Fluids 101 Fluidsbring nutrition and oxygen into the cells and remove wastes Fluid is divided into two compartments: intracellular and extracellular Extracellular is divided into interstitial and intravascular
3.
Fluids 101 Thebody’s fluid should be in balance; volume entering the body = volume leaving the body Fluid loss occurs via urine, sweat, stool, and incidental losses from respiratory effort
4.
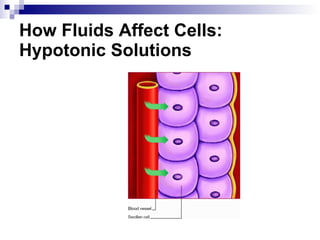
On the MoveDiffusion: Passive movement of fluid from an area of higher concentration to an area of lower concentration Osmosis: Water movement through a selectively permeable membrane from an area of lower concentration to an area of higher concentration
5.
On the MoveActive transport: Movement of molecules against a concentration as they move from an area of lower concentration to an area of higher concentration; this movement requires energy Third spacing occurs when the fluid is “trapped” in the interstitial spaces
Decreased Oncotic PressureLoss of albumin or protein leads to decreased oncotic pressure, causing fluid to “leak” from the intravascular space to the interstitial space Due to the loss in circulating fluid volume, cardiac output decreases
10.
Causes of FluidShifts Albumin losses can occur in liver failure, liver dysfunction, and malnutrition Albumin losses can lead to fluid shifting into the peritoneum, causing ascites Destruction of endothelial cells, such as in bowel surgery, can cause fluid to move and be trapped in the interstitial spaces Fluid trapped in the lungs can lead to pulmonary edema
11.
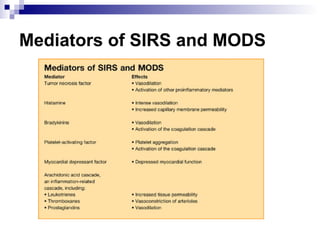
Inside the CellsInterstitial fluid trapping can cause compression of the microvasculature, resulting in hypoperfusion and ischemia Inflammatory “mediators” are released into the bloodstream, which can lead to systemic inflammatory response syndrome (SIRS) Multiple organ dysfunction syndrome (MODS) occurs, leading to organ failure and death
What Happens WhenFluids Shift? With decreased circulating volume, baroreceptors in the aorta are activated Sympathetic nervous system releases epinephrine and norepinephrine, causing vasoconstriction and an increased heart rate Kidneys launch the renin-angiotensin-aldosterone system in response to a lower glomerular filtration rate All this happens with the goal of increasing circulating volume, blood pressure, and cardiac output
14.
Fluid Shift inthe Bowel Causes abdominal distention Measure bladder pressure and abdominal girth at least every 4 to 8 hours while signs are abnormal
15.
Making the GradeA patient’s intra-abdominal pressure (IAP) determines if he has intra-abdominal hypertension. According to the World Society of Abdominal Compartment Syndrome, there are four grades of intra-abdominal hypertension: Grade I: IAP of 12 to 15 mm Hg Grade II: IAP of 16 to 20 mm Hg Grade III: IAP of 21 to 25 mm Hg Grade IV: IAP of > 25 mm Hg
16.
Complications of AbdominalSwelling Decreased cardiac output leads to decreased blood pressure, which causes: increased pressure on the aorta and the iliac and femoral arteries, leading to decreased cardiac output and decreased blood pressure impaired kidney function impaired blood flow to the bowel, liver, and spleen
17.
Monitoring the PatientFluid shift will either resolve over the next several hours (up to 48 hours) or the patient will continue to develop bowel edema and, eventually, ischemia Closely monitor vital signs, urine output, peripheral perfusion, mental status, ventilation/perfusion status, hematocrit/hemoglobin, serum electrolytes (elevated lactate may indicate bowel ischemia)
18.
Fluid Resuscitation Administermaintenance I.V. isotonic fluid plus intermittent colloids (i.e., albumin); pulls fluid from the interstitial spaces into the intravascular space Small dose of a loop diuretic, such as furosemide (Lasix) may be ordered if kidneys can’t get rid of the excess fluid If hemoglobin is low, infuse blood products, such as packed red blood cells, as ordered to help increase oxygen and pull fluid from the interstitial space
19.
If Bowel IschemiaOccurs A kidney-ureter-bladder X-ray (KUB) may be done; it will show bowel edema and any “free air,” which may indicate bowel perforation A CT scan can detect worsening bowel edema, inadequate perfusion, and hematomas Patient may need further surgery to repair a perforated bowel or to decrease edema