, 5, 97–104. VanGeest, J. B., Wynia, M. K., Cummins, D. S., & Wilson, I. B.
- 31. (2001). Effects of different monetary incentives on the return rate of a national mail survey of physicians. Medical Care, 39(2), 197–201. Available MFTP: Hostname: vt.edu Directory: Ovid Citations. Weihs, K., Fisher, L., & Baird, M. (2002). Families, health and behavior—a section of the commissioned report by the committee on health and behavior. Families, Systems and Health, 20, 7–57. Williams, J. W., Rost, K., Dietrich, A. J., Ciotti, M. C., Zyzanski, S. J., & Cornell, J. (1999). Primary care physi- cians’ approach to depressive disorders: Effects of physician specialty and practice structure. Archives of Family Medicine, 8, 58–67. Yeager, B., Auyand, M., Brown, D. L., Dickinson, P., Goldstein, J. A., Jaffe, N., et al. (1999). MFT student training in medical family therapy: A collaborative hospital project with radiation oncology. Families, Systems & Health, 17, 427–436. 230 JOURNAL OF MARITAL AND FAMILY THERAPY April 2009
- 32. TRAINING FOR COLLABORATION: COLLABORATIVE PRACTICE SKILLS FOR MENTAL HEALTH PROFESSIONALS Richard J. Bischoff, Paul R. Springer, Allison M. J. Reisbig University of Nebraska-Lincoln Sheena Lyons Devereux Adriatik Likcani Kansas State University The purpose of the study was to identify skills that mental health practitioners need for successful collaborative practice in medical settings. Known experts in the field of collabo- rative health care completed a survey designed to elicit their suggestions about what is needed for successful collaborative care practice. Through qualitative analysis, a set of 56 skills was developed. These skills are organized into three general categories of compe- tency: (a) skills for working in a medical setting; (b) skills for working with patients; and (c) skills for collaborating with healthcare providers. In their landmark text, Medical Family Therapy, McDaniel, Hepworth, and Doherty (1992) introduced an approach to health care delivery based on the Engel’s (1977) biopsychosocial (BPS) model. The foundation of medical family therapy (MedFT) is an acknowledgment that ‘‘all human problems are BPS systems problems: there are no
- 33. psychosocial problems without biological features and no biomedical problems without psychosocial features’’ (McDaniel et al., 1992, p. 26). The authors reasoned that treatments will be more effective and outcomes more positive when biological and psychosocial dimensions of functioning are considered and addressed simultaneously. This is facilitated by maximizing the collaboration between physi- cians and mental health therapists. While the scholarship of the practice of collaborative health care predates the publication of this text, it has increased dramatically since 1992. Other texts promoting the practice of MedFT have been written (e.g., Blount, 1998; Patterson, Peek, Heinrich, Bischoff, & Scherger, 2002; Prouty-Lyness, 2003; Seaburn, Lorenz, Gunn, Gawinski, & Mauksch, 1996), giving stu- dents of the approach a library of literature on the practice. While started in 1983, the journal Families, Systems, and Health has since become a premiere journal in this specialty area of mental health care. Research has established the link between biological, social, and psychologi- cal systems (see Campbell & Patterson, 1995) and the positive impact of psychotherapy, espe- cially relational approaches to treatment, on health outcomes (Cambell, 1996; Crane & Christenson, 2008; Law, Crane, & Berge, 2003). The Collaborative Family Healthcare Associa- tion, an association devoted to collaborative care practices that are characteristic of MedFT, has matured into a multidisciplinary association giving those interested in collaborative care practices a place to come together to share ideas and advance
- 34. the practice, research, and theory of medical family therapy (Bloch & Doherty, 2001). It would be difficult to imagine that one could graduate from a clinical training program in marriage and family therapy, psychology, or Richard J. Bischoff, PhD, is a Professor and Director in the Marriage and Family Therapy Program at University of Nebraska-Lincoln; Paul R. Springer, PhD and Allison M. J. Reisbig, PhD, are Assistant Professors in the Marriage and Family Therapy Program at University of Nebraska-Lincoln; Sheena Lyons, MS, Devereux, Arizona; Adriatik Likcani, MS, is a Doctoral candidate in the Marriage and Family Therapy Program at Kansas State University. Address correspondence to Richard J. Bischoff, Marriage and Family Therapy Program, University of Nebraska-Lincoln, PO Box 830800, Lincoln, Nebraska 68583- 0800; E-mail: [email protected] Journal of Marital and Family Therapy doi: 10.1111/j.1752-0606.2012.00299.x June 2012, Vol. 38, No. s1, 199–210 June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY 199 social work without an understanding of the BPS model, collaborative care practice, and Med-
- 35. FT. However, even with the existence of several degree granting and postdegree training pro- grams in MedFT and many more programs that have emphases in medical family therapy and collaborative health care, little is known about the competencies needed to practice MedFT. It is clear from reading any of the several texts on the subject that MedFT is different from the traditional mental health care practice. Those practicing MedFT need to have the same skills that are needed for traditional practice environments as well as many other skills unique to the collaborative health care environment. However, as yet, these skills have not been orga- nized nor explicitly identified. The development of a succinct set of skills, similar to that of the American Association for Marriage and Family Therapy (AAMFT) core competencies (Nelson et al., 2007), would be a step in the direction of developing training and practice guidelines for this rapidly developing approach to health care. This is particularly important in this age of outcomes-based educational standards (Maki, 2004; Miller, Todahl, & Platt, 2010; Nelson et al., 2007). The purpose of this study was to develop a set of skills that would aid educators and train- ers interested in preparing mental health therapists for practice in collaborative health care set- tings. This was achieved through a qualitative design that began with inductive qualitative inquiry with leaders of collaborative care practice in an effort to understand the competencies that mental health therapists need to work effectively in
- 36. collaborative health care settings. METHODOLOGY Participants After receiving Institutional Review Board approval, a purposive sampling strategy was used to invite experts in MedFT to participate in this study. To be identified as an expert, indi- viduals had to meet one of the following criteria: (a) the person was an author on a minimum of two peer-refereed journal articles directly related to collaborative care practice or training or (b) the person was identified as an expert by someone meeting the two publication criterion. The first criterion allowed for the inclusion of those identified as experts because they were advancing the field through publication. The second criterion allowed for the inclusion of prac- titioners who have influence on the development of the practice of MedFT through clinical practice. Thirty-three experts were invited to participate, and 25 contributed data for the study (a response rate of 76%). Sixty percent of the participants were men and 80% were over 35 years old. Sixty-eight percent reported that they had more than 5 years of experience work- ing collaboratively in a medical setting practicing the principles identified in the research, and 24% reported more than 15 years of experience. Sixty percent reported their primary place of employment as a medical setting (11 respondents worked in a medical residency program, three in a medical school, and one in a primary care medical setting). The remainder reported that
- 37. their primary employment setting was a university-based mental health training program. Fif- teen respondents identified their primary professional affiliation as MFT. Other respondents were primary care physicians (5), psychiatrists (2), psychologists (2), and one nurse. Survey A survey consisting of 13 questions was developed for the purposes of this study. Six open- ended questions were designed to elicit skills needed for successful collaborative practice. These questions elicited data about knowledge (biomedical and mental health) and clinical skills needed for successful practice in medical settings. Participants were also asked to relate an inci- dent that exemplifies successful medical, mental health collaboration. Six closed-ended questions elicited demographic information. The final question requested that the respondent identify oth- ers who they would consider to be experts on collaborative care practice and who might be able to provide useful information. In an effort to facilitate participation, participants either could choose to complete the survey on-line through a secure, password-protected website or through a paper version that was mailed to them. Potential respondents were contacted both by email (if an email address was available) and by a letter sent via US mail requesting participation in the survey. 200 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012
- 38. Data Analysis Data were initially analyzed using a process similar to the constant comparison qualitative data analysis method (Miles & Huberman, 1994) by the primary researcher and a research assistant. Using this method, content analyses were performed, and a preliminary codebook of themes or skills was inductively identified. Specifically, each participant’s response was read in its entirety to understand the skills being emphasized by each respondent. Each reader kept a list of skills that emerged from the data. They then met to review and compare their separate lists and come up with a consensus list. No skills identified by readers were eliminated from the list. Both the primary researcher and the research assistant then separately returned to the data to carefully examine the responses to each question. All responses to question number one were read, identifying support for the skills identified on the list and adding new skills to the list by comparing incidents in the data with all others. Question number two was then analyzed simi- larly, and so on. Subsequent responses were compared with those preceding them in the analy- sis, with the result being the addition of new skills or the addition of evidence for skills already noted, as appropriate. The validity, or substantive significance, of the data was established through analyst trian- gulation (Patton, 2002). Using a deductive method, three secondary coders reviewed and vali-
- 39. dated the presence and salience of each theme identified by the primary coder and his research assistant. Skills that lacked clear support in the data were discussed and compared with all other skills that had been identified. This process helped establish the validity of the primary researcher’s and the graduate assistant’s preliminary coding of the data. The primary researcher and secondary coders then collapsed and sorted each theme or skill into categories and subcate- gories. The result of this process ensured that all categories and subcategories were examined and agreed upon by all coders. In addition, this process ensured that the interpretation of the data was comprehensive and accurate. RESULTS Qualitative analysis of the survey responses resulted in a set of 56 skills that uniquely char- acterize MedFT. It is evident from the data that while the practice of MedFT includes compe- tence in the practice of psychotherapy, it also includes skills unique to working in medical settings and to collaborating with medical providers and other professionals. Consequently, the identified skills have been clustered into three categories that represent logical groupings of these skills: (a) skills for working in a medical setting; (b) unique skills for working with patients in medical settings; and (c) skills for collaborating with healthcare providers. Skills within each category are further broken down into subcategories. The skills are presented by category in Tables 1–3. Each category is described below.
- 40. Skills for Working in a Medical Setting Participants were careful to explain that working in medical settings is different from work- ing in traditional mental health practice settings. In describing this difference, one respondent explained that the medical setting is ‘‘a fast paced environment that has an organizational structure entrenched in traditional biomedical influence.’’ Others created lists such as: ‘‘differ- ences in language, pace, communication styles, confidentiality expectations, team roles, and documentation.’’ Differences such as these require those practicing MedFT to demonstrate competence in working within this unique practice environment. These skills can be organized according to those relating to (a) the unique practice culture of the medical setting, (b) medical knowledge, (c) accommodating to the medical setting, and (d) nurturing one’s professional identity. The unique practice culture of the medical setting. When stepping into a medical setting, one is stepping into a unique culture; one that is different from traditional mental health care practice. Those practicing MedFT recognize this work to understand the culture, and to prac- tice in culturally sensitive ways. One respondent counseled that ‘‘It is important for the mental health professional to recognize that he or she is entering a different culture.’’ Another respon- dent explained that ‘‘a medical setting is part of the culture of medicine. It has a language, a June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY
- 41. 201 history, a set of shared myths and archetypes like any culture.’’ The data suggest that it is par- ticularly important for mental health therapists to attend to the following characteristics of this unique culture. Language. Respondents explained that the language of medical settings has been devel- oped to facilitate the work of medicine and that this language is unique and different from that found in traditional mental health care settings. One respondent explained, Bridging the language barrier is [important]. Many MHPs [Mental Health Providers] enter into a medical setting speaking therapy and not understanding medicalease. [Developing a common language] means abandoning the terms that we learned in graduate school for more user friendly words that medical professionals understand. Another respondent explained that ‘‘The language is instrumental and action oriented. [It] mirrors the kind of expectations that the [medical provider] may have of mental health provid- ers (what can you do rather than what do you think).’’ Another respondent succinctly wrote that there is a ‘‘preference for concreteness over abstractions.’’ The importance of the language used applies equally to verbal and written (e.g., charting) communication. Several respondents
- 42. explained that mental health therapists ‘‘should understand the abbreviations for medication Table 1 Skills for Working in a Medical Setting The unique practice culture of medical settings Medical family therapists . . . Recognize that medical settings have a unique practice culture Recognize and respect the professional hierarchy in medical settings Respect the differences between medical and mental health providers in scope of practice, practice patterns and strategies, approach to patient care, etc. Know the difference between primary, secondary, and tertiary care Respect and value the contributions of the biomedical approach to care Are curious and willing to learn about unfamiliar, new, and nontraditional approaches to healing and promoting wellness Know the services that are available and how to utilize them Are visible within the medical environment as an active participant of the care team Medical knowledge Medical family therapists . . . Speak the language of the medical setting (e.g., medical terms, abbreviations, jargon) Access and use medical and pharmacological information from reliable sources
- 43. Know the diagnostic tests and treatments that are commonly used for patient medical care Accommodations to the medical setting Medical family therapists . . . Match the pace of the medical setting Are comfortable with frequent interruptions by medical staff during treatment sessions Are flexible in working with patients and families in examination rooms and other nontraditional settings Accommodate to how confidentiality is handled in medical settings Document patient progress consistent with medical setting protocols Have the ability to be an excellent short-term interventionist Nurturing professional identity Medical family therapists . . . Are willing to be shaped in professional identity and role Stay connected with mental health colleagues 202 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012 (e.g., QID, QD, PO)’’ and should be able to document psychotherapy consistent with medical charting protocols and in a way that will make this information useful to medical providers.
- 44. Time management. It is important to attend to the pacing of the medical setting and in how medical providers manage time with patients. One respondent explained that ‘‘MDs [Medical Doctors] carry a case load of several thousand and see a minimum of [four] patients per hour.’’ Another explained that ‘‘The medical clinician is usually working with [two] patients at one time.’’ This use of time can be disconcerting for the naı̈ ve mental health therapist. But, echoing the sentiment of others, one respondent wrote, ‘‘MDs must be action oriented. This time crunch should never be interpreted as evidence that the MD does not care about his ⁄ her patients.’’ The team approach to patient care. Contrary to the independence and autonomy that are hallmarks of traditional mental health practice, treatment in medical settings is typically charac- terized by a team approach where health care providers from various specialties and disciplines work together in caring for a patient. There are two noteworthy consequences of this approach for mental health therapists. First, the mental health care is often not the primary focus of the treatment. As one part of the overall care plan, the mental health treatment must support and complement the other parts of the care plan, some of which have greater immediacy and demand more attention than the mental health concerns. Second, the therapist may not occupy a primary role in direct patient care and may at times not even see the patient. There is a Table 2
- 45. Skills for Working with Patients The practice lens Medical family therapists . . . Conceptualize pathology from the biopsychosocial perspective Medical knowledge Medical family therapists . . . Have a basic understanding of biochemical processes and pharmacology Have a basic understanding of anatomy and physiology Know about the biological processes of diseases Know the medical conditions that commonly have psychosocial comorbidity Know mental health conditions that commonly manifest through physical symptoms Know common psychiatric medications, names and abbreviations, doses, and side effects Patient care Medical family therapists . . . Are skillful in working with a wide variety of treatment modalities (e.g., couple, family, individual, group) Assess and diagnose mental disorders using the current DSM and ICD Provide patient psychoeducation in both individual and group formats Engage patients who do not see the connection between their medical conditions and other areas of functioning Respond to a wide range of patient responses to illness and
- 46. medical treatment Organize and conduct family meetings Know when and how to effectively intervene in the physician- patient relationship to improve treatment outcomes Facilitate patient groups including psychoeducational groups Are able to manage chronic illness and stress Effectively apply evidence-based brief psychotherapies Effectively apply evidence-based psychotherapies to the treatment of specific problems Teach mind–body techniques Understand that the medical provider may be more invested in the patient’s mental health treatment than the patient June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY 203 hierarchy within the medical setting that must be respected to honor the team approach to care. One respondent simply stated: ‘‘You are part of a team, but your work is not at the center [of patient care].’’ Another provider pointed out: ‘‘You are likely to feel one-down, and you should not take this personally, but see it in part as part of the culture of medicine.’’ Third, there is an expectation that necessary information will be readily shared among professionals. Each per- son’s job in patient care is dependent on information obtained by other members of the care team. One respondent explained: It is . . . normal for treatment in medical settings to be done in
- 47. teams . . . Information flows freely on the team because life and death matters are often involved. This may pose a problem for mental health professionals who have a more traditional view of how confidentiality should be dealt with. The mental health provider must think of him ⁄ herself as part of a treatment team; that communication within the team is as important as anything else the mental health provider may do, that his ⁄ her role may be consultative as often as it will be treatment oriented, that he ⁄ she may need to be flexible with regard to availability. Table 3 Skills for Collaborating with Medical Providers Relationship building Medical family therapists . . . Understand the importance of relationship building to effective collaboration Build relationships with medical providers and office staff Are available, accessible, and visible to healthcare providers and flexible in style of working Actively collaborate with health care providers as a member of the care team Place self in the traffic pattern without getting in the way Collaborative communication skills Medical family therapists . . . Work within multidisciplinary teams, keeping lines of
- 48. communication open to coordinate treatment Communicate with medical providers in an efficient and clear manner Fluently use appropriate medical terminology Talk about mental health problems in a way that is easily understood by health care providers and that is respectful of all perspectives Keep medical providers informed of progress and changes in care As invited, feel comfortable to provide feedback on the work of medical provider colleagues in the treatment of their patients Interpersonal expertise Medical family therapists . . . Understand that many medical providers become frustrated when dealing with chronic mental health problems Perceive medical provider distress and respond appropriately to alleviate the distress Monitor and appropriately respond to emotional reactivity in oneself and in medical providers Think relationally, not just in conceptualizing patients’ experiences, but also in conceptualizing the relationships among providers Assess one’s own participation in and contributions to the relationship with medical providers
- 49. Evaluate the effectiveness of the collaborative relationship among care team members and among treatment providers and patients 204 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012 Many respondents explained that they use their skills as a family therapist in their interac- tions in the multidisciplinary team in culturally sensitive ways. Similar to others, one respondent wrote that to be successful in the practice of MedFT ‘‘we need to use our therapeutic skills in order to join with this new system just like we would with a new family in therapy . . .’’ Another respondent emphasized: ‘‘MH providers need to JOIN, JOIN, JOIN with the culture and the providers.’’ Medical knowledge. Medical knowledge is the foundation of the language of medical set- tings. While mental health therapists do not need to be medical experts, it was consistently underscored that they need to have enough knowledge that they can have sufficient conversa- tional fluency to participate as team members in patient care. This includes knowing basic information about diseases, disease processes, course, and treatments, including pharmacologi- cal treatments. They should have a basic understanding of pharmakinetics and psychopharma- cology and know how and where to access medical and pharmacological information on an
- 50. on-going basis. They should be able to discuss the impact of commonly used medications on patient functioning and should recognize that medical providers may want to consult with them about pharmacological treatments. A few respondents indicated that it is important to know the ‘‘difference between primary and tertiary care and understand the domains of vari- ous specialties (e.g., neurology, endocrinology, oncology, obstetrics and gynecology, rheuma- tology).’’ Familiarity with most commonly used medical terms, abbreviations, and jargon in medical settings was also cited as important. One provider wrote: I don’t think the person has to be an expert or even very authoritative in all of these areas, especially in the beginning of the collaborative relationship. But an acknowledg- ment of their importance and a willingness to continue learning are crucial. Accommodating to the medical setting. Mental health therapists trained to work in tradi- tional mental health care settings need to accommodate their style of practice to fit the practice environment of the medical setting. One respondent wrote: ‘‘The medical system is bigger than us. MHP-s are the ones that need to do the cross-over learning and bridge the two cultures.’’ Several respondents were careful to point out that not all medical settings are alike, even though the culture of medicine is common to each. Medical settings differ according to spe- cialty, treatment emphasis, population served, and other factors.
- 51. The therapist’s ability to adapt their own way of working to match that of the setting is a key to success. Most respondents identified attributes that facilitate adaptability including ‘‘humility, patience, curiosity, non- judgmental attitude toward physician behavior, empathy, and willingness to take risks,’’ ‘‘lots of flexibility,’’ ‘‘self-motivation, persistence,’’ ‘‘openness,’’ and ‘‘a sense of humor.’’ These attri- butes allow therapists to adapt their approach and apply their expertise to the unique medical practice setting within which they are working. Mental health therapists cannot succeed if they treat it as a traditional mental health care practice setting, nor can they succeed if they attempt to practice traditional psychother- apy. Two representative examples from the data describe the types of accommodations that need to be made. First, the fast-paced nature of the practice of medicine places constraints on traditional mental health treatments. Respondents emphasized the importance of applying brief focused therapies that match the problem-focused, outcomes-oriented approach of med- icine. Second, the respondents pointed out the need to adapt the traditional role of the therapist as a treatment provider. A respondent explained that in these settings, therapists need to Be able to expand [their] sense of mental health treatment beyond the 50-minute ses- sion, for example, to see the opportunities such as being available for informal consul- tations, joining an MD in a medical visit with a challenging
- 52. patient, considering issues related to the general mental health of the staff and work relationships, attending to the relationship between the health care providers and patients, etc. Nurturing one’s professional identity. Mental health therapists working in medical settings can expect to experience a challenge to their professional identity, which could result in a redefini- June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY 205 tion of how they see themselves as professionals and in how they see themselves in relation to their peers who are not working in medical settings. One of the respondents related the following: One should expect a redefinition of one’s professional identity. When I started in this setting . . . I thought of myself as a family therapist. But over the years that has proven to be an inadequate designation. I see individuals as much as anything else. Often the main focus of the treatment I provide is to help the MD ⁄ patient relation- ship. I consult and educate as much as provide therapy. My most important interven- tions often have little to do with what goes on in the therapy hour (which is often not an hour!). I think that mental health professionals who want to work in collaborative settings must realize that the setting will shape them, and this
- 53. can be very exciting and enriching, but it can also be disorienting. Respondents explained they found it important to stay connected and involved with other mental health colleagues and with their professional organization. Another respondent cau- tioned: ‘‘Establish a support network with other mental health folks, either on site or in other settings. Share experiences. Consult regarding systems issues, and support each other. Take care of yourself. Have fun.’’ Staying connected to and grounded in the mental health discipline helped these respondents stay oriented and helped them preserve a coherent sense of professional identity. It also allowed them to test out their evolving ideas, to stay abreast of advances in men- tal health treatments, and to ensure that they were engaging in ethical mental health practice. Skills for Working With Patients All the competencies needed for traditional mental health care practice are needed for work in medical settings. Respondents explained that mental health therapists practicing MedFT need ‘‘sound therapy skills, including individual, couple, and family’’ and ‘‘excellent interview- ing skills.’’ But, working with patients in a medical setting also requires the use of unique skills in patient care. Conceptualizing patient problems. Participants uniformly identified the BPS model as the most useful conceptual model when providing direct patient care. They explained that those
- 54. practicing MedFT need to recognize that most patients get mental health treatment only after seeking help for medical conditions or relief from biological symptoms. Often the mental health problem is co-occurring with a biological health problem, and both must be considered in order for mental health treatment to be successful. The patient perspective, like that of the medical provider, is first biological and then (if at all) psychosocial. Knowing about the patient’s medical condition. Respondents acknowledged that patients expect mental health therapists working in medical settings to be part of the health care team. Therapists demonstrate that they are part of the team through their comfort with biomedical language and knowledge and curiosity about biomedical conditions. It is expected that they will use language that, while it may not be the same as that used by the medical provider, is at least consistent with that used by the medical provider. The therapist should be familiar with the patient’s medical condition and the diagnostic tests and treatments associated with that condi- tion. While they do not need to know everything about it, they should ‘‘know enough of the medical condition and treatments in order to explain it to patients.’’ What the therapist does not know, they should be willing to learn. One respondent wrote: I think that there is a difference between what information a mental health profes- sional should know and what they should be willing and able to learn. . . . So, in a sense, I believe that would serve the mental health professionals
- 55. (and the PCP [Primary Care Providers] and patient) the best to ‘‘know’’ how to access this information. Patient care. Respondents wrote that mental health therapists working in medical settings are expected to assess and diagnose patients using the approved nosology found in the current versions of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and Interna- tional Statistical Classification of Diseases and Related Health Problems (ICD). They are expected to know the evidence-based protocols and have competency in applying accepted 206 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012 treatments to specific mental health diagnoses. One respondent described this expectation in the following way: Medical providers are interested in problem-based knowledge. They are not interested in one’s conceptual framework, they are interested in what problems you can address. The biggest problem is depression. Other problems are anxiety, substance abuse, pain management, smoking cessation, weight loss, ADHD. I think that these problems pre- dominate because they are very challenging for MDs to treat. All these problems require an understanding of DSM IV categories. It is fine to treat these problems in a
- 56. family systems modality, but it is vital that the mental health professional feel comfort- able with traditional diagnostic categories. MDs expect mental health professionals to be able to assess, diagnose, treat, and make recommendations to the physician regard- ing how to manage these patients in office visits. They expect the kinds of things they would expect from any specialist. Mental health therapists can also expect that they will be asked to work with the most difficult patients. One respondent explained that therapists need to be prepared to work with ‘‘somatically-oriented, drug-seeking, dependent, hopelessly depressed, and chronically mentally ill patients.’’ These are patients who are often unwilling to accept that there are psychosocial problems co-occurring with (or in some cases, superseding) the biomedical ones. They should be able to creatively work with these and other patients who may not be interested in even acknowledging a mental health problem, let alone willing to accept a referral to a mental health therapist. It was common for respondents to explain that while this work with difficult patients is designed to improve patient functioning, that much of the mental health therapist’s work with these patients is to provide relief and support for the medical provider. One respondent explained: ‘‘You are a resource to clinicians for their own development of comfort with patients.’’
- 57. Skills for Collaborating With Medical Providers It is clear from the data that multidisciplinary collaboration is a hallmark and essential characteristic of MedFT. Collaboration is facilitated as mental health therapists (a) build rela- tionships with medical providers, (b) ensure frequent and accurate communication about patients, and (c) objectively attend to relationship processes. Building relationships with medical providers. Mental health therapists working in medical settings must recognize that the relationship among providers is the foundation for collabora- tive health care and that they must attend to these relationships if they are to be successful. One of the respondents wrote: ‘‘The most important key to success is the relationship between providers.’’ Another added that relationships among providers ‘‘are the basis for referral and collaboration.’’ Respondents emphasized that medical providers are problem- focused and action-oriented. Mental health therapists build relationships by being available to medical providers, by showing a willingness to accommodate to the pace of the work environment, and by actively participat- ing with medical providers in their patient care activities, such as rounds, care team meetings, and patient interviews. They should be flexible in their style of working (e.g., accepting inter- ruptions during treatment sessions, curbside consultations), and they should be able to place themselves in the traffic pattern without getting in the way.
- 58. Collaborative communication. Frequency, length, and content of communication character- ize collaborative relationships in medical settings. Respondents indicated that medical providers expect regular communication about patients and treatment progress and that this communica- tion should be of sufficient frequency that medical providers can feel they are included in the treatment, that they have not lost their patient. ‘‘Once the collaborative medical professional refers a patient he or she will also want to be updated regularly and be included as part of the treatment process.’’ This level of communication respects the hierarchy within the medical setting and acknowledges that the medical provider is ‘‘in charge’’ of patient care. June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY 207 Because the use of language in medical settings is instrumental and action-oriented, the mental health therapist should match this communication style. Messages should be efficient and clear. One respondent explained that ‘‘most collaboration occurs through interactions that last <5 min. These are the bumps in the hall.’’ Because of this, being ‘‘accessible’’ and ‘‘visible’’ were repeatedly mentioned as essential to effective communication and collaboration. Several respondents stressed that medical providers expect to hear ‘‘what works and what one can do rather than what one thinks.’’ The caution to
- 59. traditionally trained mental health therapists is to limit theoretical explanations and to stick to what is directly relevant to the care plan. One respondent counseled: ‘‘Don’t bore people with details that don’t impact patient management.’’ Similar advice was given by another who wrote: ‘‘Be able to be concise and jar- gon free about what you believe is going on in a case.’’ Another wrote: ‘‘willingness to talk the medical language as much as possible and minimize psychobabble.’’ Another respondent even went as far as to caution well-intentioned therapists to be careful not to ‘‘proselytize’’ or become too ‘‘psychosocially fixated.’’ Yet another wrote that a successful mental health thera- pist is ‘‘one who does not feel he ⁄ she needs to preach systems to those who work in the setting; very off- putting.’’ Communicating in this way requires mental health therapists to be ‘‘comfort[able] with their own skills [without a] continuous need to prove oneself [and an] ability to function without a lot of . . . validation.’’ As participants in the communication dynamic within a medical setting, thera- pists are confident, assertive, patient, flexible, and accommodating. The respondents explained that this stance leads medical providers to ‘‘confidently value the role you play.’’ Be relationship experts. It is clear from the data that one of the roles played by mental health therapists, as relationship experts, is to attend to the relationships among providers and between providers and patients, and to intervene in a way that improves collaboration and
- 60. health outcomes. Respondents explained that medical providers expect the mental health therapist to objec- tively observe these relationships and to intervene appropriately. DISCUSSION This study results in a greater understanding of the practice of MedFT, and the unique skills needed to engage in this practice. It is clear from the data that the practice of MedFT is different from traditional mental health care practice. There appear to be two primary differ- ences. First, in addition to requiring competency in the practice of psychotherapy, MedFT requires additional competencies unique to working within the culture of medicine. Second, some competencies, while perhaps not unique to MedFT, are noteworthy because they are uniquely prominent in the practice of MedFT. So, for example, while all MFTs should have competency in multidisciplinary collaboration, it is uniquely prominent in the practice of Med- FT where therapists must negotiate daily professional relationships in a multidisciplinary envi- ronment that is inherently hierarchical. These two types of unique competencies are most likely an outgrowth of the application of the BPS model that requires therapists to consider multiple systems of functioning simulta- neously. In the practice of MedFT, the curative work of the therapist includes both interactions with the patient and family as well as interactions with medical
- 61. providers and others involved in the patient’s care. A true acknowledgment of the biological system begs multidisciplinary col- laboration just as a true acknowledgment of the social system begs family involvement in treat- ment. Consequently, the application of the BPS model expands the practice and the treatment to include interactions with other systems and people. This requires competencies in addition to those expected of skilled marriage and family therapists. Multidisciplinary collaboration appears to be a hallmark of MedFT. The modern medical system is inherently collaborative, while the modern mental health care system is not. Medical systems generally adopt a leadership model of collaboration that has a clear hierarchy with physicians, and in some cases, mid-level medical providers in the leadership role. It is clear from the data obtained from those experienced in the practice of MedFT that if MFTs are to succeed in a medical system, they must understand and respect the leadership model of 208 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012 collaboration. They may need to change their way of practicing to accommodate to the system rather than try to change the system to fit their way of doing things. This may even include the way that psychotherapy is practiced. Participants frequently extolled the importance of flexibil- ity in practice, curiosity about new ways of doing things, and
- 62. willingness to learn. The results of this study are the next step in articulating the competencies mental health therapists need to have to practice what has come to be known as MedFT. It would be a mis- take to assume that the set of competencies generated through this study is exhaustive. Perhaps if we would have returned to the participants to request additional competencies, others would have emerged. We know through the literature that other skills have been identified that were not mentioned in the data that we obtained. For example, some authors have expanded the BPS model to include the spiritual dimensions of patient functioning (e.g., Prest & Robinson, 2006), yet none of our participants acknowledged the spiritual dimension nor skills specific to working within this dimension. Also, while participants indicated that it was important to be curious about nontraditional approaches to care, only one participant made even passing refer- ence to mind–body techniques. Yet, the literature suggests that these techniques are particularly efficacious (Astin, Shapiro, Eisenberg, & Forys, 2003) and within the scope of practice of mar- riage and family therapists (McCollum & Gehart, 2010). We are aware of some therapists working in medical settings who regularly teach mind–body techniques to their patients and to medical students (Saunders et al., 2007). Other skills not mentioned include the importance of knowing how patients move through the medical system and being able to intervene on the patient’s behalf, skills specifically related to making referrals so that the biological dimensions
- 63. of mental health problems are addressed, and understanding how payment and billing occur within the medical setting in which one is working (Patterson et al., 2002). Emphasized in our data was the importance of cultural competence in relation to the culture of the medical system. Given that this was such a prominent theme, we found it curious that we were not able to find references to the importance of demonstrating competency with the culture of the patient’s system. Similarly, while participants were careful to identify the importance of recognizing and negotiating power imbalances in the medical setting, they did not identify the importance of being sensitive to how these same power dynamics impact patients and families and the role of the therapist in helping them navigate these power imbalances. That these two seemingly important skills were not mentioned may be a function of how the questions were worded; we specifically asked for unique knowledge and skills to the practice of MedFT. It may be that participants see these competencies as important to the practice of marriage and family therapy and psychotherapy in general and not unique to the practice of MedFT. It is possible that had we asked specifically about these, and other techniques gleaned from the literature and experience, that we would have been able to develop a more comprehensive list. But, then we might have sacrificed coming to understand those competencies that are spe- cifically unique to the practice of MedFT. Additional research is needed to further refine and
- 64. expand this list of skills. Specifically, it is possible that the application of a Delphi methodology (Stone Fish & Busby, 1996) could be helpful in clarifying those skills that are particularly important to the practice of MedFT. This method has been used successfully by others to develop lists of skills, most notably the list that has become the AAMFT core competencies (Nelson et al., 2007). Implications for Training and Practice Identifying competencies is a first step toward developing learning and assessment activities that will expedite student learning (Maki, 2004). A logical next step is to develop learning and assessment activities, similar to what has been carried out with regard to the AAMFT core competencies (Hodgson, Lamson, & Feldhousen, 2007; Miller, Linville, Todahl, & Metcalfe, 2009; Openshaw et al., 2006; Perosa & Perosa, 2010). The results of this research will facilitate the development of these learning and assessment activities. Developing these activities in light of learning outcomes will lead to training that is more focused and efficient and that will better prepare students for the realities of collaborative care practice. The results will also help experi- enced therapists interested in expanding or changing their practice to include work in medical settings and medical, mental health collaborations. These therapists can use this research to June 2012 JOURNAL OF MARITAL AND FAMILY THERAPY 209
- 65. understand the skills unique to the practice of MedFT. Attending to these unique skills will help them appropriately incorporate these skills into their practice, thereby increasing the likeli- hood that the transition in their practice will be successful. Those already working in medical settings will find that these results provide them with literature that will help to document and articulate the competencies needed for MedFT. This may be particularly important in attempt- ing to described MedFT to those who may not be familiar with it. It may also help by provid- ing a useful organization of these skills and practices unique to MedFT. These and other implications are important to the advancement of the practice of MedFT. REFERENCES Astin, J. A., Shapiro, S. L., Eisenberg, D. M., & Forys, K. L. (2003). Mind-body medicine: State of the science, implications for practice. The Journal of the American Board of Family Practice, 16, 131–147. Bloch, D. A., & Doherty, W. J. (2001). The continuing evolution of the Collaborative Family Healthcare Associ- ation. Families, Systems, and Health, 19, 1–3. Blount, A. (Eds.) (1998). Integrated primary care: The future of medical and mental health collaboration. New York: Norton.
- 66. Cambell, T. L. (1996). Clinical trials of collaborative healthcare. Families, Systems, and Health, 14, 137–144. Campbell, T. L., & Patterson, J. M. (1995). The effectiveness of family interventions in the treatment of physical illness. Journal of Marital and Family Therapy, 21, 545–584. Crane, D. R., & Christenson, J. D. (2008). The medical offset effect: Patterns in outpatient services reduction for high utilizers of health care. Contemporary Family Therapy, 30, 127–138. Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196, 129–136. Hodgson, J. L., Lamson, A. L., & Feldhousen, E. B. (2007). Use of simulated clients in marriage and family therapy education. Journal of Marital and Family Therapy, 33, 35–50. Law, D. D., Crane, D. R., & Berge, J. (2003). The influence of marital and family therapy on high utilizers of health care. Journal of Marital and Family Therapy, 29(3), 353– 363. Maki, P. L. (2004). Assessing for learning: Building a sustainable commitment across the institution. Sterling, VA: Stylus. McCollum, E. E., & Gehart, D. R. (2010). Using mindfulness
- 67. meditation to teach beginning therapists therapeu- tic presence: A qualitative study. Journal of Marital and Family Therapy, 36, 347–360. McDaniel, S., Hepworth, J., & Doherty, W. (1992). Medical family therapy: A biopsychosocial approach to fami- lies with health problems. New York: Basic Books. Miles, M. B., & Huberman, A. M. (1994). Qualitative data analysis (2nd ed.). Thousand Oaks, CA: Sage. Miller, J. K., Linville, D., Todahl, J., & Metcalfe, J. (2009). Using mock trials to teach students forensic core competencies in marriage and family therapy. Journal of Marital and Family Therapy, 35, 456–465. Miller, J. K., Todahl, J. L., & Platt, J. J. (2010). The core competencies movement in marriage and family ther- apy: Key considerations from other disciplines. Journal of Marital and Family Therapy, 36, 59–70. Nelson, T. S., Chenail, R. J., Alexander, J. F., Crane, D. R., Johnson, S. M., & Schwallie, L. (2007). The devel- opment of core competencies for the practice of marriage and family therapy. Journal of Marital and Family Therapy, 33, 417–438. Openshaw, D. K., Miller, J. K., Todahl, J. L., Linville, D., Platt, J. J., & Coyle, S. (2006, October). The AAMFT
- 68. core competencies: Conceptualization and application. Paper presented at the 2006 Annual Conference of the American Association for Marriage and Family Therapy, Austin, TX. Patterson, J., Peek, C. J., Heinrich, R. L., Bischoff, R. J., & Scherger, J. (2002). Mental health professionals in medical settings: A primer. New York: Norton. Patton, M. Q. (2002). Qualitative research and evaluation methods (3rd ed.). Thousand Oaks, CA: Sage. Perosa, L. M., & Perosa, S. L. (2010). Assessing competencies in couples and family therapy ⁄ counseling: A call to the profession. Journal of Marital and Family Therapy, 36, 126–143. Prest, L. A., & Robinson, W. D. (2006). Systemic assessment and treatment of depression and anxiety in families: The BPSS model in practice. Journal of Systemic Therapies, 25(3), 4–23. Prouty-Lyness, A. M. (2003). Feminist perspectives in medical family therapy. New York: Haworth. Saunders, P. A., Tractenberg, R. E., Chaterji, R., Amri, H., Harazduk, N., Gordon, J. S., et al. (2007). Promot- ing self-awareness and reflection through an experiential mind- body skills course for first year medical stu- dents. Medical Teacher, 29, 778–784.
- 69. Seaburn, D. B., Lorenz, A. D., Gunn, W. B., Gawinski, B. A., & Mauksch, L. B. (1996). Models of collaboration: A guide for MHP-s working with health care practitioners. New York: Basic Books. Stone Fish, L., & Busby, D. M. (1996). The Delphi method. In D. H. Sprenkle & S. M. Moon (Eds.), Research methods in family therapy (pp. 469–484). New York: Guilford. 210 JOURNAL OF MARITAL AND FAMILY THERAPY June 2012 Copyright of Journal of Marital & Family Therapy is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. O R I G I N A L P A P E R ‘‘Is Our Daughter Crazy or Bad?’’: A Case Study of Therapeutic Assessment with Children Francesca Fantini • Filippo Aschieri • Paolo Bertrando Published online: 28 March 2013
- 70. � Springer Science+Business Media New York 2013 Abstract In this paper we present a new model of intervention with documented efficacy that combines psychological tests and assessment methods with therapeutic techniques to promote change in clients. We will discuss Therapeutic Assessment of Children and their families (TA-C) through the case of a 4-year-old girl, Clara, and her family. Clara’s parents were distressed by her uncontrollable rage outbursts and feared she might be ‘‘crazy’’. The treatment helped to shift the narrative the parents had about Clara and give new meanings to her behaviors. We describe in detail the steps of the assessment and provide a theoretical discussion of the therapeutic processes involved. Keywords Assessment � Family � Children � Therapy Within systemic therapy, skepticism about the tools and methods typical of psychological assessment has been fostered both by the social constructionist stance that prevailed within the field in recent year, and by prejudices about the very nature of testing, i.e., the idea that psychological tests pertain to the domain of naı̈ ve realism and
- 71. tend to give an account of clients’ problems framed in a positivistic view. In such a context, psychological assessment is viewed as an effort to measure the ‘‘true reality’’ of clients’ problems, thereby mini- mizing their own experiences, views, and hypotheses (Brown 1972). While this underlying philosophy may characterize the traditional approach to psychological assessment, in recent years new ways have been developed of integrating the tools and methods of the assessment practice in a therapeutic and post-modern framework. This is the case of Therapeutic Assessment (TA), a semi-structured form of brief integrative intervention (Kaslow 2000) developed by Finn and his colleagues (Finn and Tonsager 1992, 1997; Finn 2007) over the last 20 years. TA combines psychological assessment with techniques and F. Fantini � F. Aschieri (&) European Center for Therapeutic Assessment, Università Cattolica del Sacro Cuore, Via Nirone 15, 20123 Milan, Italy e-mail: [email protected] P. Bertrando Private practice, Milan, Italy
- 72. 123 Contemp Fam Ther (2013) 35:731–744 DOI 10.1007/s10591-013-9265-3 principles of interpersonal and systemic psychotherapy. TA has proved to be effective with different types of clients such as adult outpatients (Finn and Tonsager 1992; Newman and Greenway 1997), couples (Durham-Fowler 2010), families with children (Tharinger et al. 2009; Smith et al. 2010), and adolescents (Ougrin et al. 2008). Research has focused on the effectiveness of TA with different types of problems, i.e., self- harm (Ougrin et al. 2008); internalizing symptoms, (Aschieri and Smith 2012); externalizing symptoms (Smith et al. 2010); disorganized attachment (Smith and George 2012); and developmental trauma (Tarocchi et al. in press). Therapeutic Assessment with Children and Their Families TA with children and their families (TA-C) involves a suggested series of steps described
- 73. in various publications (Aschieri et al. 2013; Smith et al. 2009; Tharinger et al. 2008a; Finn 2007). In summary, after the initial phone contacts, the assessor meets the parents to co- construct assessment questions that capture their main puzzles and worries about their child or their relationship with their child (Step 1). By focusing on the parents’ questions, the assessor aims to involve parents as active participants from the beginning of the process. Assessment questions are used to build an alliance around parents’ motivations and goals, and to foster their curiosity about their child. Also, the clear formulation of the assessment goals as focused on their puzzles and worries has the effect to lower the parents’ anxiety about the assessment. The assessor also works to gather background information about the family and uses assessment questions as guides to chose which themes the parents are open to discuss and don’t find threatening. In fact, besides the explicit goal of collecting parents’ questions, the assessor also works to build a secure
- 74. relationship with them, based on experiences of emotional attunement, collaborative communication and the repair of possible disruptions (Finn 2012). The creation of a such a relationship is considered essential for a therapeutic change to occur. The child being assessed may have his/her own questions too, and these are collected in the second session, usually scheduled with the whole family. Afterwards, the assessor begins the testing phase with the child to collect useful information relevant to the assessment questions. The parents are usually asked to observe test administration or the unstructured activities (i.e. drawings) that are part of this phase from behind a one-way mirror, over a video link, or from the corner of the testing room (Step 2). Later, the assessor and parents discuss their observations and their relevance to the parents’ assessment questions (Tharinger et al. 2008b). Different from other systemic collaborative interventions (see, for example, Teixeira et al. 2011), in TA-C the parents are involved directly as co-assessors, observing
- 75. and interpreting their children’s behaviors during the testing. Next the assessor schedules one or more family sessions, the so called intervention sessions; these represent occasions to work even more on the systemic aspects of the child’s problem and to work with the family members on possible new ways of interacting (Tharinger et al. 2008a) (Step 3). Finally, the assessor meets the parents for a summary/discussion (i.e., feedback) session, where the main results of the assessment are summarized and discussed (Finn 2007; Tharinger et al. 2008b) (Step 4). The assessor also gives feedback to the child about the assessment results in the form of an individualized fable (Tharinger et al. 2008c) (Step 5). TA-C can be done by one clinician or by two, depending on the presence of a colleague trained in the approach and on the financial aspects of the assessment. Clearly, one of the main advantages of working with a co-therapist is that during the testing phase, while one clinician works with the child, the other can stay behind the one-way mirror with the
- 76. 732 Contemp Fam Ther (2013) 35:731–744 123 parents. There, the second clinician can support the parents emotionally and begin com- menting with them on what is happening in the assessment room with the child. A recent review of the research on TA by Finn et al. (2012) revealed fewer empirical studies supporting TA-C than TA with adult clients. However, the results available so far are promising. An aggregate group study by Tharinger et al. (2009) assessed the overall effectiveness of the TA-C model with 14 families with preadolescent children referred for emotional and behavioral problems. The study showed that TA- C reduced symptoms in both parents and children, increased communication and positive emotions, and decreased negative emotions and conflicts within the family. Also, participants reported high engagement in the assessment and satisfaction with the services. Tharinger and Pilgrim