
Recommended
Recommended
More Related Content
Similar to Assignment Stakeholder Management in OrganizationsTo prepare fo.docx
Similar to Assignment Stakeholder Management in OrganizationsTo prepare fo.docx (9)
More from lynettearnold46882
More from lynettearnold46882 (20)
Recently uploaded
Recently uploaded (20)
Assignment Stakeholder Management in OrganizationsTo prepare fo.docx
- 1. Assignment: Stakeholder Management in Organizations To prepare for this assignment read the case study “Aetna Inc.: Managing Inherent Enterprise Risks Through Stakeholder Management.” Prepare a 2- full pages paper that addresses these items: · Describe the stakeholder management approach of the organization before the issues arose. · Which of the three concepts of stakeholder management was most closely aligned with that approach? · Describe the stakeholder management strategy that was devised to combat the negative perceptions of the organization. In what ways did the approach change? · Do you think the new stakeholder management strategy of the organization better supports its responsibility to its constituents? Why? How? Response includes three ways in which the stakeholder management approach supports the strategic objectives of the company. Support your assignment with specific references to all resources used in its preparation. Use correct APA formatting for all resources. The Walden Writing Center provides preformatted templates with APA-compliant pagination, margins, and spacing. ICT285 Databases TSA 2018 Assignment 2 Worth: 20% of your final grade.
- 2. Due: Sunday 25 November 2018 11:55PM Submit to: LMS, via the Assignments tool. Submit Parts 1 and 2, Part 3 sample data and Part 4 CREATE VIEW statements as a SINGLE Word document. Parts 3 and 4 should be completed in Oracle on arion. Ensure you complete the declaration that is part of the submission process. You do not need to include a separate cover sheet but you should include your name and student number as part of your document filename. Your name and student number should also be included within in the assignment document. Late assignments that do not have an extension will be penalised at the rate of 5% per day. This is an INDIVIDUAL assignment. This assignment requires you to implement the database you designed to address some of the requirements of the GardenSwap case study in Assignment 1. You will need to incorporate any changes to your original design required as a result of the feedback on Assignment 1 both individually and as a class (e.g. on the online forum), and to address the additional/amended requirements listed in this document.
- 3. The assignment addresses the following learning outcomes for the unit: 3. Demonstrate practical skills in using SQL 5. Demonstrate practical skills in normalisation and convert a conceptual database design to a logical design in 3NF 6. Create a database from a given design using a DBMS and implement specified constraints using appropriate tools and approaches 7. Explain and implement security as it applies in the database environment. Marks are distributed as follows: Part 1: Revised ERD and schema 10 Part 2: Data dictionary 20 Part 3: Implementation 30 Part 4: Views 40 Total 100 Case study Re-read the description of the GardenSwap case study in Assignment 1 Q5 if you need to refresh your memory. Also view any additional material that has been posted
- 4. about hints and partial solutions. Astrid Winterblossom is pleased with your work so far and has asked you to go on to implement your design. However, like so many clients, she wants to make some changes to the requirements. As it turns out, people were not very keen on formalising the swapping part of their activities, although they would still like to view the various skills that other members have and are prepared to help others with. The swaps themselves will probably continue informally, but will NOT be recorded as part of the database at this stage. However, the event advertising part of Astrid’s garden community has proved to be very popular, and she would like you to develop this part as a priority, with the resultant system renamed GardenFriends. She has a revised set of requirements based on feedback from the community. Astrid’s revised requirements are as follows: registered on the GardenFriends database, with the same requirements for registration information as stated previously. This
- 5. includes a list of the services/skills they are prepared to offer. attendees are taken round a member’s garden where features of particular interest are pointed out; Skills and Techniques, where attendees learn skills such as composting or chainsaw maintenance; and Know Your Plants, which focuses on the cultivation of a particular species or group, such as roses or Banksias. presents the event on the day (these may or may not be the same person). Some events also include additional helpers who assist in providing 1:1 assistance to attendees. These helpers come from the pool of registered members and each helper may volunteer to assist in many different events. description, date, location, and number of places available), but additional information has also proved useful and is to be included in the final system. In particular, Astrid would like to ensure the postcode of the
- 6. location is collected, and any instructions to participants included (“bring your own trowel and secateurs” or “don’t forget your hat and sunscreen”. She would also like to record whether the event meets accessibility guidelines for people in wheelchairs or with limited mobility. events to the general public as well as registered GardenFriends members, in the hope that many will be inspired to join GardenFriends. Guests sign up on the website with their name, suburb, mobile phone number and email. Part 1: Revised ERD and schema (10 marks) a) Create and submit the ERD for this database that you are going to use as the basis of your implementation. b) Include a one or two paragraph explanation as to the changes you have made to the ERD on
- 7. the basis of your feedback from Assignment 1 and/or as a result of having to support the new functionality and views described in this assignment. c) Show the relational schema in 3NF that will be the basis of your implemented design. Show your relations using the following convention: RELATION_NAME (PrimaryKey, Attribute, Attribute, … ForeignKey) Part 2: Data dictionary (20 marks) Create a data dictionary for your database. This should include: a) For each table: a definition of each column (attribute), consisting of the column name, brief description of what it represents, its data type and size, domain (allowable values), any default value, whether it is required, whether unique, and any constraints (primary key, foreign key). You can follow the example in Lab 07. Use the data types available in Oracle. b) For each of the columns that is a foreign key, give the appropriate referential integrity rules
- 8. (i.e. the “on delete…. ; on update“ etc actions that should apply when the corresponding primary key is altered). The appropriate action should be included whether or not there is a statement in Oracle to implement it. c) Any business rules (enterprise constraints) that should apply to the database that haven’t already been covered by cardinality or participation constraints. Note that your data dictionary must be consistent with your ERD and schema. Part 3: Implementation (30 marks) Implement the tables for the GardenFriends database in Oracle SQLPlus on arion.murdoch.edu.au. Note the following: a) All tables should be created as per your ERD and data dictionary; the marker will check your ERD against your tables. You do NOT need to include the SQL CREATE TABLE statements that you used to create the tables.
- 9. b) All entity and referential integrity constraints should be created and appropriately named. c) All columns (attributes) should be of an appropriate data type/size and be set as required, unique or not as appropriate. d) All domain constraints should be implemented. e) All tables should be populated with sample data that will allow the marker to test that your database fulfils the application requirements as specified and supports the transactions and views listed below. Also provide the same sample data in your Word document. If you use a screen dump, it MUST be a size that is readable without zooming. Note you do NOT need to include the SQL INSERT statements that you used to add the data. f) SELECT, UPDATE, INSERT and DELETE permissions should be GRANTED on all database objects (particularly tables and views) to the user MARKERTL.
- 10. This is most important. If you do not grant this permission, the marker will not be able to mark this part of your assignment and you will not get any marks for it. g) Please state in your documentation whether you have used your V account or H account. Part 4: Views (40 marks) Create VIEWS for the following in Oracle (views should be named as ViewA, ViewB etc). Note that some of these have changed from Assignment 1 in line with Astrid’s new requirements. You should also provide the CREATE VIEW statements you used to create the views in your Word document. These should be as text, not screen dumps. A. All the members represented in the database, and details of the skills they offer, listed in alphabetical order of last name. B. A list of all the equipment available for loan, the contact details of the member who is loaning the equipment, and any specific information about the conditions of loan. C. A list of attendees (name, phone number, and whether they are registered members or guests)
- 11. who have signed up for Fran Forklift’s workshop on ‘Chainsaw use and maintenance’. D. All the events (title, date) that were more popular (i.e. higher attendance) with guests than with registered members. E. All the upcoming events (title, date, location) in a given postcode (e.g. 6150) for the next month (i.e. the whole of the next calendar month). F. Details (title, description, date, location, leader name, instructions) of all the events that mention roses. G. Names of any members who have organised, led or helped in more events than they have attended as participants. The result table should also show the number of events. H. All the events (title, date, leader) that meet accessibility guidelines. I. A list of guests who attended (or are signed up to attend) events that are not in their home suburb. The result table should also show their home suburb and the event suburb. J. The number of unfilled places in each category of event that has been held so far. NOTES:
- 12. suburb, gardener etc, you should ensure that your sample data demonstrates this. However, it is important that your query also works for other possible values, without changing anything apart from the literal value. requirement. For example, if “the previous month” is asked for, the query should not use a particular month such as ‘November’ in the SQL. https://docs.oracle.com/cd/B19306_01/server.102/b14225/ch4da tetime.htm http://www.akadia.com/services/ora_date_time.html You can use TO_CHAR to format your output (see e.g. https://www.techonthenet.com/oracle/functions/to_char.php ) Please note the following about the marking of this assignment: your documentation to your implementation. This means for example, that tables, columns and constraints should be named in your database as they are in your documentation. Relationships defined in your ERD should be defined in your database using foreign keys.
- 13. er will view the sample data in your tables. above. privileges on all relevant objects (tables and views) to the user MARKERTL. If you do not do this, the marker will not be able to mark part of your assignment (and you may be awarded 0 for this section). https://docs.oracle.com/cd/B19306_01/server.102/b14225/ch4da tetime.htm http://www.akadia.com/services/ora_date_time.html https://www.techonthenet.com/oracle/functions/to_char.php UV3935 November 27, 2009 This case was prepared by Barbie Carmichael, Batten Fellow and Senior Counselor, APCO Worldwide, and Assistant Professor James Rubin. It was written as a basis for class discussion rather than to illustrate effective or 2009 by the University of Virginia Darden School Foundation, Charlottesville, VA. All rights reserved. To order copies, send an e-mail to
- 14. [email protected] No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means—electronic, mechanical, photocopying, recording, or otherwise—without the permission of the Darden School Foundation. AETNA INC.: MANAGING INHERENT ENTERPRISE RISKS THROUGH STAKEHOULDER MANAGEMENT (A) Prologue In the spring of 2003, Roger Bolton, Aetna Inc.’s senior vice president of communications, and David Carter, Aetna’s vice president of corporate public relations, compared notes as they walked back to their offices following discussions with Aetna’s attorneys, with whom they had been working for the past four years. Together, they had been managing the continuous communications challenges surrounding class action litigation that physicians had brought against managed care companies and had watched Aetna’s position erode, both in its financial results and its reputation among key stakeholders—patients, physicians, corporate benefits customers, employees, and investors. It had not been a fun ride.
- 15. The company had been cast in news reports as a typical corporate stereotype: Aetna was scripted as the leading villain in the saga of managed health care insurance, callously inflicting onerous policies on patients and doctors that put profit above the well-being of their customers. By 2003, however, the company had reached a turning point. Employee morale was recovering under new leadership that had brought a fresh, clearly communicated strategic vision and improving relations with physicians. After a series of Wall Street losses and surprises, the new strategy was beginning to translate into improved bottom line results. Aetna was now showing a profit, but its progress was still fragile. Now, Bolton and Carter faced their next challenge. Aetna had just concluded confidential negotiations with the plaintiffs in the class action suit. Within the week, Aetna would break from the eight managed care insurers named in the lawsuits and announce a settlement. Both executives knew that the positioning of this settlement would be a significant strategic issue needing debate at the management group level, Aetna’s most senior executive council. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019.
- 16. -2- UV3935 Their announcement options covered a wide range, from low- key to high-visibility. Their proposal for the management group needed to include the business case for their recommended announcement strategy as well as a draft press release and the media headlines they would be seeking so that the management group could see how the strategy would be carried out in terms of the identified spokespeople and supporting messages. As they entered the working conference room that had become ground zero for managing the communications on this issue, they reflected on the enormous changes that had taken place at Aetna. They knew that persuasive arguments could be made for any of the potential communications strategies before them. In fact, members of the management group could reasonably and thoughtfully champion opposite ends of the spectrum, from a low-key announcement to a high-visibility strategy. As they began to formulate a strategy, they reflected on the roller-coaster ride the company had experienced, which would form the context for any announcement strategy they
- 17. would recommend. A New Era for Aetna: 1995–99 In 1995, just eight years before its 150th anniversary, Aetna had begun to embark on a new strategic course, breaking away from its long history as a traditional multiline insurance company that, as recently as 1990, Fortune had ranked as the nation’s fifth-most-admired financial services company. Then named Aetna Life and Casualty, the company had recorded an enviable, sustained track record, successfully navigating multiple natural and financial crises— such as the Great Depression and the San Francisco earthquake—that had tripped up lesser competitors. Following a board-level strategic business review conducted in 1994–95, however, Aetna had concluded the best fit for its long-term growth was in health care and financial services, according to Ed Shaw, who served as the company’s general counsel from 1999 to 2004.1 Completing the sale of Aetna’s property and casualty business to the Travelers Insurance Group in April 1996, Aetna CEO Ronald Compton said the transaction represented a “major phase in Aetna’s transformation from a traditional multiline insurer to a growth company focused on leading edge health care and retirement services” (Exhibit 1).2 Three months later,
- 18. Aetna completed its acquisition of U.S. Healthcare, giving Aetna, according to Compton, “the scale and expertise necessary to thrive in the dynamic health care industry” and positioning the 1 Case writer interview with Ed Shaw, December 22, 2005; unless otherwise noted, all subsequent Shaw quotations and attributions derive from this interview. 2 “Aetna Completes Previously Announced Sale of Property/Casualty Operations to Travelers,” Aetna press release, April 2, 1996. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -3- UV3935 company “to deliver superior long-term value to shareholders” (Exhibit 2).3 Now renamed Aetna Inc., the company saw its future as bright. Compton said: The health care industry, and managed care in particular, continues to be a business with excellent current and future prospects. Our unique ability to provide
- 19. access to affordable, high-quality health care on a national level will be the key to our future success, allowing us to create the first truly national managed care company.4 The newly named Aetna Inc. soon found, however, that capturing the financial synergies anticipated from integrating U.S. Healthcare would be more difficult than expected, an all too common scenario in many mergers and acquisitions. In 1997, Aetna announced it would take a $108 million charge attributed to problems integrating the two companies. The news surprised shareholders, who had relied on Aetna officials’ earlier upbeat statements on the company’s financial condition. Aetna later agreed to pay $82.5 million to settle a class action shareholder lawsuit emerging from this dispute. Despite this initial hiccup, Aetna stayed on its new strategic course. Under the leadership of CEO Richard Huber, who had assumed that role following Compton’s retirement in 1998, the company continued to grow its position in the health care industry, acquiring NYLCare Health Plans (in 1998) for $1.05 billion and Prudential Healthcare (in 1999) for $1 billion. Both newly acquired businesses were transitioning from old-line indemnity insurers to the managed care model. With the Prudential acquisition, Aetna had become the largest U.S. provider of health benefits.
- 20. The Health Care Industry Consolidates The health care service industry that Aetna was strategically targeting had always been distinguished by its complexity. It was composed of multiple stakeholders—patients, physicians, hospitals, pharmaceutical companies, regulatory agencies, and health insurers—each focused on preserving individual interests while also being inexorably dependent on one another. Beginning in 1990, however, the complex web of services that comprised the delivery of health care in the United States began a spiral of activities that fed upon each other, spinning off some of the players, consolidating others, and converging sources of power among stakeholders that would culminate in a High Noon confrontation. Prior to 1990, the traditional business model for physicians had largely been a small or solo private practice. Consumer awareness of, or use of, the Internet had not yet begun to gain traction. As a result, patients’ primary sources for medical information specific to themselves or 3 “Aetna and U.S. Healthcare Complete Merger,” Aetna press release, July 19, 1996. 4 Aetna press release, July 19, 1996. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational
- 21. Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -4- UV3935 medical information in general were their personal physicians, and patients’ preferences for specific doctors were not yet restricted through health care plans requiring the selection of “primary care physicians.” In that context, physicians had grown accustomed to running the show, with access to their own medical records on each patient and largely unchallenged judgment on individual medical treatments. But fundamental changes were emerging in the 1990s that would inevitably reconfigure the business model for delivering health care. Computer-based business management had spread beyond the early adopters of government and large corporations, profoundly changing computer hardware (the emergence of personal computers), software (increasingly sophisticated and accessible business management and database management programs), and networks (the U.S. Defense Department’s ARPANET’s evolving into the World Wide Web). These changes combined to provide the foundation that would later enable broad access to health care
- 22. information on both individual patients and broad populations of patients, displacing the role of the individual physician practitioner as the primary hub for medical information. In parallel with these changes, corporate buyers of health insurance were observing an unending escalation of health care costs, with no mitigating solution on the horizon. As employers began adopting so-called cafeteria-style health care plans, those rising costs became more directly visible to employees. With each annual benefit enrollment cycle, employees would evaluate the cost–benefits tradeoffs in their various options, making the rising costs much more visible and personally relevant. In addition, by 1990, the discipline of fact-based quality process management had demonstrated its ability to make material improvements in corporate productivity, particularly in the manufacturing sector, with 1988 Baldridge Award winners such as Motorola becoming the role models for improved profitability through efficiency gains in manufacturing. The next frontier was applying the discipline of quality process management to nonmanufacturing business processes and to the service industry as a whole. Re- engineering and the adoption of best practices had become the hallmarks of a well-managed enterprise, offering win-wins to all stakeholders through quality products or services at lower costs
- 23. with increased profitability. One potential solution to visibly spiraling health care costs came from combining the advanced capability in computing with the discipline of quality process management. More powerful and sophisticated information-processing systems allowed insurers to access consolidated health care data, providing them with the fact- based information they would need to effectively apply quality process management to health care services. Identifying and delivering “best practices” in health care promised to deliver quality care while at least stemming the rate of escalating costs, if not lowering costs. Health maintenance organizations (HMOs) provided insurers with a logical business model for delivering cost-effective best practices in health care. Prepaid care fees sought to deliver preventative medicine by encouraging patients to seek regular care through a predefined This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -5- UV3935
- 24. group of physicians who could coordinate among a network of specialists. The physicians, in turn, were controlled through tightly managed processes and procedures optimized for delivering medically necessary treatment and eliminating or discouraging unnecessary costs. Although they had existed for decades in the United States, HMOs had not begun to gain broader acceptance until the late 1970s with the passage of the Health Maintenance Organization Act of 1973. The act allowed HMOs to access the employer-based market from which they had been previously barred, requiring employers with 25 or more employees to offer federally certified HMO options. By 1977, once the federal government’s pace quickened in issuing supporting regulations and certifying plans, HMOs had begun to grow rapidly.5 By 1993, as employees sought to contain the increasing bite of their income that the cost of health care was consuming, 51% had opted for managed care programs. By 1995, employee adoption of these programs had risen to 73%.6 With their patients increasingly consolidating into managed care plans affiliated with multiphysician clinics or multiphysician networks, the sole practitioner business model to which physicians had become accustomed faced a fundamental change in the balance of power. No longer at the hub of the health care system, doctors began to consolidate. In 1991, just over one-
- 25. third of all physicians were solo practitioners. By 1995, that number had shrunk to just over a quarter, with nearly 30% having instead opted to become employees of hospitals or HMOs. Alternatively, many opted to join independent practice associations (IPAs), providing them with a means to contract collectively with managed care plans as they became part of a plan’s provider network. In stark contrast to the sole practitioner business model, by August 1996, approximately 4,000 IPAs were in operation, with an average of 300 physicians each.7 To level the playing field in dealing with managed care organizations, these physician practices increasingly sought the expertise of a new player in the market, the private physician management firm (PPM), which would negotiate and market physician practices with managed care firms. In just two years (1994 to 1996), the number of physicians affiliated with the three largest PPMs had grown nearly 700%, from 3,787 to 25,763.8 During this same decade, hospital ownership also underwent dramatic change. In the same two-year period, nearly half (41%) of all nonfederal U.S. hospitals saw changes in their asset ownership. At the decade’s end, Lori Mitchell, then chairman of the Healthcare Financial Management Association, summarized the roller-coaster rides the nation’s hospitals experienced: Hospital consolidations are continuing in many areas…Hospital profitability is declining in many parts of the country, and some hospitals have
- 26. dipped into or 5 Penny Singer, “Health Maintenance Plans: A Growing Market,” New York Times, March 30, 1986. 6 Martin Gaynor and Deborah Hass-Wilson, “Change, Consolidation, and Competition in Health Care Markets,” Journal of Economic Perspectives 13, no. 1 (1999): 141–64. 7 Gaynor and Hass-Wilson. 8 Gaynor and Hass-Wilson. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -6- UV3935 depleted their reserves over the past few years…Turnover in senior leadership positions continues to be high.9 For the health care insurance market, these fundamental changes represented both an opportunity and a threat. Consolidation through mergers and acquisitions had the potential to provide economies of scale to achieve increased efficiencies in the HMO business model. Failure to act, however, would likely position an insurer on the weaker side of
- 27. the power curve, making it an acquisition target or bloating its competitive cost structure due to its relatively diminished bargaining power. In this changed business context, the M&A action among health care insurers was fast and furious. Of the 592 HMOs in operation in 1996, 62 either merged or were acquired. By 1997, the 128 independent Blue Cross/Blue Shield plans that had been in operation in 1975 had shrunk to only 58.10 Initially, these dramatic changes in the health care system succeeded in stemming the double-digit rise in health care costs and, consequently, some insurance premiums. But by the end of the decade, what appeared to make sense on paper was challenged by the difficulties inherent in consolidating so many disparate players into the overall system. Lori Mitchell summarized the scene surrounding insurers in 1999: After a number of years of premium declines, commercial insurance premiums are beginning to rise again in most areas of the country. Rising health care costs— especially costs associated with pharmaceuticals—have necessitated this increase. Many insurers have found that their own administrative software is not designed to support various nontraditional insurance products and provider agreements. As a result, extended claim payment delays are common in most parts of the country. Consolidation of commercial insurers through merger and
- 28. acquisition continues to occur, though the expected reductions in overhead costs and strengthening of market position have not always materialized.11 Patients Lose Patience Ironically, as Mitchell explained, coexisting with this massive health care industry consolidation was a trend moving in the opposite direction: a proliferation in the number of differing health care products and provider agreements. Responding to consumer backlash against restrained choices in initial HMO plans, insurers had begun expanding the boundaries of managed care by offering subscribers more choices, such as preferred provider organizations (PPOs). A variation on the earlier managed care models, PPOs offered subscribers broader 9 Lori Mitchell, FHFMA, CPA, “Chapters of Change on the Healthcare Delivery Landscape,” Healthcare Financial Management, April 14, 1999. 10 Gaynor and Hass-Wilson. 11 Mitchell. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019.
- 29. -7- UV3935 choices in selecting a physician either in-network (at a negotiated discount rate) or out-of- network (at a higher price). Competition among the various provider networks enabled, at least initially, reduced in-network rates. But the diversity of provider networks and competing products also came with the complexity of administering and processing a wide variety of differing plans and claims. The result was increased administrative costs and slow claims processing. To control costs among the divergent provider networks, PPOs adhered to some of the tightly controlled policies and procedures of HMOs. This typically included records reviews to validate that the prescribed treatment was appropriate to the patient’s condition. In addition to ensuring that the treatments conformed to proven medical practices, this records review also sought to disallow treatments aimed more at increasing reimbursements than treating patients. Another common PPO requirement was obtaining an insurer’s precertification or prior approval before nonemergency hospitalization. The negative impacts of all these HMO practices on physician and patient stakeholders—
- 30. increased administrative costs for both insurers and providers, slower claims processing, and perceived insurer intervention in the doctor–patient relationship through insurer-approved medical treatments—combined to trump the managed care business model’s promised win-win. As the HMO model’s market penetration continued to grow, so did the inherent risks from the HMO business model as the negative impacts on stakeholders became more visible. Doctors came to believe that insurers were second-guessing their medical judgment, adding significant administrative overhead costs to their medical practice and potentially endangering their patients’ health by prohibiting what they deemed to be appropriate care. Patients saw their insurers as blocking access to needed treatments, and patients without employer-based insurance found themselves excluded from the in-network medical care discounts, pricing them out of the market. Angry Patients and Physicians Converge with Politicians and Lawyers In the early 1990s, health care reform had focused primarily on cost containment and had emerged as a political issue, best exemplified by Hillary Clinton’s 1993 universal health care plan. In that context, managed care was part of the solution.
- 31. By the end of the decade, voters had directly experienced what they saw as the negative consequences inherent to the current managed care “solution.” Choice had replaced cost as the driving issue in health care reform, and the Patients’ Bill of Rights had replaced universal health care as the legislative solution. Positioned as a statement of the rights to which patients were entitled as recipients of medical care, a key component of the 1999 Patients’ Bill of Rights passed by the House of Representatives gave patients a broad new ability to sue their HMOs in state court. In contrast, the Senate version restricted patients’ ability to sue for punitive damages This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -8- UV3935 in cases where coverage of medical procedures was delayed or denied.12 Competing bills continued to be debated, with Congress still arguing about the best legislative solution in 2001, ultimately ending in a stalemate. What Congress failed to enact through legislation, plaintiffs’
- 32. attorneys sought to achieve through litigation. Flush from collecting $243 billion from the tobacco industry and $10.4 billion in fees for themselves, plaintiffs’ attorneys had learned the formula for “Litigation Incorporated” as means to achieve policy changes through litigation rather than regulation.13 With the courtroom proceedings staged as mere background scenery, their core formula for action involved first softening up the political environment through high-profile media coverage of consumer victims harmed through the onerous actions of greedy corporations. These ready-made news stories were too appealing for the media to ignore and would occur well before any trial and often even before the initial filing of the suit itself. With that context in place, federal and state legislators could then be easily recruited to stage hearings and investigations, scoring political points if not enacting legislation. From there, states’ attorneys general could be dispatched to the rescue, staging more lawsuits and inquiries on multiple fronts. Observing the financial risks from this sustained run of negative exposure, all well in advance of any actual trial on the merits of the cases, nervous investors by now had driven down stock prices to the point that corporate executives and their boards were forced to consider settlements. High Noon
- 33. In this highly dynamic context, Aetna had expanded its base of subscribers to more than 21 million with its 1999 acquisition of Prudential Healthcare. But in this context, bigger was not necessarily better. Aetna had taken steps to eliminate redundancies from its acquisitions, for example, eliminating 4,000 positions and closing half its claims processing centers following the U.S. Healthcare acquisition. But many analysts believed the company had overpaid for these acquisitions, leaving it with an uncompetitive cost structure. In addition, while competitors had responded to consumer backlash by offering more choices for subscribers, Aetna continued to adhere to a more stringently controlled business model as a means of controlling costs. In fact, U.S. Healthcare, Aetna’s first acquisition, had been perceived as being one of the most hard- nosed of all the HMOs, limiting doctors’ fees and requiring doctors to take all patients, regardless of what kind of Aetna health plan they had selected, prompting many doctors to stop working with Aetna.14 12 Dena Bunis, “Patients’ Bill of Rights Goes to Committee,” Salon, November 5, 1999, http://www.salon.com/ health/log/1000/11/05/patients_rights/ (accessed November 2, 2009). 13 John Helyar and Soo-Min Oh, “They’re Ba-a-ack!” Fortune, June 26, 2009.
- 34. 14 Pamela Moore, “Aetna: A Long Way to the Recovery Room,” BusinessWeek, July 16, 2001. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -9- UV3935 The net result was that being the biggest, with more than 21 million subscribers, simply multiplied the collective negative impact of its restrictive policies and procedures. As BusinessWeek summarized it, Aetna’s situation was bleak: Having overpaid for its acquisitions and managed them badly, the Hartford insurer expects to trail the industry in profitability for years to come. Its costs are far higher than those of rivals, its premiums often far cheaper, and it faces increasing employer resistance to raising them. And healing the company’s image may be hardest of all: Aetna alienated consumers and doctors by sticking with the unsavory cost-control tactics of early HMOs long after more nimble rivals were
- 35. offering greater choices of doctors and services.15 The plaintiffs’ lawyers could not have scripted a better cast to play villains and victims as they placed the next target for their mass tort litigation enterprise in their crosshairs. Enter stage left: David Boise, who was then leading the Justice Department’s case against Microsoft, and Richard Scruggs, who had led the litigation against tobacco companies, particularly the state lawsuits. True to their formula for softening up the environment before even filing a lawsuit, they obtained high-profile Wall Street Journal coverage of their litigation plans: “Attorneys Prepare Suits against HMOs.”16 Aetna, the nation’s largest health insurer, saw its stock drop 18%; the number- two insurer, United Healthcare, experienced a 19% drop. Four months later, on February 25, 2000, William Donaldson was named Aetna president and CEO, replacing Richard Huber, who resigned. Donaldson, then immediate past chairman and CEO of the New York Stock Exchange, had served on Aetna’s board of directors since 1997. It was time for urgent care. Triage: 2000–01 As Aetna entered the year 2000, the company had become the industry’s leading health
- 36. care insurer with the majority of its business in that sector, most of which was based on the managed care business model. But the managed care entities Aetna had acquired in the last half of the 1990s to provide economies of scale had each had their own struggles in converting to the managed care model. Integrating them into a single, effective operation had been more difficult than anticipated.17 In addition, Aetna had credibility problems with physicians and Wall Street 15 Moore. 16 Laurie McGinley and Milo Giyelin, “Attorneys Prepare Suits Against HMOs,” Wall Street Journal, September 30, 1999. 17 Case writer interview with Roger Bolton, January 10, 2009; unless otherwise noted, all subsequent Bolton quotations derive from this interview. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -10- UV3935 investors, two of its key stakeholders. “Aetna was promising
- 37. lower cost for consumers and textbook, evidence-based medicine. Most saw this as good,” Shaw said. “But it was not good as seen by doctors. Instead, they saw it as interfering with the doctor–patient relationship.” Wall Street investors had seen the company miss earnings guidance, escalating high-profile litigation, a major decline in the stock, and a CEO resignation. Ironically, by the time the class action litigation had emerged, the managed care industry was already moving away from what Aetna Corporate Counsel Robert Stillman called the “Mother May I?” policies that had triggered the consumer backlash. The industry had also begun to streamline processing, implementing online access to fee schedules and current procedural terminology (CPT) codes. The exception to that trend, however, was industry leader Aetna. Following its acquisition of U.S. Healthcare, Stillman explained, Aetna clung to the cost control model of managed care and was aggressively communicating its practices, leading some critics to maintain that the policies were placing the insurer in the position of deciding what the right medical care was.18 Health care of the 1990s, Stillman said, could not survive if it angered doctors: “All these massive lawsuits came down to fundamental business practices that were symptomatic of aspects of the business model that angered physicians.”
- 38. The company needed new management to take a fresh look at the situation and decide what actions to take. Under Donaldson’s leadership, Aetna found new guidance and a fresh perspective in John (Jack) W. Rowe, MD, who became CEO and president of Aetna US Healthcare in September 2000. Rowe, an esteemed gerontologist, was the former CEO of Mount Sinai NYU Health, one of the nation’s largest private hospital systems. While he had never run a publicly traded company the size of Aetna, which had at the time 18.3 million members and $27 billion in revenues, as a physician, he brought a stakeholder’s perspective to assessing Aetna’s situation. In a September 2000 New York Times profile, Rowe compared the challenge facing him at Aetna to his first job as a junior faculty member at Harvard Medical School, where he was assigned to develop the first-ever academic research and teaching program on aging: It was an uphill battle to establish a new era of medicine in a school that had been around for hundreds of years. I felt like Sisyphus, pushing a rock uphill every day only to have it roll back down again. Over time, we built the nation’s largest academic research program on aging…Aetna looks very much to
- 39. me like my first job at Harvard. Health insurance is broken in this country and we need to re- 18 Case writer interview with Robert Stillman, December 19, 2005; unless otherwise noted, all subsequent Stillman quotations and attributions derive from this interview. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -11- UV3935 engineer it. I don’t know if it will be like pushing a rock uphill, but if it is, I am prepared.19 Rowe signaled a new perspective even before his first day at Aetna. “The Saturday before I started with Aetna,” Rowe recalled, “I was invited by the American Medical Association to meet with its board. The first thing I said was that I had been a long- term, dues-paying AMA member. That differentiated Aetna for them.”20
- 40. Six months after joining Aetna, Rowe was named president, CEO, and chairman. Donaldson, having established Aetna’s new leader and having refocused Aetna entirely on health care and group benefits by selling Aetna Financial Services and Aetna International to AIG, could now step down from active management but remain on the board. By July 2001, less than one year after joining Aetna, Rowe’s top executive team was entirely new. “A lot of people in the company,” Rowe said in a 2001 BusinessWeek article, “need the kind of leadership that says, ‘Don’t tell me where you are from. Tell me where you are going.’”21 Two key new members Rowe recruited to the management team were Ronald Williams, named EVP and chief of health operations, and William Popik, MD, chief medical officer. Together, the team quickly assessed the situation as urgent and prioritized what needed to be done. In 2001, Rowe estimated that Aetna was losing about $1 million a day. Williams provided the strategic vision and detailed understanding of how to achieve operational excellence. As the former president of WellPoint Health Networks, he had played a key role in moving WellPoint from near-bankruptcy to being recognized as one of the best- managed companies in health care.22 A quiet, unassuming
- 41. leader, Williams set the tone by showing up for work at Aetna one day after he left WellPoint. “If I didn’t show urgency in what I did,” Williams asked, “why should anyone else?”23 The operational systems challenge for Williams was daunting. While Aetna’s competitors had expanded patient choices and had begun to provide more online access for patients and doctors, Aetna did not have the management information systems in place that could yield reliable data and enable those kinds of operations. Stillman said that a common complaint among physicians was Aetna’s slow pace in paying claims, something doctors attributed to the company’s playing the float, given its history as a financial services company. In addition, the rationale for why some claims were approved and others rejected was a “black box” mystery. While some believed these operational glitches represented willful misconduct, in reality Aetna 19 Jenny Holland, “My First Job: John W. Rowe: Different Rick, Different Hill,” New York Times (September 17, 2000). 20 Case writer interview with John W. Rowe, MD, July 5, 2006; unless otherwise noted, all subsequent Rowe quotations derive from this interview. 21 Moore. 22 Moore. 23 Sonia Alleyne, “Aetna: The Turnaround King,” Black
- 42. Enterprise, August 2, 2006. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -12- UV3935 had inadequate system tools in place that could sort through fundamental data, such as which codes it would pay and which codes it would not.24 William Popik, a well-regarded medical chief recruited from Cigna, faced the similarly daunting challenge of reorienting Aetna’s understanding of the inherently negative impacts the company’s policies and practices were having on their key stakeholder—physicians. Popik explained: Aetna was operating on a tightly controlled HMO model coupled with an institutional arrogance among those who had led that model on what health care should be for members and doctors. The company was also naïve about the power of physicians. The physicians were not blameless in this, some
- 43. thinking they could run the show based simply on “Trust me” with no accountability. But Aetna thought it could overcome the doctors and run their model through. Doctors normally could not agree on anything. But Aetna’s business practices were able to unite them in their desire to kill off the company and join with the lawyers. Popik summarized the situation they faced in 2001: “Aetna had become the poster child for everything wrong with managed care.” Another immediate priority was fixing Aetna’s unprofitable cost structure. Aetna had ended 2001 with a net loss of $279.6 million and growing concerns about being targeted for a hostile takeover. Painful but decisive steps were needed. Under Rowe’s leadership, Aetna adjusted premium costs to better reflect the actual health care costs the company faced. This change resulted in a membership loss of nearly eight million individuals, as well as product and market withdrawals in areas where it lacked the ability and market share to adequately negotiate profitable contracts with providers.25 Building the Aetna Way: 2001–06 From inherent risks to inherent strengths: transforming the business model
- 44. Rowe understood that what needed fixing at Aetna was more than tactical improvements of inefficient processes. The conclusion from a recently completed enterprise risk management assessment had indicated that Aetna’s greatest risk would be its failure to differentiate. “Without 24 Shaw; case writer interview with William Popik, January 4, 2006; unless otherwise noted, all subsequent Popik quotations derive from this interview. 25 Moore; Katzenbach Partners, “Anatomy of a Turnaround: The Difference Between Leading and Managing,” http://kathzenbach.com/Work/PublicationsInstance/tabid/73/Def ault.aspx?Entity_ID=383 (accessed July 2, 2009). This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -13- UV3935 differentiation,” Rowe explained, “insurance becomes a commodity with price being the only differentiator.”
- 45. Re-engineered operations enhanced through improved information processing would not differentiate Aetna if the underlying processes added no differentiating value. A more fundamental step to Aetna’s turnaround first required challenging long-held beliefs on what should be re-engineered. Otherwise the company could find itself efficiently implementing strategically flawed business processes. Rowe’s fresh perspective as a physician was critical at this stage, Shaw said: He was particularly good at knocking down the conventional wisdom. For example, the medical loss ratio or MLR had been a long held financial metric at Aetna. From Jack’s perspective, this was not a loss. It represented Aetna paying doctors for what they are supposed to do. It should be the medical cost ratio, not a loss ratio. Rowe quickly understood that some of Aetna’s underlying processes and business practices were counterproductive, such as the precertification requirement. “In some cases,” Rowe said, “that requirement made sense. But in other cases, like requiring precertification before performing a caesarian section, it was silly since the procedure would not have been denied anyway.” Aetna was the industry leader, and if it left
- 46. inherently flawed processes unchallenged, the damage would be replicated thousands of times, given the volume of Aetna’s claims. Rowe’s strategic vision for Aetna’s differentiated position was based on its ability as an insurer to prove the business case for quality care, not simply cost-effective care. The source for that differentiation rested with the smarter use of information to yield better medical outcomes. “The value-add of a health plan is more than negotiating and paying claims,” Rowe said. “The information we have about a member can improve the health of patients and can help doctors and patients decide on treatments and options.” In seeking to differentiate Aetna, Rowe was converting the inherent risks imposed by the current business practices in the managed care business model into inherent strengths in a transformed managed care business model. Rowe understood that physicians would be essential to accessing that information and defining insurance policies and practices that improved health care rather than seeming to interfere with it. If Aetna were going to change its practices, it needed to stop alienating doctors and start getting their input. There was, however, a significant roadblock. Following up on the groundwork Donaldson had done, Rowe began his outreach to physicians by setting up a
- 47. meeting with the Connecticut Medical Society. The meeting was soon canceled due to the physician class action that had been filed. So long as the class action were in place, meaningful dialogue with doctors and progress on Aetna’s strategic direction would be at a stalemate. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -14- UV3935 Removing the Roadblocks After the September 1999 Wall Street Journal article had broken the story about impending litigation, plaintiffs’ attorneys had sought to certify two class actions against managed care insurers Aetna, Humana, Cigna, Prudential, HealthNet, WellPoint, United Healthcare, and Coventry. One class would represent consumers (or subscribers) and the other would represent doctors (or providers). The suits alleged conspiracy under the Racketeer Influenced and Corrupt Organizations Act (RICO), which, if successful, would mean treble damages for the defendants.
- 48. Plaintiffs alleged that the HMO defendants had used cost containment as a screen to cheat doctors by manipulating claims and delaying payments. This included allegedly automated procedures to “down code” claims submitted by doctors to exclude those services from payment. Also at issue was the “all-products clause” requiring a doctor in an insurer’s network to accept all forms of plans offered by that insurer, no matter how unprofitable or administratively encumbered those plans might be for the physician. The intent was to prohibit doctors from cherry-picking. In 2000, doctors’ cases that had been filed across the country were consolidated in the Southern District of Florida before U.S. District Judge Federico A. Moreno in Miami and certified as a class action of more than 700,000 physicians. Moreno subsequently dismissed the consumer class action in 2002, ruling that there were too many differences among what different members were told about their coverage to justify class action treatment.26 Most observers had believed the patients/subscribers case had been the weaker of the two and expected the dismissal. Aetna’s focus, from the start, was on the doctors/providers class. As the industry leader in a financially weak position, the case posed a substantial threat. Given its huge volume of claims transactions, if Aetna lost on any of the key issues, its financial exposure
- 49. would be enormous. “This was bet-the-company litigation,” Shaw said. Given the high stakes, Shaw adopted a two-track litigation strategy. On track one, Aetna would play hardball, sending an unequivocal message that it would aggressively pursue its defense and vigorously engage at each step of the legal process, from discovery and depositions of class members to thoroughly arguing each key issue. According to Shaw, track two would focus on a potential settlement aimed at changing the business practices at issue. Rowe’s recruitment of Williams and Popik were key enablers for track two. Through Williams’s work on improving operations and Aetna’s information systems, the company was now in a position to understand the financial implications of potential changes. Through Rowe’s and Popik’s combined efforts to improve relationships with physicians, a dialogue could now begin. From the start, Aetna had ruled out any settlement compensation on a per-transaction basis for past practices. For the industry leader, an amount calculated on a per- transaction basis would be financially impossible. Instead, Aetna would focus settlement 26 Julie Kay, “HMO Suit Brings Big Payoffs to Lawyers but Leaves Unsettled Questions,” Daily Business Review, June 27, 2006.
- 50. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -15- UV3935 discussions on future business practices, consistent with its strategy for transforming its managed care business model, advancing Rowe’s strategic vision for Aetna while also addressing physicians’ underlying concerns in ways beyond what a monetary settlement alone could do. As settlement discussions began, reinvention at Aetna was already under way, and the industry as a whole had already begun moving away from the policies at issue in the litigation. But the cost-control-driven policies and practices of the HMO model had built a legacy of distrust among physicians, who entered the settlement discussion skeptical that the changes they had seen would be sustained. Shaw named Aetna Corporate Counsel Robert Stillman to lead the negotiations on track
- 51. two with a core group of doctors and state medical societies. As the discussions began in 2002, Aetna was in the uncertain, early stages of a turnaround, accentuating concern for the financial implications of any potential settlement, particularly if it meant that Aetna would be at a competitive disadvantage by assuming a higher cost structure. As Stillman guided the ensuing discussions, he kept the emphasis on future business practices that would improve the overall quality of care, a common ground for all sides of the negotiating table. “Some of the discussions confirmed changes we already had in place or were moving toward,” Stillman recalled. “For example, Aetna did not yet have online access for doctors to access fee schedules or CPT codes, but we were moving in that direction, and that capability would be needed, in any case, for the more open and transparent practices we envisioned.” Even with the focus on the future, the physicians’ frustrations with past practices were always present. “By 2001, the industry had already ceased requiring the contentious all-products clause,” Popik explained as an example of that frustration. “But during the settlement negotiations, physicians would insist that issue be included to ensure it would never reappear.” Once settlement discussions had advanced beyond theory, Aetna decided to advise the other defendant companies, which tried to talk the company out of its plan. At the time, Cigna had also been in urgent settlement discussions due to the aggressive trial schedule it was facing.
- 52. “Even though they were advanced in their discussions,” Shaw recalled, “the settlement they had constructed was fairly limited in terms of changing future business practices.” When Cigna announced its tentative settlement in 2002, medical societies in 19 states aggressively opposed it, calling it “woefully inadequate.”27 A few days later, Moreno, under whom the cases had been consolidated in 2000, halted Cigna’s proposed settlement after preliminary approval had been granted in a state court. No further action on the Cigna settlement could occur without Moreno’s permission.28 From Controlling to Enabling 27 “200,000 Physicians: Cigna Settlement Bad for Doctors and Their Patients,” http://www.allbusiness.com/ legal/trial-procedure-suits-claims/6012559-1.html, December 10, 2002 (accessed November 2, 2009). 28 “U.S. Judge Halts Cigna Settlement,” New York Times, December 13, 2002. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -16- UV3935
- 53. The biggest battle in negotiating the settlement centered on the amount of money Aetna would pay the more than 700,000 doctors in the class. Any meaningful per-doctor payment had the potential to bankrupt the still financially fragile Aetna. The common-ground breakthrough came through the creation of a medical foundation. Initially conceived of by Stillman and strongly supported by Bolton and Carter, the new foundation would be funded by Aetna and would focus on enhancing physicians’ ability to provide their patients with quality health care. Critical areas would include initiatives to reduce or prevent childhood obesity, for example, and to improve end-of-life care. Physicians, who would receive minimal per-physician compensation through the settlement, could choose to contribute their compensation to the foundation, expanding on Aetna’s grant. The addition of the foundation to the settlement provided Aetna with a constructive action platform that positioned the company as taking positive, forward- looking action and differentiated the company from its competitors. In addition to the foundation, negotiations focused on revising the contested managed care practices. “The overall settlement involved a mixture of new things not already done, some things that had already been changed, some things Aetna knew
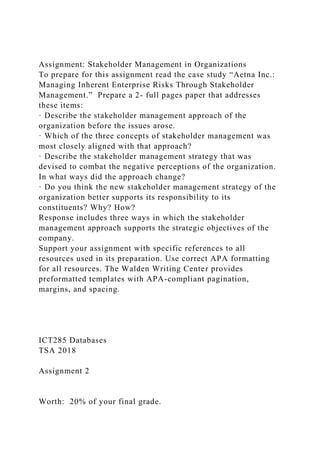
- 54. it had to do, and some things that Aetna did not want to do, but had to do anyway,” Popik recalled. Managed care had focused on controlling costs through the insurers’ administrators, who authorized treatments based on proven procedures. Through the settlement, in language approved by the American Medical Association, Aetna changed its coverage language to explicitly give more weight to treating physicians’ clinical judgment as a factor in approved treatments and applying generally accepted medical standards in determining medical necessity. In addition, the settlement would establish a national advisory committee of practicing physicians to provide Aetna with ongoing counsel on issues of concern. The committee would institutionalize a cooperative process between Aetna and physicians as they worked together to improve health care through revised managed care practices. Finally, Aetna would implement information systems and policies that would dramatically increase its openness and transparency with physicians, enabling them to understand their options in advance of treatment, reduce administrative overhead, and speed payments.29 The much disliked “black box” of insurance claims processing would now be in the sunlight. In all, the settlement totaled $170 million, resulting in an after- tax charge net of insurance
- 55. coverage of $75 million (Table 1). Aetna estimated the value to physicians for these changes in its business practices would be $300 million, resulting from outcomes such as more prompt payments and lower administrative costs. 29 “Physicians and Aetna Begin New Era of Cooperation,” Aetna press release, May 22, 2003. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -17- UV3935 Foundation $20 million Legal fees $50 million Payment to Physicians $100 million Total $170 million Data source: Aetna Inc. Anticipating the reaction to Aetna’s settlement terms, Rowe understood that some people would think spending $170 million to settle the case was crazy. “As a CEO, I was making a strategic decision. Lawyers offer a legal view, but a legal victory doesn’t
- 56. necessarily equate to a business victory,” he said. Table 1. Settlement summary. The Announcement Dilemma Once the settlement was finalized in spring 2003, Aetna needed to announce it promptly, given its obvious material impact on the company. How to announce the settlement was not obvious. The context Based on the pattern of previous major litigation settlements from high-visibility cases, Aetna could anticipate headlines such as “Plaintiffs Bring Aetna to its Knees” as journalists and commentators inevitably began their scoreboarding of who won and who lost. The plaintiffs’ high-profile celebrity attorneys and their obvious enjoyment of being in the spotlight seemed to guarantee a major story with the typical David-and-Goliath casting. By 2003, Aetna was barely turning a profit. Observers could conclude that Aetna’s
- 57. decision to settle was a sign of desperation, guilt, or a weak defense. Whatever the perceived cause for settling, some would see this as Aetna’s taking on a larger cost structure than its competitors because of the settlement terms. That perception could trigger a bad Wall Street reaction and potentially concern some of Aetna’s corporate benefits customers, who might question whether Aetna would be less able to manage the cost of their health care plans. Employees were another key stakeholder to consider. Having previously witnessed firsthand Aetna’s fallen market position, many Aetna employees had been encouraged once the company had begun to turn the corner. Aetna was a proud company with a long tradition, and its culture would have a hard time accepting that it had done something wrong and needed to be punished. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -18- UV3935 Finally, Aetna’s line business management was eager to put the
- 58. litigation behind the company as quietly and as quickly as possible. All its competitors were still committed to battling the issues through litigation. Aetna was by itself in its decision to settle. Range of strategies All these concerns could support a low-key announcement strategy with talking points ready to refute the anticipated negative reactions. In this scenario, the announcement would likely occur at the end of the day on a Friday or just before a holiday, making it a one-day news story without much visibility. On the other hand, a negative reaction to the settlement was not guaranteed. By 2003, many on Wall Street and in the business world in general had seen the risks companies faced if they chose to fight all battles with a well-funded and media- savvy plaintiffs’ bar. Aetna’s forward motion in its turnaround and new strategic course could be compromised by the arduous and distracting process of effectively managing mass litigation. In addition, continuing the legal battle would mean ongoing litigation expenses estimated to be about $20 million per year. Regardless of which communications approach Aetna selected at announcement time, Bolton and Carter knew the company had one shot at getting it
- 59. right. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -19- UV3935 Exhibit 1 AETNA INC.: MANAGING INHERENT ENTERPRISE RISKS THROUGH STAKEHOULDER MANAGEMENT (A) April 2, 1996, Press Release Aetna Completes Previously Announced Sale of Property/Casualty Operations to Travelers HARTFORD, CT, April 2, 1996—Aetna (NYSE: ΑET) said today that it has completed the previously announced sale of its Property/Casualty operations to the Travelers Insurance Group Inc. for total consideration of $4.1 billion. “The closing of the sale of our Property/Casualty business completes a major phase in Aetna’s transformation from a traditional multiline insurer to a growth company focused on leading edge health care and retirement services, in both the U.S. and
- 60. selected international markets,” Aetna Chairman Ronald E. Compton said. As part of the P/C sale agreement, Travelers has assumed eight years of Aetna’s lease at CityPlace in downtown Hartford. Aetna has previously announced that it will take a $190 million after-tax charge for its remaining CityPlace lease obligation in conjunction with the close of the transaction. For more information about Aetna Inc., please visit the company’s website at www.aetna.com. Source: Aetna Inc. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019. -20- UV3935 Exhibit 2 AETNA INC.: MANAGING INHERENT ENTERPRISE RISKS THROUGH STAKEHOULDER MANAGEMENT (A) July 19, 1996, Press Release
- 61. Aetna and U.S. Healthcare Complete Merger Merger creates nation’s leading health care benefits company HARTFORD, CT, July 19, 1996—Aetna (NYSE: ΑET) and U.S. Healthcare (NASDAQ: USHC) today announced that they have completed their merger, creating the nation’s leading health care benefits company. Aetna Chairman Ronald E. Compton said, “This merger transforms Aetna into a growth company with the scale and expertise necessary to thrive in the dynamic health care industry, and positions us to deliver superior long-term value to shareholders. The health care industry, and managed care in particular, continues to be a business with excellent current and future prospects. “Our unique ability to provide access to affordable, high-quality health care on a national level will be the key to our future success, allowing us to create the first truly national managed care company,” Compton said. As part of the merger, Aetna Life and Casualty Co. has been renamed Aetna Services, Inc. and a new holding company, Aetna Inc., has been formed as the parent company to Aetna Services and U.S. Healthcare, Inc. Aetna Inc. will begin trading on the New York Stock Exchange under the symbol “AET” commencing on Monday, July 22, 1996.
- 62. U.S. Healthcare shareholders will receive $34.20 in cash, 0.2246 shares of Aetna Inc. common stock, and 0.0749 shares of Aetna Inc. 6.25% Class C Voting Preferred Stock for each share of U.S. Healthcare stock. Each share of Aetna Life and Casualty Company stock will become one share of new Aetna Inc. stock. The combined Aetna/U.S. Healthcare health business will provide health care benefits, specialty health, group life and disability insurance to more than 23 million Americans. For more information about Aetna Inc., please visit the company’s website at www.aetna.com. Source: Aetna Inc. This document is authorized for use only in ANGELA MONTGOMERY's Stakeholder Management and Organizational Behavior - MSPM 6160 at Laureate Education - Baltimore from Feb 2018 to Apr 2019.