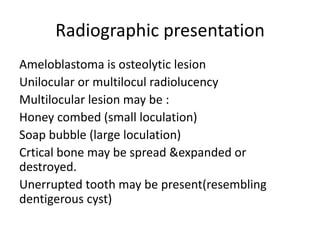
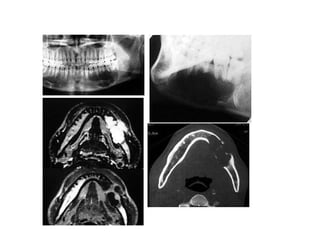
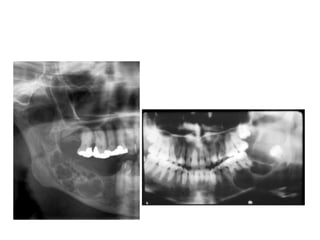
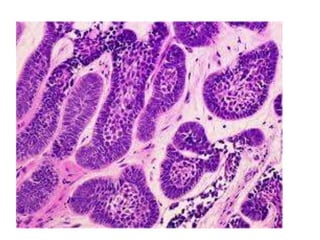
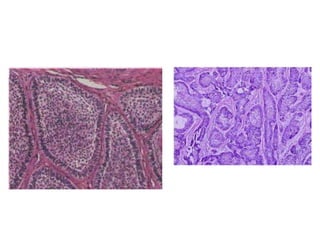
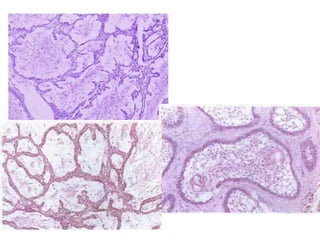
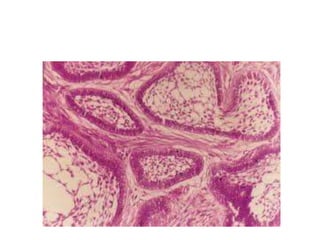
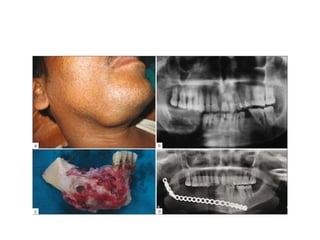
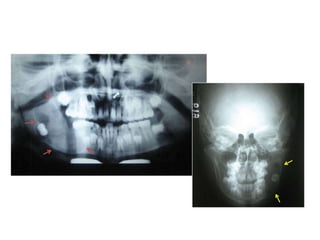
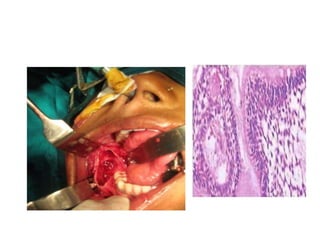
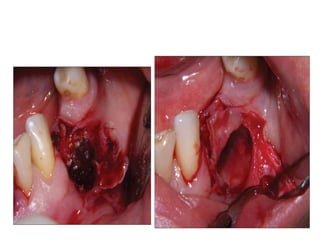
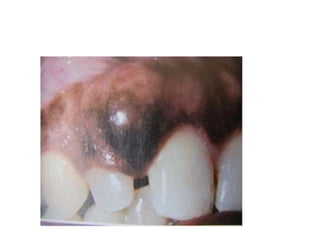
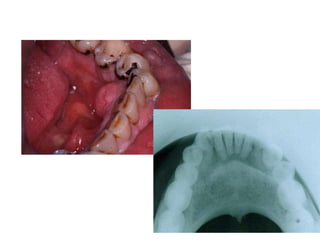
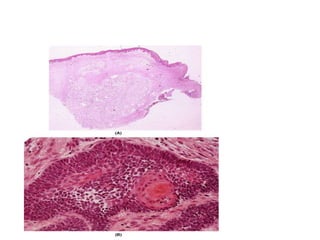
Ameloblastoma is a benign but invasive odontogenic tumor that arises from epithelial tooth-forming cells. It most commonly occurs in the mandible of adults between 30-60 years old. Clinically, it presents as a painless swelling and expansion of the jaw. Radiographically, it appears as a multilocular radiolucency. Histologically, it is characterized by proliferating odontogenic epithelium forming follicles. Treatment ranges from conservative curettage to segmental resection depending on the size and location of the tumor. Unicystic ameloblastoma originates within the lining of an odontogenic cyst and has a better prognosis than the conventional type.


























































![AMELOBLASTOMA [op].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ameloblastomaop-230511134017-11636869-thumbnail.jpg?width=640&height=640&fit=bounds)




















