Downloaded 184 times
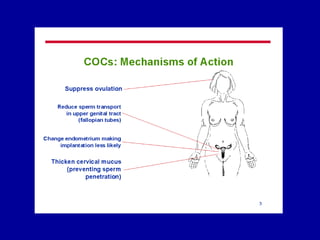
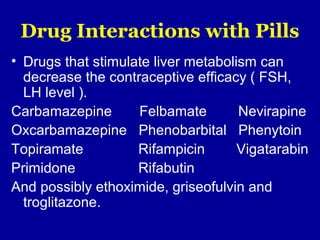

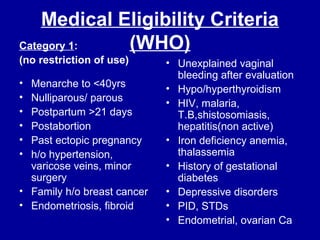
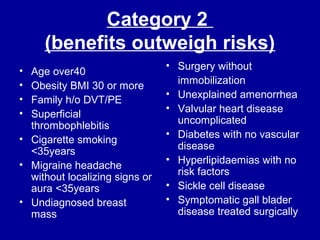
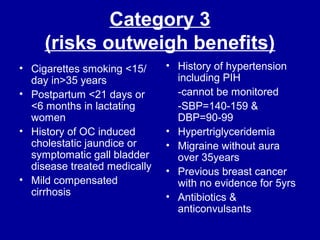
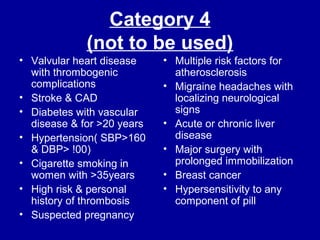
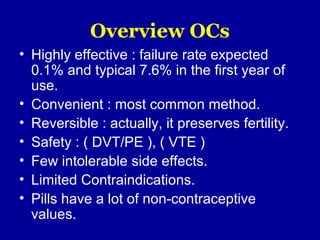



This document provides an overview of oral contraceptives (OCs). It discusses the history of contraception, the development of the pill in the 1950s-60s, and the pharmacology of estrogen and progestin components. It covers the mechanism of action, drug interactions, medical eligibility criteria, benefits, and some newer contraceptive options like Yasmin, the 24/4 regimen, vaginal ring, and contraceptive patch. The document emphasizes that OCs are a highly effective, convenient, and reversible method of contraception that also provide various non-contraceptive health benefits when used by eligible women.