Rhabdomyolysis
•
17 likes•9,510 views

Rhabdomyolysis is a condition where skeletal muscles are damaged and release myoglobin into the bloodstream, which can damage the kidneys. It causes muscle pain, weakness, swelling, and dark or red urine. In severe cases it can lead to kidney damage or failure. It is caused by conditions that damage muscles severely like injuries, overexertion, alcohol or drug abuse, lack of blood flow, or surgery. Diagnosis involves clinical suspicion and lab tests showing abnormal electrolytes, enzymes and myoglobin in the blood and urine. Treatment focuses on fluid resuscitation and electrolyte replacement in early stages and may require dialysis in severe cases.
![overview ,[object Object],[object Object],[object Object],[object Object],[object Object],[object Object]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Rhabdomyolysis
Similar to Rhabdomyolysis (20)
More from Jamie Ranse
More from Jamie Ranse (20)
Recently uploaded
Recently uploaded (20)
Rhabdomyolysis
- 1. Jamie Ranse : Critical Care Education Coordinator, Staff Development Unit, ACT Health. RHABDOMYOLYSIS
- 9. causes: hours of ischemia 0 2 4 6 Tolerable-no permanent histological changes Irreversible anatomic and functional changes Muscle necrosis
- 10. causes: cellular ion physiology
Editor's Notes
- Diagnosis The doctor will ask about your symptoms and medical history, and perform a physical exam. Tests may include: Urine tests Blood tests Muscle testing ( electromyography ) Treatment Treatment may include: Hydration Giving large amounts of fluid is the main treatment. Fluids are usually given directly into a vein by an IV. Hydration helps to quickly flush myoglobin out of the kidneys, in order to restore their function. Medication Medication may include: Diuretics—to help flush out the kidneys Bicarbonate—to minimize myoglobin's toxic effects Dialysis Dialysis is a procedure that uses an artificial kidney machine to filter blood. The clean blood is then returned to your body. Prevention Steps for prevention include: Drink plenty of fluids when: Exercising Sitting or working in hot, humid weather Avoid overuse of alcohol. Avoid illicit drugs.
- muscle injury Crush injuries , long surgeries in lithotomy or lateral decub, surgery on morbidly obese patients (gluteal), contact sports, burns, lifting heavy weights ( Occurs in up to 85% of patients with traumatic injuries. Those with severe injury who develop rhabdomyolysis-induced renal failure have a 20% mortality rate) Exercise: talk about NYPD Alcohol / drugs: alcohol abuse and subsequent immobility and coma, direct myotoxic effects of alcohol Vascular compromise: compartment syndrome, embolus and subsequent reperfusion Sugical procedures: Rarely may be caused by extensive surgical procedures using large muscle dividing incisions (in ICU paralytic agents such as vecuronium, due to prolonged stasis_
- muscle injury Crush injuries , long surgeries in lithotomy or lateral decub, surgery on morbidly obese patients (gluteal), contact sports, burns, lifting heavy weights ( Occurs in up to 85% of patients with traumatic injuries. Those with severe injury who develop rhabdomyolysis-induced renal failure have a 20% mortality rate) Exercise: talk about NYPD Alcohol / drugs: alcohol abuse and subsequent immobility and coma, direct myotoxic effects of alcohol Vascular compromise: compartment syndrome, embolus and subsequent reperfusion Sugical procedures: Rarely may be caused by extensive surgical procedures using large muscle dividing incisions (in ICU paralytic agents such as vecuronium, due to prolonged stasis_
- Age range 33 – 43 years old, average age of 36 years 8 male, 2 female 5 smokers 8 prostitution/anti-crime cops from 6 th precinct (all male) All walk-in, 2 on 3/15, 1 on 3/16 and remaining 7 on 3/18-3/19 5 hospitalized < 1 day 5 hospitalized 4-10 days Of those hospitalized > 1 day: 2 had underlying conditions unrelated to the training which required follow-up and hospital care All received IV fluids, responded well to treatment, decreased CK levels over time Independent investigators discovered a referral from the commanding officer, following participants complained of sore muscles.
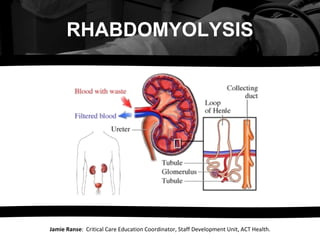
- Damage to skeletal muscle may take various forms. Crush injuries damage muscle cells directly, as well as impairing the blood supply; other causes may damage muscle cells by interfering with their metabolism . The muscle tissue rapidly fills with fluid from the bloodstream, as well as sodium and chloride . The swelling itself may lead to destruction of muscle cells, but those cells that survive react by pumping sodium out of the cells in exchange for calcium (through the sodium-calcium exchanger ). The accumulation of calcium in the sarcoplasmic reticulum leads to continuous muscle contraction and depletion of ATP , the main carrier of energy in the cell. Calcium also stimulates the enzyme phospholipase A2 , which damages the mitochondrion , causing the production of reactive oxygen species . [22] In addition, neutrophil granulocytes (the most abundant white blood cells ) enter the muscle tissue, producing an inflammatory reaction and releasing even more reactive oxygen species. [2] The swollen and inflamed muscle may directly compress structures in the same fascial compartment, causing compartment syndrome. The swelling may also further compromise blood supply into the area. Finally, destroyed muscle cells release potassium, phosphate , myoglobin (a heme and therefore iron -containing protein), creatine kinase (an enzyme) and uric acid (a breakdown product of purines from DNA ) into the blood. Activation of the coagulation system may precipitate diffuse intravascular coagulation. [2] High potassium levels ( hyperkalemia ) may lead to potentially fatal disruptions in heart rhythm. Phosphate precipitates with calcium from the circulation, leading to hypocalcemia (low calcium levels). [2] Various consequences of muscle swelling and breakdown together may cause renal failure. The swelling of large areas of muscle tissue leads to depletion of fluid from the circulation, causing relative lack of blood flow to the kidney. Uric acid may precipitate in the tubules , causing obstruction. Finally, the most important problem is the accumulation of myoglobin in the tubules. [2] Myoglobinuria (the appearance of myoglobin in the urine) occurs when the levels in plasma exceed 1.5 mg/dl. [1] As the kidneys reabsorb more water from the filtrate, myoglobin forms casts that obstruct the normal flow of fluid through the nephron ; the condition is worsened by high levels of uric acid and acidification of the filtrate. Iron released from the myoglobin generates reactive oxygen species, damaging the kidney cells. Acute tubular necrosis (destruction of the cells of tubules) occurs, preventing the kidney from performing its normal excretory functions (hence the fall in glomerular filtration rate ), electrolyte regulation (hence worsening potassium levels) and hormone production (hence decreased vitamin D processing, further worsening the low calcium levels). [2]
- Clinical suspicion: The diagnosis may be suspected in anyone who has suffered a trauma, crush injury or prolonged immobilization, Compartment Syndrome is a clinical diagnosis (i.e. no tests conclusively prove its presence or absence), but direct measurement of the pressure in a fascial compartment may be used to assess its severity. Values of 30–50 mmHg (4–6.5 kPa ) indicate severe compartment syndrome and possible need for fasciotomy , which is an incision to relieve increased pressure Abnormal electrolytes: CK: at a later stage due to deteriorating kidney function (abnormally raised or increasing creatinine and urea levels, falling urine output). The most reliable test in the diagnosis of rhabdomyolysis is the level of creatine kinase (CK) in the blood. This enzyme is released by damaged muscle, and levels above 5 times the upper limit of normal (ULN) indicate rhabdomyolysis. Depending on the extent of the rhabdomyolysis, levels up to 100,000 units are not unusual. [2] Initial and peak CK levels have a linear relationship with the risk of acute renal failure: the higher the CK, the more likely it is that kidney damage will occur. [21] CK levels rise after 12 hours of the initial damage, remain elevated for 1–3 days and then fall gradually. K: High potassium levels (hyperkalemia) tend to be a feature. Calcium: Low calcium levels may be present in the initial stage, Cardiac troponin : levels (normally used to diagnose heart damage) are increased in half of all cases, but not associated with other evidence of heart damage in at least a third of those cases. [20] LFTs: about a quarter of patients have abnormal liver function tests due to liver damage. Myoglobin: has a short half-life, and is therefore less useful as a diagnostic test in the later stages. [1] Urine: Decreased Uo typical pink-red discoloration of the urine. Blood - Dipstick analysis of urine may reveal a positive result for &quot;blood&quot; in the absence of red blood cells on microscopy,
- Fluid therapy The main goal of treatment is to treat shock and preserve kidney function. Initially this is done through the administration of generous amounts of intravenous fluids, usually saline (0.9% weight per volume sodium chloride solution). In victims of crush syndrome (e.g. in earthquakes), it is recommended to start this even before the casualties are extracted from collapsed structures. This will ensure sufficient circulating volume to deal with the muscle cell swelling (which typically commences when blood supply is restored), and to prevent the deposition of myoglobin in the kidneys. Amounts of 6 to 12 liters over 24 hours are recommended. [2] While many sources recommend mannitol, which acts by osmosis to ensure urine production and may prevent heme deposition in the kidney, there are no studies directly demonstrating its benefit. Similarly, the addition of bicarbonate to the fluids is intended to improve acidosis (high acid level of the blood) and thereby prevent cast formation in the kidneys, but there is limited evidence that it has benefits above saline alone. Furosemide, a loop diuretic, is often used to ensure sufficient urine production. [1][2] Electrolytes In the initial stages, electrolyte levels are often abnormal and require correction. Calcium levels initially tend to be low, but as the patient's condition improves calcium is released from where it has precipitated with phosphate, and vitamin D production resumes, leading to hypercalcemia (abnormally high calcium levels). This &quot;overshoot&quot; occurs in 20–30% of those people who have developed kidney failure. [1] Dialysis If kidney dysfunction (acute renal failure, ARF) develops (usually 1–2 days after the initial muscle trauma), renal replacement therapy (RRT) may be required. This may take the form of hemodialysis or hemofiltration. Certain types of peritoneal dialysis are also effective in removing the high levels of toxic solutes that can accumulate in rhabdomyolytic renal failure, and may be the only available option in some Third World settings. [23] RRT removes excess potassium, acid and phosphate that accumulates when the kidneys are unable to function normally and is required until kidney function is regained. [1] EARLY Begin early, even on the field Damaged muscles attract a lot of fluid Up to 10L/day Ideally ½ NS with 100mmol/L bicarb prevents tubular precipitation reduces risk of hyperkalemia from damaged mm corrects acidemia not proven beneficial however not deleterious 10ml/h 15% mannitol renal vasodilator free radical scavenger Forced diuresis w/in 6 hrs of admission LATE Dialysis – intermitted preferred to continuous Reduce use of anticoagulants in trauma patients