Downloaded 15 times

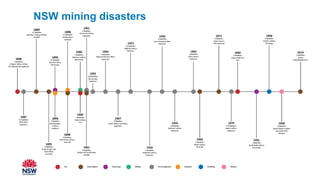
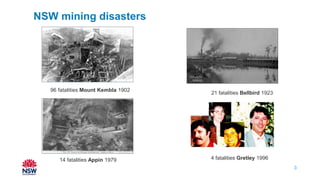
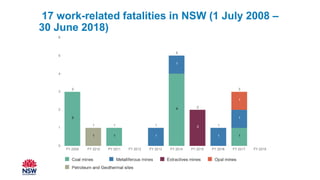
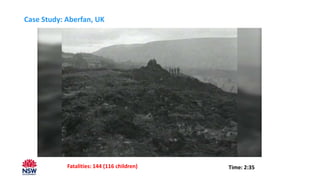
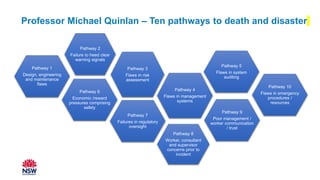
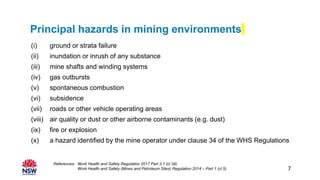
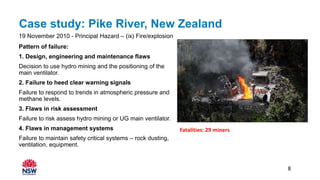
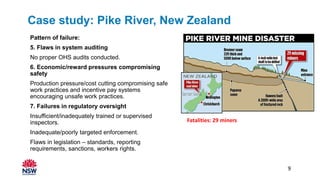
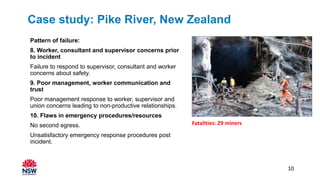
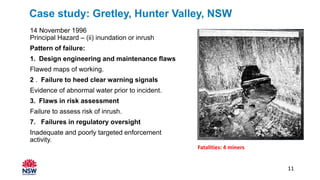
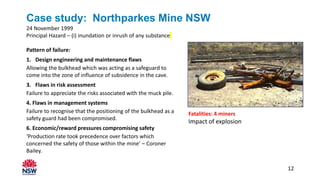


The document discusses various mining disasters in New South Wales, highlighting fatalities and case studies that identify patterns of failure leading to these incidents. Key factors include design and maintenance flaws, poor risk assessment, and deficiencies in management systems and regulatory oversight. Recommendations for better safety include an effective regulatory framework, strong leadership, and proactive risk management practices.