Constrictive pericarditis
•Download as PPTX, PDF•
0 likes•63 views

Constrictive pericarditis occurs when a thickened fibrotic pericardium impedes normal diastolic filling of the heart. Common causes include uremia, neoplasm, radiation, and surgery. The noncompliant pericardium interferes with filling of all cardiac chambers during diastole while systolic function remains normal. This reduces cardiac output and elevates venous pressures, causing symptoms like dyspnea, edema, and hepatomegaly. Diagnosis involves echocardiogram, ECG, CT/MRI and cardiac catheterization. Definitive treatment is pericardiectomy though medical management may help in early or inflammatory cases.

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Constrictive pericarditis
Similar to Constrictive pericarditis (20)
Recently uploaded
Recently uploaded (20)
Constrictive pericarditis
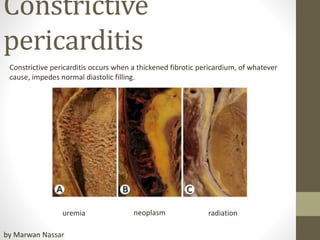
- 1. Constrictive pericarditis Constrictive pericarditis occurs when a thickened fibrotic pericardium, of whatever cause, impedes normal diastolic filling. uremia neoplasm radiation by Marwan Nassar
- 2. normal
- 3. Functions of the Pericardium Although surgical removal of the pericardium (pericardiectomy) and congenital absence of the pericardium are well tolerated 1.Stabilization of the heart within the thoracic cavity by virtue of its ligamentous attachments. 2. Protection of the heart from mechanical trauma and infection from adjoining structures. The pericardial fluid functions as a lubricant and decreases friction of cardiac surface during systole and diastole. 3. Prevention of excessive dilation of heart especially during sudden rise in intracardiac volume e.g. acute aortic or mitral regurgitation.
- 5. PATHOPHYSIOLOGY Noncompliant pericardium interferes with diastolic filling of all cardiac chambers. Systolic function is normal. filling in the early (1/3) diastolic phase is normal until abruptly encounters the rigid pericardium and filling stops in later (2/3) part of diastole Although systolic function is normal, decrease in ventricular filling reduces cardiac output. Elevation of right heart diastolic pressure raises systemic venous pressure, which leads to jugular venous distention, hepatomegaly, and edema.
- 6. Clinical Presentation develop slowly over a number of years, so that patients may not be aware of all of their symptoms until questioned. similar to those associated with CHF. -Dyspnea** -Lower-extremity edema and abdominal swelling and discomfort * -Nausea, vomiting, and right upper quadrant pain, if present, are thought to be due to hepatic congestion, bowel congestion, or both. -The initial history may be more compatible with liver disease (cryptogenic cirrhosis) Less common Chest pain, presumably due to active inflammation Easy fatigability Fever Tachycardia Palpitations Paroxysmal nocturnal dyspnea Diaphoresis
- 7. Physical Examination In more advanced stages, the patient may appear ill, with marked muscle wasting, cachexia, or jaundice Cardiovascular findings -Elevated JVP -Sinus tachycardia is common while the BP normal or low. -The apical impulse is often impalpable, and the patient may have distant or muffled heart sounds. -A friction rub is usually not found. -A pericardial knock -Pulsus paradoxus is a variable finding. -Kussmaul sign (ie, elevation of systemic venous pressures with inspiration) is a common nonspecific finding
- 8. Physical Examination Gastrointestinal, pulmonary, and other organ system findings -Hepatomegaly with prominent hepatic pulsations in 70% of patients. -ascites, -spider angiomata, -and palmar erythema, Peripheral (dependent) edema is a common finding
- 9. DIAGNOSIS **Echocardiogram is useful in providing key hemodynamic findings. The presence of pericardial effusion indicates effusive constrictive pericarditis and may reveal thick pericardium. *ECG is abnormal but nonspecific atrial fibrillation is common. Chest x-ray may show evidence of pericardial calcification. *CT and MRI are most helpful in differentiating constrictive pericarditis from restrictive cardiomyopathy with which it resembles so closely both hemodynamically and clinically. *Cardiac catheterization shows the typical dip-plateau pattern and equalization of diastolic pressures.
- 11. TREATMENT The most definitive therapy consists of pericardiotomy. in the early stage of the disease and hence the importance of early recognition. Individuals with significantly advanced symptoms related to constriction may derive little benefit from pericardiectomy particularly how has high surgical risk. medical management is ineffective unless a prominent inflammatory component is present. Transient constrictive pericarditis who are medically stable may be given a trial of conservative treatment for 2-3 months (using NSAIDs and/or steroids). Subacute constrictive pericarditis may respond to steroids if treated before pericardial fibrosis occurs Diuretics are the mainstay to relieve congestion and optimize clinical volume status. medications used to treat patients specific to the underlying cause of the pericardial disease directed toward the causative disease (eg, antituberculosis medication) is appropriate Complications (eg, atrial arrhythmias) require their own therapy as appropriate beta-blockers and calcium channel blockers should be avoided
- 12. Summery