Disc prolaps and rehabilitation
•Download as PPTX, PDF•
6 likes•1,456 views

Any buldge around disc causing compression of nerve root. Herniation of disc is of 4 types:- Contact:- No rupture in outer layer of NP within their limit, discogenic pain & deep dull pain. Complete rupture /protruded disc :- Outer most layer is intact & inner layer of AF is ruptured. Herniated Sequestered disc:- Outer most layer is also ruptured & nerve root compression (NRC) is there. 4 No buldge:- Nuclear Matrix comes out but no rupture of AF, No NRC but sequestration NRC is there.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Disc prolaps and rehabilitation
Similar to Disc prolaps and rehabilitation (20)
More from Shri Guru Ram Rai Institute of Medical Science
More from Shri Guru Ram Rai Institute of Medical Science (20)
Recently uploaded
Recently uploaded (20)
Disc prolaps and rehabilitation
- 1. DISC HERNIATION Dr. Niraj Kumar , Pt BPT, MPT MHA & Ph.D Physiotherapy (Orthopaeducs) Associate Professor Physiotherapy Dept. Shri Guru Rai Institute Of Paramedical Sciences , Dehradun
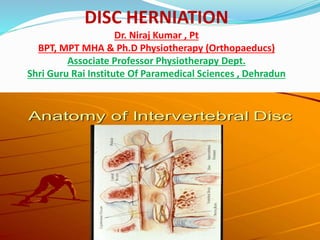
- 2. IVD consist of AF,NP & CEP. The central core of the IVD is composed of the NP. The AF surrounds the NP, occupying the majority of the disc space. On the superior and inferior surfaces of the IVD lies the cartilage end plates. The spinal column has 23 IVDs, starting from the C2-3 interspace to the L5-S1 interspace. C= 6, T= 12 & L=5. The IVD is generally considered to be an avascular tissue structure. The IVD receives innervations primarily from two sources: the sinuvertebral nerve and the sympathetic trunk via the multiple gray rami. The Biochemical Composition • Water : 65 ~ 90% wet wt. • Collagen : 15 ~ 65% dry wt. • Proteoglycan : 10 ~ 60% dry wt. • Other matrix protein : 15 ~ 45% dry wt.
- 4. Function:- 1. Separate the vertebrae from each other. 2. provides the surface for the shock-absorbing gel of the nucleus pulposus. 3. The NP distribute hydraulic pressure in all directions within each IVD under compressive loads. 4. Restricted intervertebral joint motion • 5. Contribution to stability • 6. Resistance to axial, rotational, and bending load
- 5. DEFINATION:- Any buldge around disc causing compression of nerve root. Herniation of disc is of 4 types:- 1. Contact:- No rupture in outer layer of NP within their limit, discogenic pain & deep dull pain. 2. Complete rupture /protruded disc :- Outer most layer is intact & inner layer of AF is ruptured. 3. Herniated Sequestered disc:- Outer most layer is also ruptured & nerve root compression (NRC) is there. 4 No buldge:- Nuclear Matrix comes out but no rupture of AF, No NRC but sequestration NRC is there.
- 6. Resinick & Niwayma etal classified into following type:- 1) Annular buldge:- Weakened portion of AF is buldge out, pain with or without radiation. 2) Protrusion:- Nuclear matrix protrudes periphery but outer layer of periphery intact but inner layer of periphery rupture. 3) Extrusion:- Outer layer also damages & nuclear matrix comes out, NRC is there. 4) Sequestration:- Extruded material will give another buldge. And +ve NRC.
- 7. 1) Repetitive mechanical activities – Frequent bending, twisting, lifting, pushing , pulling and other similar activities causes discs damaged. 2) Living a sedentary lifestyle – Individuals who rarely if ever engage in physical activity are more prone to herniated discs because the muscles that support the back and neck weaken, which increases strain on the spine. 3) Degenerative changes:- Degeneration is the major cause of spinal disc herniation mostly seen in old age pts. that weakened the disc causes herniation. 4) Traumatic injury to lumbar discs commonly occurs when lifting while bent at the waist, rather than lifting with the legs while the back is straight. 4) Obesity – Spinal degeneration can be occurred dueto excess body fat. 5) Poor posture – Improper spinal alignment while sitting, standing, or lying down strains the back and neck. 6) Tobacco abuse – The chemicals commonly found in cigarettes can interfere with the disc’s ability to absorb nutrients, which results in the weakening of the disc. 7) Mutation- in genes coding for proteins involved in the regulation of the extracellular matrix, such as MMP2 and THBS2, has been demonstrate 8) Poor and inadequate strength of the trunk 9) Sitting for long hours.
- 8. INTRA-DISCAL PRESSURE In supine/prone lying----25kg discal pressure. Side lying—75kg, Standing---100kg Sitting without support-----140kg Sitting forward---185kg Sitting forward without lifting weight on hand-----275kg Standing lifting weight, hip bending---340kg On coughing, laughing---120kg
- 9. Neck /Cervical region *Severe Pain in back of neck & Arm muscle weakness *Deep ach pain near or over the shoulder blades on the affected side *Increased pain when bending the neck or turning head to the side *Pain made worse with coughing, straining or laughing *Neck pain, especially in the back and sides along with spasm *Burning pain radiating to the shoulder, upper arm, forearm, and rarely the hand, fingers or chest *Tingling or numbness in one arm
- 10. Lower Back /Lumbar area *Severe low-back pain *Pain radiating to the buttocks, legs, and feet. *Pain worse with coughing, straining or laughing & during spinal flexion. *Muscle spasm *Tingling or numbness in legs or feet* *Muscle weakness or atrophy in later stages *Loss of bladder or bowel control & numbness in the genital area in case of cauda -equina syndrome
- 11. 1. First no complain of radiation, when radiation occurs then actually the disc is occurs i.e true herniation. 2. Neurogenic Pain in Cx & Lx area. 3. Paresthesia about 75% of pts. 4. Numbness, loss of sensation at dermatome level. 5. Tenderness over particular herniated discal level. 6. Spinal mobility- Pain aggravates on forwards bending of Cx & Lx . Sometime lateral bending is also painful. 7. L5 nerve root compression causes difficulties of great toes extension. 8. Inability to walk
- 14. Differential diagnosis 1.Mechanical pain 2.Discogenic pain 3. Osteoporosis 4. Osteomyelitis 5. Spondylosis 6. Spinal stenosis 7. Spondylolysthesis – Step Deformity at particular level. 8.Neurofibroma- Nerve. Tumour (paraperesis, Bladder & bowel)----LMNL
- 15. 9. Ankylosing spondylitis 10. Piriformis syndrome 11. Pott’s spine 12. Lumbar canal stenosis 13. Facet jt. syndrome 14. Any soft tissue injury of Cx & Lx area. 15. Mass lesion or malignancy- Note-In PIVD pain is decrease during rest but tumour pain is not diminished.
- 16. Special test for cervical spine 1. Foramina Compression Test, Spurling's Test (Vertebral Compression Test) or Quadrant Test --- pt.- sitting + therapist- applied gentle axial compression on top of head neck in extension, lateral flexion . 2. Foramina Destruction Test- therapist places the one hand under the chin & other hand around occiput area + lifted or destructed in upward direction & distraction force of up to approximately 14 kg.--- +ve –relief of pain.
- 18. 5. Shoulder Depression test--- Pt. - supine or in a sitting position + patient laterally flexes her/his head away from the side that is being tested. and presses down on the patient’s shoulder any localized pain or shoulder pain or arm pain indicates +ve NRC. 6. Brachial Plexus Tension Test ULTT-1 (Radial nerve) ULTT-2-a (Medial root of Median nerve) ULTT-2-b ( Lateral root of Median nerve) ULTT-3- Ulnar nerve
- 19. 1. Straight Leg Raise (Lasegue & sciatic nerve test): POP:- Supine lying POT:- Standing behind the tested side & therapist lifts or passively flexes hip the patient's leg while the knee is straight. Perform hold relax muscle stretch:- A) If this increases the ROM most likely tight hamstrings B) If this has no effect on pain -may be nerve root impingement or irritation ROM Interpretations: 0 –30°-----indicates hip pathology or severely inflamed nerve root. 30 - 50°-----indicates sciatic nerve involvement. 50 –70°---------indicates probable hamstring involvement 70 –90°---sacroiliac joint is stressed.
- 21. 2. Bowsting test:- SLR carried out until pain reproduced ------knee is gradual flexed till pain disappears ----- therapist rest his/ her limb on his shoulder & palpate the sciatic nerve in popliteal fossa –sudden firm pressure on nerve reproduces pain in back or radiates down in leg ---indicate +ve Bowsting sign 3. Kerning test Femoral stretch test. Prone Knee Bending Test Slump Test
- 22. DRUG MANAGEMENT 1.NSAID:- Diclofenac potassium (Cataflam), Diclofenac sodium (Voltaren, Voltaren XR), Diclofenac sodium , Ibuprofen, Indomethacin , Piroxicam 2. ANTACIDS:- pantoprazole and rabeprazole , Aluminum and Magnesium Hydroxide Oral Suspension , Ranitidine, Zantac, Zoton 3. Calcium therapy with vitamin D3 4. Common Muscle Relaxant Medications Baclofen, Chlorzoxazone, Carisoprodol , Cyclobenzaprine, Metaxalone, Methocarbamol , Tizanidine
- 23. 5. DRUGS USED IN PERIPHERAL NEUROPATHY Methylcobalamin:- Methylcobalamin, also known as Methyl-B12 or Mecobalamin, is a form of the common vitamin B12. It differs from typical B12 in that it has an additional methyl group, and contains metal-alkyl bonds. It supports nerve function and neuron health in the brain and contributes improved signalling in the central nervous system. This is especially true in patients who have degenerative neurological conditions such as those that affect the myelin sheath like multiple sclerosis (MS). Gabapentin:- anti-epileptic drug, also called an anticonvulsan. Gabapentin is used in adults to treat neuropathic pain (nerve pain)caused by herpes virus or shingles (herpes zoster). 6. Chemonucleolysis: dissolution of the Nucleus Pulposus by percutaneous injection of a proteolytic enzyme (chymopapain). This enzyme has the property of dissolving fibrous and cartilaginous tissue.
- 24. Acute Stage:- Conservative Management :- Aim of physiotherapy--- ►To accelerate healing . ►To relief pain. ► To restore mobility. ► To restore posture & strength ► Prevention ►To accelerate healing :- ●Rest:- 1 – 2 days but in severe cases 7 to 10 days (1 to 2wks.) ● Corset or lumber belt (L-S belt). ●If severe disabling pain crutches are advised ●Elastic adhesive strapping applied over the back to immobilised the spine. It should be used up to 10 days & replace the tape 2 to 3 times. Elastic Adhesive strapping
- 25. ►To relief pain:- 1. Traction :- ICT & ILT is used for relives intradiscal pressure & increase the disc space. 2. Electrotherapy modalities--- Cryotherapy: reduces muscle spasm and inflammation in acute phase. TENS: relieves pain in both acute and chronic phases. UST: as phonophoresis increases extensibility of connective tissues Moist heat: used as an adjunct before applying specialised techniques to decrease muscle spasm. SWD- pulsed SWD in acute condition and continuous SWD in chronic cases for 20 to 25 mints . LWD pulsed SWD in acute condition and continuous SWD in chronic cases. 08 to 12 mints. IFT – 20 to 25 mints LASER:- Laser therapy treatment is very advance method for pain relief and decrease inflammation,
- 26. ► To restore mobility. 1. Mobility exe.:- Mobility exe. of SI & hip can also include. 2. AROM exercises within pain free range to the lower limb can be done e.g.- ankle toe movements, heel drag, hip abduction/adduction. 3. Mobilization of thoracic spine Mobilization of segments above and below the affected segmental level. 4. Piriformis/ Hams/ Calf muscle stretching 5. Maintain/ improve mobility of neural tissues- SLR with foot dorsiflexion. ► To restore posture & strength a) Spinal extension/ strengthening exe:- In initial stage movt. of spine is contraindicated but after subside of pain can start the isometric spinal exe & then isotonic spinal exe. c) Local support in the form of corset (lumbosacral belt), abdominal binder, tape etc.
- 27. ► Prevention:- Posture and activity modification- Avoid forward bending, sitting for long duration or lifting activities,
- 28. A) Soft tissue flexibility :- 1) Hamstring m/s tendinous unit stretching 2) Quads m/s tendinous unit stretching 3) Iliopsoas m/s tendinous unit stretching 4) Gastrosoleus m/s tendinous unit stretching 5) External & Internal hip rotators . B) Joint mobility:- 1. Lumber spine segmental mobility 2. Hip ROM 3. Thoracic segmental mobility
- 29. C) Stabilisation Programme :- 1) Prone Gluteal squeeze with arm raise with alternate arm raise with leg raise with alternate leg raise alternate arm & leg raises 2) Supine pelvic bracing 3) Bridging programme ● Basic Position ● One leg raised with ankle wt. ● Stepping ● Balancing with Gymball 4. Quadruped with alternate one arm & leg movement 5. Kneeling stabilisation. 6. Wall slide quadriceps strengthening
- 30. 7. Abdominal Programme ♦ Curl ups ♦ Diagonal curl up ♦ Diagonal curl up with inclined board. ♦ Straight leg lowering. 8. Gym Programme ♦ Latissimus pull down ♦ Angled leg press ♦ Lunges Hyperextension bench 9. Aerobic Programme ♦ Progressive walking ♦ Swimming ♦ Stationary bicycling ♦ Running on treadmill.
- 31. The disc is removed by following techniques. a) Hemilaminectomy/Partial laminectomy- Part of the lamina and ligamentum flavum on one side is removed, taking great care not to damage the facet joint. b) Laminectomy- Laminae on both sides with spinous process are removed. Such wide exposure is required for big, central disc producing cauda equina syndrome. c) Microdiscectomy- done with an operating microscope. Exposure is very limited. Morbidity and hospitalisation is less. d) Fenestration- Ligamentum flavum bridging the two adjacent laminae is excised and spinal canal at affected level exposed. e) Laminotomy- In addition to fenestration, a hole is made in the lamina for wider exposure.