
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Acute Disseminated Encephalomyelitis
Similar to Acute Disseminated Encephalomyelitis (20)
Recently uploaded
Recently uploaded (20)
Acute Disseminated Encephalomyelitis
- 2. Acute disseminated encephalomyelitis (ADEM), is also known as postinfectious encephalomyelitis sometimes. It is a demyelinating disease of the central nervous system that typically presents as a monophasic disorder associated with multifocal neurologic symptoms and disability. A mean age of between 5-8 years.
- 3. Acute disseminated encephalomyelitis (ADEM) is a neurological, immune-mediated disorder in which widespread inflammation of the brain and spinal cord damages tissue known as white matter. White matter is tissue composed of nerve fibres, many of which are covered by a collection of fats and proteins known as myelin. Myelin, which collectively may be referred to as the myelin sheath, protects the nerve fibres, acts as an insulator and increases the speed of transmission of nerve signals. Damage to the myelin sheath affects the nerve’s ability to transmit information and potentially can cause a wide range of neurological symptoms. INTRODUCTI ON
- 4. The exact cause of ADEM is not known. Many researchers suggest that ADEM may represent an abnormal immune reaction directed against the body’s own tissues (autoimmune disorder). In autoimmune disorders, the body’s natural defences (e.g., antibodies, lymphocytes) against substances that are perceived as foreign (antigens) inappropriately begin to attack healthy tissues, for unknown reasons.
- 5. In approximately 50-75 percent of ADEM cases, the inflammatory attack is preceded by a viral or bacterial infection. The inflammatory attack and neurological symptoms often begin within a couple of weeks after the viral or bacterial illness. Large number of viruses associated with these infections, including : • Measles , Mumps, Rubella • Varicella zoster, Epstein-Barr, Cytomegalovirus • Herpes simplex, Hepatitis A, Influenza • Enterovirus infections.
- 6. *Less than 5 percent of ADEM cases follow immunization. Currently the measles, mumps and rubella vaccinations are the most commonly associated vaccinations with post- vaccineADEM. Neurological symptoms typically appear 4 to 14 days after the immunization has been done.
- 7. Categories ofADEM 1.MonophasicADEM *Any new or changing symptoms within this three month period is considered as one event. * Is a one-time episode that can develop over a period for as long as three months. * Symptoms that might occur during an oral steroid taper or within one month of the completion of the taper are also classified as one single episode.
- 8. *Is defined as a subsequent attack that involves the same symptoms that occurred during the initial attack. *The MRI findings tend to be similar to the initial attack, and there are no lesions, but there could be an enlargement of the lesions from the original episode
- 9. 3. MultiphasicADEM *There must be signs of encephalopathy, but symptoms and neuroimaging findings are in different areas from the initial attack. *There might be new lesions evident on MRI and there might also be evidence of partial or complete resolution of the lesions associated with the first episode
- 10. Fever, Headache, and Vomiting Encephalopathy is a characteristic feature of ADEM and usually develops rapidly. Signs and Symptoms
- 11. Encephalopathy results in symptoms, such as: * Altered level of consciousness (lethargy →coma) * Acute cognitive dysfunction * Behavioral changes * Seizures In about ⅓ of those diagnosed. Other common neurologic signs of ADEM include: * Long tract pyramidal signs *Acute hemiparesis *Cerebellar ataxia *Cranial neuropathies
- 13. A diagnosis is made based upon identification of characteristic symptoms, a detailed patient history, a thorough clinical evaluation and a variety of specialized tests including imaging techniques such as magnetic resonance imaging (MRI). An MRI can demonstrate characteristic brain lesions in individuals with ADEM. Additional tests to exclude other conditions may also be performed. Such tests may include infectious, immunologic, and metabolic tests.
- 14. * An ADEM diagnosis is considered when individuals develop multifocal neurologic abnormalities with: o Excessive irritability o Confusion o Altered level of consciousness (encephalopathy) Especially if the onset of symptoms occurs within 1 to 2 weeks after a viral/bacterial infection or a vaccination
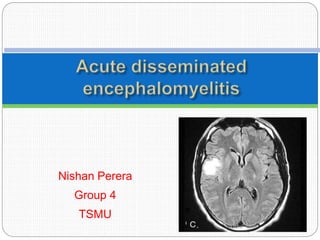
- 15. Axial T2-weighted FLAIR MRI of the brain in a child with acute disseminated encephalomyelitis (ADEM).
- 17. Children with ADEM typically present with fever, meningeal signs, acute encephalopathy, and evidence of inflammation in blood and cerebrospinal fluid. Thus, consideration should be given to treatment with broad-spectrum antibiotics and acyclovir until an infectious etiology is excluded.
- 18. 1. high-dose intravenous glucocorticoids. 2. intravenous immunoglobulin. 3. plasma exchange. However, the effectiveness of these treatments forADEM has not been definitively confirmed, as there are no prospective clinical trial data to determine optimal treatment, including dose or duration.
- 19. In the only study that compared these two treatments for ADEM intravenous methylprednisolone (n=21) was associated with a modestly better outcome, as measured by the median Expanded Disability Status Scale, than intravenous dexamethasone (n=25), and the difference was statistically significant . The strength of this result is limited by small patient numbers, lack of randomization, and lack of blinded treatment or assessment.
- 20. Data from small case series and case reports suggest that intravenous immune globulin (IVIG) is beneficial as rescue therapy in patients with ADEM who fail to respond to methylprednisolone or as initial therapy . Dosing of IVIG in these studies ranged from 1- 2 g/kg given either as a single dose or divided over 3 – 5 days .
- 21. Limited data suggest that plasma exchange is beneficial in children with ADEM who fail treatment with IVIG and/or methylprednisolone . The largest series was retrospective and reported improvement following plasma exchange in six children with ADEM who did not respond to initial treatment with glucocorticoids followed by IVIG . In another retrospective study, plasma exchange demonstrated some benefit for patients with idiopathic transverse myelitis when used in combination with iv glucocorticoids. Therefore, it may be of particular benefit for patients withADEM associated with myelopathy .
- 22. Although no consensus exists, some experts suggest obtaining at least two additional MRIs after the 1st normal MRI, over a period of at least 5 years from the initial episode ofADEM to confirm the absence of new inflammatory demyelinating lesions .
- 23. Most children with ADEM make a full recovery, usually slowly over 4 – 6 weeks. At follow-up, approximately 60 - 90 % have minimal or no neurologic deficits . Although modern studies of ADEM in children report little or no mortality, earlier studies suggested that the mortality of postinfectious ADEM was as high as 5 %. The extent and site of lesions on the initial MRI do not predict
- 24. the following case series illustrate the range of outcomes for children withADEM: The largest study included 84 children from Argentina withADEM. At a mean follow-up of 6.6 years, the neurologic examination was either normal or detected minor abnormalities but no associated disability in 75 children (89 %). Residual deficits in the remaining children included : mild to severe hemiparesis, mild paraparesis, partial epilepsy, reduced visual acuity, and mental handicap.
- 25. In a report from Australia, 31 children withADEM were followed for an average of 18 months . Complete recovery occurred in 25 (81 %). Mild abnormalities were detected in the remaining 6 patients; these included recurrent headaches, behavioral problems, esotropia, subtle hemiparesis, and minor gross motor abnormalities.
- 26. DONE BY NISHAN PERERA TSMU GROUP 4