Downloaded 516 times

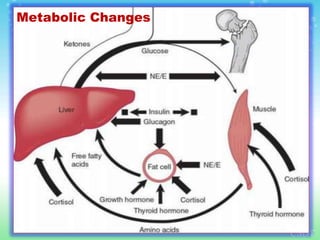
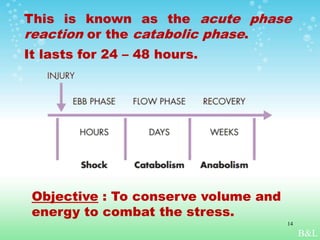
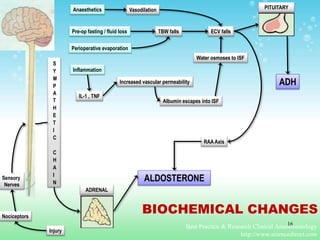
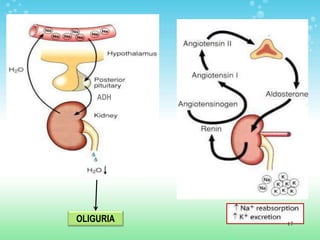
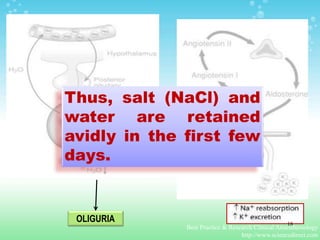
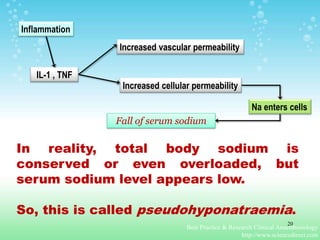
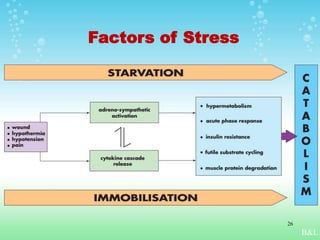



The document discusses the stress response associated with surgery, emphasizing the need for stress-free peri-operative care. It highlights the physiological and biochemical changes during the acute phase reaction, including fluid retention, metabolic alterations, and potassium management. Recommendations for minimizing surgical stress include adequate fluid therapy, minimal fasting, proper analgesia, and early post-operative mobilization and feeding.























































































