Alexander1
Students are required to submit one written assignment during the course of the semester. The
required content of the assignment is set forth below. The written essays must be submitted
electronically by the student into the course Safe Assign system. Only Word format is accepted by the
system. THE WRITTEN ASSIGNMENT IS DUE NO LATER THAN THE DATE AND TIME SET FORTH ON
THE COURSE SCHEDULE. ABOLUTELY NO LATE PAPERS WILL BE ACCEPTED.
IMPORTANT NOTE: Students are NOT allowed to submit papers they have written for any
other course including written assignments and papers submitted in POLS 2301. If a student is retaking
POLS 2302 for a grade replacement, the student is NOT allowed to submit a paper previously submitted
in any POLS 2302 course or any other course. Submission of a paper previously submitted by you or any
other student in any other course will appear in SafeAssign and be considered by the instructor to be
plagiarized. A paper submitted in this course – written by the student or any other person - that appears
in any other course will result in an assignment score of zero. Your name and work will be submitted into
a permanent file marked “plagiarism” and may be used by the instructor or subsequent instructors for
evidence of one-time or repeated plagiarism and may be used as evidence of academic dishonesty
resulting in expulsion from Lamar University.
• Your essay must include a title page containing your name, POLS 2302, Written Assignment (with
an essay title), semester, and the date of your submission of the assignment through Safe
Assign. (The title page is not included as a numbered page and your essay should meet the page
number requirement exclusive of the cover page.)
• The written assignment MUST be uploaded as ONE document (title page, essay, works cited
should all be in the SAME document). Students may NOT submit the assignment via email inside
or outside the course Blackboard system. Students may not cut and paste essays into the
assignment window - the assignment MUST be uploaded as a WORD document and MUST be in
ONE file. Do NOT upload more than one written assignment document. The system will only allow
[Last Name] 2
you to select ONE file, so make sure that file is the combined cover page, paper, AND
bibliography. Assignments uploaded in any format other than WORD, such as a PDF, RTF, ZIP,
etc., will automatically receive an overall assignment score of zero. Assignments submitted only
via email will automatically receive a zero as will assignments submitted outside of Safe Assign.
In summary, you MUST submit your paper:
1. As one complete paper (no separate submissions of title pages or bibliographies);
2. In Word format (no zip drives, PDF, RTF or other forms of submission);
3. As an uploaded document from your computer; with the box checked for your
agreement to submit your paper to the Global.
Alexander1 Students are required to submit one written.docx
1. Alexander1
Students are required to submit one written assignment during
the course of the semester. The
required content of the assignment is set forth below. The
written essays must be submitted
electronically by the student into the course Safe Assign
system. Only Word format is accepted by the
system. THE WRITTEN ASSIGNMENT IS DUE NO LATER
THAN THE DATE AND TIME SET FORTH ON
THE COURSE SCHEDULE. ABOLUTELY NO LATE PAPERS
WILL BE ACCEPTED.
IMPORTANT NOTE: Students are NOT allowed to submit
papers they have written for any
other course including written assignments and papers
submitted in POLS 2301. If a student is retaking
POLS 2302 for a grade replacement, the student is NOT allowed
to submit a paper previously submitted
in any POLS 2302 course or any other course. Submission of a
paper previously submitted by you or any
2. other student in any other course will appear in SafeAssign and
be considered by the instructor to be
plagiarized. A paper submitted in this course – written by the
student or any other person - that appears
in any other course will result in an assignment score of zero.
Your name and work will be submitted into
a permanent file marked “plagiarism” and may be used by the
instructor or subsequent instructors for
evidence of one-time or repeated plagiarism and may be used as
evidence of academic dishonesty
resulting in expulsion from Lamar University.
• Your essay must include a title page containing your name,
POLS 2302, Written Assignment (with
an essay title), semester, and the date of your submission of the
assignment through Safe
Assign. (The title page is not included as a numbered page and
your essay should meet the page
number requirement exclusive of the cover page.)
• The written assignment MUST be uploaded as ONE document
(title page, essay, works cited
should all be in the SAME document). Students may NOT
submit the assignment via email inside
3. or outside the course Blackboard system. Students may not cut
and paste essays into the
assignment window - the assignment MUST be uploaded as a
WORD document and MUST be in
ONE file. Do NOT upload more than one written assignment
document. The system will only allow
[Last Name] 2
you to select ONE file, so make sure that file is the combined
cover page, paper, AND
bibliography. Assignments uploaded in any format other than
WORD, such as a PDF, RTF, ZIP,
etc., will automatically receive an overall assignment score of
zero. Assignments submitted only
via email will automatically receive a zero as will assignments
submitted outside of Safe Assign.
In summary, you MUST submit your paper:
1. As one complete paper (no separate submissions of title
pages or bibliographies);
2. In Word format (no zip drives, PDF, RTF or other forms of
submission);
4. 3. As an uploaded document from your computer; with the box
checked for your
agreement to submit your paper to the Global
Reference Database;
4. No later than November 4, 2022, at 11:59 p.m.
You should note that the assignment folder closes precisely at
11:59 p.m. Submissions
submitted at 11:59.1 will be rejected by the system, registered
as a late submission, and result in an
assignment score of zero.
The written assignment will be used to access the Critical
Thinking and Communication Skills
Learning Outcome core curriculum requirements of the Texas
Higher Education Coordinating Board
(THECB). A copy of the assessment rubric designed to satisfy
THECB requirements will be provided in
class.
Write a three-to-five page essay containing the
following:
5. An introductory paragraph containing a brief description of
three subject areas studied this
5. semester that you found most interesting and/or informative,
and a statement about a
contemporary political problem or issue related to the course
that will be discussed in greater
detail later in the paper. The three subject areas you discuss
MUST be from POLS 2302 and
[Last Name] 3
cannot be topics studied in POLS 2301 (i.e., parties, the media,
interest groups, elections).
Subject areas should focus on topics listed in the syllabus. In
POLS 2302, one of your topic areas
should be one of the three branches of government.
6. Identify, discuss and describe a specific contemporary
political problem in one of the three
subject areas you identified.
7. Construct and communicate a solution to the problem you
identified (above). Make sure to
develop and express your solution in the form of an argument
that is supported by well-
6. documented and properly cited facts and data. A good paper
will have at least 3-5 scholarly
sources in addition to the course textbook(s) and course videos.
Correct grammar, capitalization, punctuation, complete
sentences, and CITATION of your
sources is required. Textbook readings with page numbers (or
chapter headings and subheadings for
digital textbooks without page numbers) and textbook citation;
lectures or video instruction (title and
presenter/author of the video); and outside scholarly research
must be included in your assignment.
Wikipedia/Encyclopedia/Dictionary/Spark Notes and other
similar sources are NOT allowed
and will result in an assignment score of zero. Failure to
submit the assignment by the deadline will
result in a grade of zero for the overall written assignment
grade. Citations must be provided in both the
body of your essay and in a “Works Cited” section at the
conclusion of your essay. Also note that
references to court cases must be italicized (Brown v. Board of
Education) or underlined (Brown v. Board
of Education). If you are using internet citations, you MUST
7. include the FULL URL, title, author (if
available) and access date.
Your written assignment should be typed and double spaced
with 12-point font and one-inch
margins top, bottom, and side. Political Science as a field has
adopted the APSA Manual of Style;
[Last Name] 4
however, you are free to use the citation style adopted by your
major department or the style used in your
English composition courses (MLA or other style). Regardless
of citation style, all sources must be
properly, thoroughly, and consistently cited. Careful attention
to grammar, spelling, and the mechanics of
presentation is expected. Wikipedia is not a reliable source of
information. Any citation of Wikipedia,
Dictionary.com (or any Dictionary related website), E-
Encyclopedia (or any Encyclopedia website), Spark
Notes, Cliff Notes, Reference.com, Shmoop.com,
Socialstudieshelp.com, Study.com, Vocabulary.com,
Ask.com , Softschools.com, Scholastic.com, biography.com,
8. study.com, quotationspage.com,
legallanguage.com, totallyhistory.com, history.com,
UShistoryscene.com, The Bible, Major Motion
Pictures, or anything similar in a term paper or other
assignment in this course will result in an automatic
score of 0 (zero) on the assignment. Scholarly resources would
include journal articles, books, and news
organization websites.
Carefully read the Course Management Policies, “Academic
Honesty Statement” for additional
guidelines for your written assignments. Any cut and paste,
plagiarized, or Wiki cited posts or papers will
result in an automatic grade of zero for the overall assignment
and possible expulsion from the course
and Lamar University. NO late papers will be accepted, this
includes papers posted a minute or more
late. Students have ONLY one chance to upload papers to Safe
Assign and the version that is uploaded is
the version that will be graded.
9. Biological
Psychiatry
GOS
210
Biolog
:
Archival Report
Secondary Sources of Negative Symptoms in
Those Meeting Criteria for a Clinical High-Risk
Syndrome
Tina Gupta, Gregory P. Strauss, Henry R. Cowan, Andrea
Pelletier-Baldelli, Lauren M. Ellman,
Jason Schiffman, and Vijay A. Mittal
ABSTRACT
BACKGROUND: Negative symptoms are diagnostic
characteristics of schizophrenia. They can result from primary
(i.e., idiopathic) or secondary (i.e., due to other factors such as
depression, anxiety, psychosis, disorganization,
medication effects) features of the illness. Although secondary
sources of negative symptoms are prevalent among
individuals meeting criteria for clinical high-risk syndromes
that are due to high rates of comorbidity, the extent to
which secondary sources account for variance in negative
symptom domains is unknown. Addressing this gap is an
important step in informing vulnerability models and treatments
for negative symptoms. This study aimed to inves-
tigate secondary sources of negative symptoms in those meeting
criteria for a clinical high-risk syndrome (N = 192).
METHODS: Simultaneous regression and hierarchical
10. partitioning methods were used to determine the proportion of
variance explained by selective serotonin reuptake inhibitor use,
anxiety, depression, unusual thought content, and
disorganized communication in predicting severity of five
negative symptom domains (avolition, anhedonia, aso-
ciality, blunted affect, and alogia).
RESULTS: Findings revealed that depression explained the
largest proportion of variance in avolition, asociality, and
anhedonia. Anxiety was the most predictive of blunted affect,
and selective serotonin reuptake inhibitor use explained
the most variance in alogia. Analyses within male and female
samples revealed that in males, depression explained a
large proportion of variance in several negative symptom
domains, while in females, selective serotonin reuptake
inhibitor use explained variance in alogia.
CONCLUSIONS: Results highlight heterogeneity in variance
explained by secondary sources of negative symptoms.
These findings guide treatment development for secondary
sources of negative symptoms. Furthermore, results
inform etiologic models of psychosis and negative symptom
conceptualizations.
https://doi.org/10.1016/j.bpsgos.2021.05.008
Negative symptoms have long been considered a core
component of psychopathology in individuals with schizo-
phrenia (1,2). Early factor analytic studies in schizophrenia
have supported a two-factor negative symptom structure
consisting of diminished expression and motivation and plea-
sure (3–5). However, more recent confirmatory factor analytic
and network analysis studies that directly tested the latent
structure of the construct suggest that the two-factor model
offers a poor fit; rather, a five-factor model, corresponding to
the five domains identified in the National Institute of Mental
Health consensus conference on negative symptoms (6),
provides an excellent fit. These findings have been replicated
across contemporary negative symptom scales (Brief Negative
11. Symptom Scale, Clinical Assessment Interview for Negative
Symptoms, Scale for the Assessment of Negative Symptoms),
across multiple cultures, using multiple mathematical tech-
niques (confirmatory factor analysis, network analysis), and
across chronic, first episode, and clinical high-risk (CHR)
phases of illness (7–13). In addition, negative symptoms can
ª 2021 THE AUTHORS. Published by Elsevier Inc on behalf of
the S
CC BY-NC-ND license
(http://creativecommons.org/licenses/by-nc-
ical Psychiatry: Global Open Science September 2021; 1:210–
218 w
result from primary (i.e., idiopathic) or secondary (i.e., due to
depression, anxiety, hallucinations, delusions, disorganization,
medication effects) sources of influences (14–16), and this
notion can complicate conceptualization and treatment.
Essentially, two individuals can have the exact same score on
a negative symptom rating scale but for very different reasons
(i.e., equifinality). Importantly, when secondary sources of
negative symptoms are identified and appropriately targeted,
they are typically effectively treated (16), whereas primary
negative symptoms remain largely resistant to current phar-
macological and psychosocial interventions (17).
Historically, primary and secondary negative symptoms
have been distinguished clinically using the Schedule for the
Deficit Syndrome, which requires clinicians to judge whether
negative symptoms are of clinically significant severity and
whether they likely result from secondary sources (e.g.,
anxiety, depression, positive symptoms, extrapyramidal
symptoms); in the absence of clear secondary sources
deemed to drive negative symptoms, they are rated as
ociety of Biological Psychiatry. This is an open access article
under the
nd/4.0/).
12. ww.sobp.org/GOS ISSN: 2667-1743
Delta:1_given name
Delta:1_surname
Delta:1_given name
Delta:1_surname
Delta:1_given name
Delta:1_surname
https://doi.org/10.1016/j.bpsgos.2021.05.008
http://creativecommons.org/licenses/by-nc-nd/4.0/
http://www.sobp.org/GOS
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
primary. Cases where negative symptoms are considered of
sufficient severity, to be driven by primary (rather than sec-
ondary) factors, and to be persistent (rather than transient) are
deemed to meet criteria for the deficit syndrome (a putative
schizophrenia subgroup with distinct etiologic factors). Of
note, secondary effects of positive symptoms on negative
symptoms have been identified in the literature (14,16). For
example, an individual may experience persecutory thoughts
and withdraw from social interactions (16). Other work has
found influences of extrapyramidal side effects on blunted
affect (18) and relationships between negative symptoms and
depression and anxiety (19,20). In addition, disorganization is
associated with blunted affect (e.g., facial and vocal flattening
due to limited available cognitive resources) (21) as well as
motivational impairments (22).
Individuals meeting criteria for a CHR syndrome also display
clinically significant negative symptoms (23–27). These im-
pairments have been found to emerge before attenuated
13. positive symptoms, are linked to poor functional outcome, and
are predictive of transition to a psychotic disorder (26,28,29).
However, the extent to which negative symptoms are driven by
secondary sources in this group is unclear. Currently, there are
measures such as the Negative Symptom Inventory-Psychosis
Risk (NSI-PR) (25,27) that are geared toward isolating primary
negative symptoms. However, distinct categorizations (i.e.,
nondeficit and deficit syndrome) observed in schizophrenia are
not yet possible to implement in CHR groups. Investigating the
potential influences of secondary sources (i.e., the variance
explained) can provide foundation for this future work. One
might expect secondary sources to account for some of the
proportion of variance in negative symptom scores, given
elevated rates of comorbid mood and anxiety disorders, high
rates of psychotropic medications prescription, and the pres-
ence of attenuated positive and disorganized symptoms
(30,31). Similar to schizophrenia (13), negative symptoms
exhibit a five-factor structure in those meeting criteria for a
CHR syndrome (7), and it will be critical to determine the
extent
to which these individual domains are predicted by various
secondary sources. Determining the proportion of variance
explained by common secondary factors can inform early
intervention and prevention efforts, given that negative symp-
toms are known to remit in some individuals with schizo-
phrenia when the appropriate secondary source is effectively
targeted (16).
The aim of this study was to investigate sources of sec-
ondary negative symptoms in a sample of individuals meeting
criteria for a CHR syndrome. Specifically, we assessed the
proportion of variance in five negative symptom domains
(avolition, asociality, anhedonia, blunted affect, alogia), in line
with current findings suggesting that a five-factor structure of
negative symptoms is optimal in CHR groups (7), accounted
for by anxiety, depression, unusual thought content, disorga-
14. nization, and psychotropic medication prescription. To achieve
these aims, regression analyses and hierarchical partitioning
were used. Given the research suggesting relationships be-
tween mood symptoms and both anhedonia and asociality in
schizophrenia (19,20) (e.g., bidirectional relationships between
feeling depressed and anxious and reduced enjoyment in ac-
tivities or wanting to interact with others), we predicted that
mood symptoms (i.e., anxiety, depression) would explain the
Biological Psychiatry: Global Ope
largest variance in anhedonia and asociality. Furthermore,
given the evidence of the role of extrapyramidal side effects on
blunted affect in schizophrenia (18), medication use would
explain most of the variance in blunted affect and alogia.
Finally, given the findings of relationships between disorgani-
zation and both blunted affect and avolition in schizophrenia
(21,22), we predicted that disorganization would explain a large
portion of the variance in blunted affect and avolition. It is also
possible that anxiety and unusual thought content would
explain some variance across all negative symptom domains
because these facets of psychopathology have evidenced
relationships with negative symptoms broadly defined.
METHODS AND MATERIALS
Participants
In this cross-sectional design, participants were 192 in-
dividuals meeting criteria for a CHR syndrome, aged 13–30
(mean = 19.90, SD = 2.21) years. The sample included par-
ticipants recruited to the Adolescent Development and Pre-
ventive Treatment Program at University of Colorado Boulder
and Northwestern University (principal investigator: VAM) and
the Multisite Assessment of Psychosis-Risk study (32).
Participant data were collected during baseline assessments
across sites. The Structured Interview for Psychosis Risk
Syndromes (SIPS) (33) was administered to assess the pres-
15. ence of psychosis-risk symptoms. The SIPS is designed to
detect a CHR syndrome by assessing positive symptom do-
mains (e.g., unusual thought content/delusion ideas, suspi-
ciousness/persecutory ideas). Participants received a CHR
status by receiving a score ranging from 3 (moderate) to 5
(severe but not psychotic) on any SIPS positive symptom
domain, a standardized approach in the field (33). Furthermore,
participants were considered as meeting the criteria for a CHR
syndrome if they met the criteria for schizotypal personality
disorder or had a family member with a schizophrenia spec-
trum and other psychotic disorder diagnosis, with a decline in
functioning (7% of the sample). The Structured Clinical Inter-
view for the DSM (34) was used to assess for comorbid
diagnoses.
Measures
Negative Symptoms. The NSI-PR (25,27) was adminis-
tered to assess negative symptom domains. Items were
averaged for each negative symptom subscale to create five
domain scores (avolition, asociality, anhedonia, blunted affect,
alogia). All raters went through a gold standard training pro-
gram for reliability purposes. See the Supplement for more
details regarding this interview.
Information was also obtained regarding internal experience
(e.g., wanting to spend time with friends, thinking about goals)
and behavior (e.g., amount of time spent with friends, engaging
in goal-directed activities) for avolition and asociality specif-
ically, in line with negative symptom studies in schizophrenia
(5). Discrepancies between internal experience and behavior
(i.e., higher difference scores) are meaningful in separating
phenomenology from behavior. Furthermore, higher difference
scores could be reflective of secondary sources of negative
symptoms. While internal experience and behavioral analyses
n Science September 2021; 1:210–218 www.sobp.org/GOS 211
16. http://www.sobp.org/GOS
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
as well as differences scores are not central to the study, we
do include findings in the supplemental analyses (see more
information below).
Measures Assessing Sources of Secondary Negative
Symptoms. Selective serotonin reuptake inhibitor (SSRI):
Participants provided information regarding whether they were
currently prescribed an SSRI medication during the back-
ground section of the assessment. The variable of interest was
dichotomized (yes/no) to assess current use.
Anxiety: Anxiety scores were a combination of self-report
measures available—the State-Trait Anxiety Inventory (STAI),
Trait Version (35), Anxiety subscale (35) (n = 85) and the Beck
Anxiety Inventory (36) (n = 102). The STAI questionnaire mea-
sures symptoms of generalized anxiety, excluding items
loading on a depression factor. Final variables were sums of all
item responses, and both scales were z scored to combine into
a broader anxiety domain and limit missing data in analyses.
Analyses with just the STAI (and not Beck Anxiety Inventory)
are included in the Supplement.
Depression: Depression was scored using a combination of
self-report measures available as well—Center for Epidemio-
logical Studies, Depression Scale (CES-D) (37) (n = 83) and the
Beck Depression Inventory (38) (n = 101). The CES-D is a
shortened version of the original CES-D scale, which includes
14 items assessing the severity of depressive symptoms in the
17. past week. Final variables were sum scores of all item re-
sponses, and both scales were z scored to combine into a
broader depression domain and limit missing data in analyses.
Analyses with just the CES-D (and not Beck Depression In-
ventory) are included in the Supplement.
Unusual thought content/delusional ideas: As mentioned,
the SIPS was used to identify a risk syndrome and includes
several questions intended to assess the presence and
severity of unusual thought content/delusional ideas. There are
a total of five questions assessing perplexity and delusion
mood, six for first-rank symptoms, five for overvalued beliefs,
three for other unusual thoughts, and two for nonpersecutory
ideas of reference. See the Supplement for example questions.
A rating is given on a 0 (absent) to 6 (severe and psychotic)
scale based on question responses.
Disorganized communication: The disorganized communi-
cation rating from the SIPS was also used in analyses. This
variable probes for difficulties in thinking reflected in speech.
In
addition to question responses, behavioral observations dur-
ing the clinical interview (e.g., coherence during the interview)
are taken into account in the final rating.
Data Analysis
Levine’s test of homogeneity of variance indicated that SIPS-
attenuated positive symptoms were not different across
sites, so the samples were combined. To begin with, site dif-
ferences were examined in negative symptom domains. Where
negative symptom scores were significantly different across
sites, site was controlled for in analyses, and a note was made
as to whether this was a significant predictor. Regression an-
alyses included both simultaneous linear regression and hier-
archical partitioning, and a false discovery rate was used to
18. account for multiple comparisons in central analyses. Linear
212 Biological Psychiatry: Global Open Science September
2021; 1:21
regression models examined overall model fit and unique ef-
fects of each predictor variable (SSRI medications, anxiety
scores, depression scores, unusual thought content, disorga-
nized communication). If the overall regression model was
significant or at trend level, hierarchical partitioning (39) was
used to investigate contributions of predictors independent of
all other predictors. Hierarchical partitioning averages across
all possible permutations of a regression model to determine
the proportion of predictive value contributed by each inde-
pendent variable in a statistical model. In contrast to traditional
regression, hierarchical partitioning can target each predictor’s
relative explanatory weight without being influenced by multi-
collinearity and dependencies. Hierarchical partitioning was
used using the R statistical software (Version 3.5.1) package
hier.part to examine the proportion of variance in each of the
five negative symptom domains (avolition, asociality, anhe-
donia, blunted affect, alogia) accounted for by common sec-
ondary negative symptoms (SSRI use, anxiety, depression,
unusual thought content, disorganized communication). In
addition, we included analyses assessing motor abnormalities
from the Sensorimotor and Activity Psychosis-Risk scale to
investigate the contributions of this possible secondary source
on negative symptoms (see the Supplement) (40). We did not
evaluate antipsychotic medications owing to limited sample
size reporting current use.
Ethical Standards
All procedures contributing to this work comply with the ethical
standards of the relevant national and institutional committees
on human experimentation and with the Helsinki Declaration of
1975, as revised in 2008.
19. RESULTS
Demographics
The sample consisted of individuals with an average age of 20
years (mean [6 SD], 19.90 [2.21]) and included 45% males and
54% females. The average parental education was an Asso-
ciate’s degree or 2 years in college. In terms of race and
ethnicity, the sample was diverse (Asian = 15%, Black = 15%,
White = 58%, American Indian = 3%, Native Hawaiian or Pa-
cific Islander = 1%, and Hispanic = 19%). Participants
endorsed attenuated positive symptoms with an average sum
score of 11 (3.99) and exhibited mild-moderate levels of
disorganized communication (1.65 [1.25]) and unusual thought
content (3.05 [1.13]). In addition, approximately 15% of the
sample were taking SSRI medications. Approximately 26% of
the sample met DSM criteria for substance use–related dis-
orders, 36%met the criteria for depressive disorders, and 50%
met the criteria for anxiety disorders. Participants reported
negative symptoms that ranged from absent to severe (anhe-
donia, 1.42 [1.09]; avolition, 1.55 [1.18]; asociality, 1.54
[1.22];
alogia, 0.83 [1.19]; blunted affect, 1.32 [1.25]). In addition,
participants reported a range of depression and anxiety scores
as well in the mild to severe range (STAI, 18.39 [5.24]; Beck
Anxiety Inventory, 18.61 [12.63]; CES-D, 19.87 [5.62]; Beck
Depression Inventory, 16.57 [11.59]). There were site differ-
ences in avolition (F188 = 3.93, p = .02), blunted affect (F186 =
3.43, p = .03), and alogia (F185 = 5.65, p = .004) scores. Given
0–218 www.sobp.org/GOS
http://www.sobp.org/GOS
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
20. Psychiatry:
GOS
these site differences, site was a covariate in subsequent
analyses.
Proportion of Variance in Five Negative Symptom
Domains Accounted for by Common Secondary
Sources
Avolition. The overall regression model, when controlling for
site, was significant (R2 = 0.14, F6,169 = 4.52, pcorrected =
.001).
Regression analyses indicated that depression explained the
largest portion of variance in the model (b = 0.40, p = .0002).
Hierarchical partitioning analyses confirmed findings (see
Figure 1).
Asociality. Regression analyses indicated a significant
overall model fit (R2 = 0.10, F5,168 = 3.78, pcorrected = .001)
and
suggested that depression (b = 0.35, p = .002) explained a
large portion of the variance in asociality, and disorganized
communication was at trend level (b = 0.14, p = .08). Similarly,
hierarchical partitioning confirmed these findings, as shown in
Figure 1.
See Table S1 for findings showing overall regression model
fit in avolition behavior and internal experience (n = 134) and
in
asociality behavior (n = 132) and internal experience (n = 131)
in a sample with available data. In addition, see Table S2,
which displays the proportion of variance accounted for by
common secondary sources in avolition behavior and aso-
ciality internal experience (i.e., negative symptom regression
models that were significant from Table S1). Findings from
regression analyses and hierarchical partitioning indicated that
21. anxiety explained the largest proportion of variance in avolition
behavior, while no findings were observed with avolition in-
ternal experience. Furthermore, depression explained most of
the variance in asociality internal experience, but no findings
were observed with asociality behavior. See the Supplement
for correlations between behavior-internal experience differ-
ence scores and secondary sources investigated (no signifi-
cant findings) (Table S3).
Anhedonia. The overall regression model was significant
(R2 = 0.08, F5,170 = 2.81, pcorrected = .02). Regression
findings
Biological Psychiatry: Global Ope
revealed that depression explained most of the variance in
anhedonia (b = 0.26, p = .01). Hierarchical partitioning
confirmed these analyses.
Blunted Affect. There was a significant overall model fit
(R2 = 0.11, F6,167 = 3.27, pcorrected = .002). Regression
analyses
indicated that anxiety explained a large portion of variance in
blunted affect (b = 20.30, p = .008). It is also important to note
that site was also a significant predictor (p = .02). Hierarchical
partitioning confirmed regression findings.
Exploratory analyses were conducted unpacking blunted
affect to investigate the proportion of variance in each of the
three blunted affect items (body gestures, blunted facial affect,
blunted vocal affect) accounted for by common secondary
negative symptoms (see Table 1). Linear regression revealed a
significant overall model fit for blunted facial affect (F5,170 =
4.59, p = .0006, R2 = 0.12), suggesting that anxiety (b = 20.49,
p = .0001) and depression (b = 0.44, p = .0004) explained a
large portion of the variance in the model. Hierarchical parti-
tioning confirmed these findings as well. There was also a
significant model fit for reductions in body gestures (F7,166 =
22. 3.00, p = .005, R2 = 0.11), with disorganized communication
explaining a portion of the variance at trend level (b = 0.15, p =
.12) and anxiety at trend level (b =20.23, p = .09). Site was also
a significant predictor in the model (p = .01) and was controlled
for in this analysis. Hierarchical partitioning confirmed these
findings. Finally, the linear regression model was not statisti-
cally significant for blunted vocal affect (F5,168 = 1.95, p =
.09,
R2 = 0.05), and thus, hierarchical partitioning was not used.
Alogia. When controlling for site, the overall regression model
was significant (R2 = 0.13, F7,167 = 3.51, pcorrected = .002),
suggesting that SSRI medication use (b = 0.54, p = .03) and
depression (b = 0.23, p = .04) explained the largest proportion
of variance in alogia. Site was also a significant predictor
(p = .002). Hierarchical partitioning showed a similar pattern.
Longitudinal Analyses
See Table S5 for longitudinal analyses conducted with
available 12-month follow-up data (baseline secondary
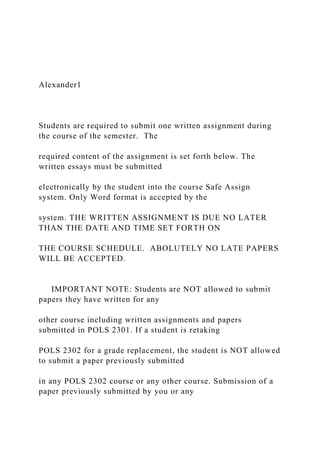
Figure 1. Proportion of variance in negative
symptom domains accounted for by common
secondary sources in a clinical high-risk sample
(N = 192). Effects $30% are labeled. Negative
symptom domains (i.e., avolition, asociality, anhe-
donia, blunted affect, alogia) represent domain
scores from the Negative Symptom Inventory-
Psychosis Risk. *Indicates that the regression
model was significant, p , .05. Selective serotonin
reuptake inhibitor (SSRI) scores are dichotomous
(yes/no). Anxiety scores were collected using the
State-Trait Anxiety Inventory, Trait Version, Anxiety
Subscale, and Beck Anxiety Inventory. Depression
scores are sum scores from the Center for Epide-
miological Studies, Depression Scale and Beck
Depression Inventory. Unusual thought content
23. and disorganized communication are domain
scores from the Structured Interview for Psychosis-
Risk Syndromes. BA, blunted affect.
n Science September 2021; 1:210–218 www.sobp.org/GOS 213
http://www.sobp.org/GOS
Table 1. Proportion (%) of Variance in Blunted Facial
Expressions and Body Gestures Accounted for by
Common Secondary Negative Symptoms in a Clinical High-
Risk Sample
Secondary Negative
Symptoms
Blunted Facial
Expressions
Blunted Body
Gesturing
SSRI 0 17
Anxiety 45 28
Depression 36 7
Unusual Thought Content 8 14
Disorganized
Communication
10 34
24. Blunted affect specific negative symptom items (i.e., blunted
facial
expressions and body gesture) from the Negative Symptom
Inventory-Psychosis Risk. Blunted vocal affect was not
included,
given that the regression analyses were not significant, so
hierarchical partitioning was not used. SSRI scores are
dichotomous
(yes/no). Anxiety scores were collected using the State-Trait
Anxiety
Inventory, Trait Version, Anxiety Subscale, and Beck Anxiety
Inventory. Depression scores are sum scores from the Center for
Epidemiological Studies, Depression Scale and the Beck
Depression
Inventory. Unusual thought content and disorganized symptoms
are
domain scores from the Structured Interview for Psychosis-Risk
Syndromes.
SSRI, selective serotonin reuptake inhibitor.
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
sources predicting follow-up negative symptoms, controlling
for baseline negative symptom scores). Analyses suggested
that SSRI use and disorganized communication significantly
predicted anhedonia (n = 55), unusual thought content and
SSRI use significantly predicted blunted affect (n = 56), and
unusual thought content significantly predicted alogia (n = 57)
at follow-up.
Differences in Secondary Sources of Negative
Symptoms Between Males and Females
25. Given the differences in the distribution of biological sex,
supplemental analyses were conducted to investigate in-
teractions between sex and secondary sources in predicting
negative symptoms. There were significant interactions for
Table 2. Regression Findings Reflecting the Proportion of V
Common Secondary Sources by Biological Sex in a Clinical
High
Domain R2 F (df) p Value Signific
Females (54%)
Avolition 0.10 1.74 (6,93) .12 N/A
Asociality 0.05 1.08 (5,94) .38 N/A
Anhedonia 0.05 0.92 (5,94) .47 N/A
Alogia 0.16 2.85 (6,93) .01 SSRI
Males (45%)
Avolition 0.26 3.39 (7,68) .004 Depress
Asociality 0.28 5.21 (5,68) .004 Depress
Anhedonia 0.19 3.33 (5,70) .009 Depress
Alogia 0.21 2.61 (7,67) .02 Depress
Negative symptom domains are taken from the Negative
Symptom Invent
Anxiety Inventory, Trait Version, Anxiety Subscale, and Beck
Anxiety
Epidemiological Studies, Depression Scale and the Beck
Depression Inven
26. NA, not applicable; SSRI, selective serotonin reuptake
inhibitor; UTC, un
214 Biological Psychiatry: Global Open Science September
2021; 1:21
avolition (F11,163 = 2.91, p = .002), asociality (F11,161 = 2.97,
p =
.001), anhedonia (F11,163 = 1.98, p = .03), and alogia (F11,162
=
2.24, p = .01).
When unpacking significant interaction effects (and con-
trolling for site in analyses with avolition and alogia) in the fe-
male group, secondary sources did not predict avolition,
asociality, or anhedonia (see Table 2). However, SSRI use did
explain some of the variance in alogia (20% were on SSRIs). In
the male group, depression explained a large portion of the
variance in avolition, asociality, anhedonia, and alogia (see
Figure 2). Please note that in the sample of males, 25%met the
criteria for depression, 29% met the criteria for anxiety, and
8% were on SSRIs.
DISCUSSION
To our knowledge, this is the first study to examine the pro-
portion of variance in negative symptom domains accounted
for by common secondary sources in a sample of individuals
meeting criteria for a CHR syndrome. These findings revealed
differences in secondary source contributions in negative
symptom domains, suggesting heterogeneity across these
symptoms in their potential influences on specific negative
symptoms. To ensure unbiased estimates of each predictor’s
effects, we conducted hierarchical partitioning analyses to
partition the explained variance while adjusting for possible
multicollinearity. The hierarchical partitioning results indicate
the proportion of the explained variance accounted for by each
27. predictor. Overall, proportions of variance by these models
were in the small-medium range (41). The central takeaway of
these findings is that secondary sources contribute a sub-
stantial portion of variance in negative symptom severity
scores (suggestive of driving negative symptoms, although
future research is warranted) in negative symptoms, and re-
sults provide information regarding which secondary sources
may be particularly relevant for specific negative symptoms.
Together, these data suggest that considering secondary
sources in vulnerability models, the prevention of psychosis,
and treatment development for negative symptoms are critical.
ariance in Negative Symptom Domains Accounted for by
-Risk Sample
ant Secondary Source Predictor b p Value
N/A N/A
N/A N/A
N/A N/A
0.72 .006
ion, UTC 0.54, 0.30 .0004, .05
ion 0.68 ,.001
ion 0.48 .002
ion 0.51 .003
ory-Psychosis Risk. Anxiety scores were collected using the
State-Trait
Inventory. Depression scores are sum scores from the Center for
tory.
28. usual thought content.
0–218 www.sobp.org/GOS
http://www.sobp.org/GOS
Figure 2. Proportion of variance in negative symp-
tom domains accounted for by common secondary
sources in male clinical high-risk sample (45% of the
whole sample). Effects $30% are labeled. Negative
symptom domains that had significant interactions are
included (i.e., asociality, anhedonia, blunted affect,
alogia) and represent domain scores from the Negative
Symptom Inventory-Psychosis Risk. *Indicates
regression model was significant, p , .05. Selective
serotonin reuptake inhibitor (SSRI) scores are dichoto-
mous (yes/no). Anxiety scoreswere collected using the
State-Trait Anxiety Inventory, Trait Version, Anxiety
Subscale, and Beck Anxiety Inventory. Depression
scores are sum scores from the Center for Epidemio-
logicalStudies,DepressionScaleandBeckDepression
Inventory. Unusual thought content and disorganized
communication are domain scores from the Structured
Interview for Psychosis-Risk Syndromes.
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
While this study did not systematically assess for primary and
secondary symptoms (i.e., using tools and interviews designed
for this), these data also provide foundation for additional work
for this area.
A consistent finding in this study across analyses with
29. negative symptom domains was that mood symptoms
contributed to large portions of variance in negative symp-
toms. Specifically, results indicated that depression explained
the largest proportion of variance avolition (68%), asociality
(58%), and anhedonia (64%). In addition, anxiety explained a
large portion of variance in blunted affect (40%), particularly
blunted facial affect. Together, these data indicate that
depression and anxiety may be useful treatment targets for
individuals presenting with clinical elevations in these negative
symptom domains. Depression and anxiety are common co-
morbid diagnoses in this group (30,42–45) and are large con-
tributors to seeking treatment initially (45). Along these lines,
depression and anxiety are suggested to predict transition to
psychosis and are correlated with negative symptoms in
studies with CHR groups (31). While findings with depression
were not surprising, results suggesting that anxiety predicts
blunted affect (particularly blunted facial affect) were not what
we expected. It is possible that in social situations, individuals
may be threat activated, which in turn contributes to reduced
cognitive resources and variability in displays of facial ex-
pressions. In contrast, when thinking about the other direction
of findings, it is possible that blunted affect may lead to
negative social evaluation and responses (e.g., rejection),
which in turn could contribute to anxiety. While all speculative,
these data do highlight the interconnected nature of anxiety
and blunted facial affect that may be a topic of further inquiry
in
future work.
In analyses with alogia, SSRI medication use and depres-
sion explained the largest proportion of variance. Given the
findings suggesting overlaps between depression and nega-
tive symptom severity in schizophrenia (46) and CHR groups
(24,47), it is expected that SSRI use would explain some of the
variance in negative symptoms. While speculative, it is
possible that SSRI use (e.g., medication side effect) may
30. induce alogia. Alternatively, increased alogia may cause clini-
cians to prescribe SSRIs more often.
Biological Psychiatry: Global Ope
Furthermore, disorganized communication explained some
of the proportion of variance in asociality and reduction in body
gestures. Disorganized communication from the SIPS (33) re-
flects disorganized thinking or thought disorder, observed
through speech (e.g., tangential, circumstantial speech). From
a cognitive perspective, it is possible that disorganized
communication may be contributing to negative symptoms,
such as blunted affect, through a cognitive pathway in which
processing and coordinating information becomes overloaded
(48). It is also important to note that site was a significant
predictor in analyses with blunted affect, particularly blunted
body gestures (as well as alogia). While this is the limitation of
this study, it also may suggest that blunted affect and alogia
may vary depending on geographic location, community, and
cultural context. However, further research investigating this is
needed.
Our findings also indicated that males in our sample
endorsed secondary sources that explained large amounts of
the variance in the five negative symptom domains. Specif-
ically, in the male group, depression explained a large portion
of the variance in negative symptoms. Furthermore, these
findings are in contrast to results with female subjects in whom
no significant findings were observed except with alogia.
Specifically, SSRI medication use explained a portion of the
variance in alogia. Together, these data suggest that it would
be valuable to consider biological sex in the treatment of
secondary sources and negative symptoms. However, addi-
tional research is warranted.
As noted, these data have important clinical implications for
vulnerability models, the prevention of psychosis, and treat-
ment development. First, these data provide support for the
31. possibility of staging models to be updated to include earlier
phases that focus on negative symptoms specifically, perhaps
with a critical role for general symptoms (e.g., anxiety) that are
common secondary sources. At present, these models do not
fully incorporate negative symptoms. This is a gap in these
heuristics because negative symptoms often develop years
before attenuated positive symptoms and predict conversion
more strongly when they occur before age 18 (49). Critically,
future research is needed to determine whether those with
primary or secondary negative symptoms are more likely to
n Science September 2021; 1:210–218 www.sobp.org/GOS 215
http://www.sobp.org/GOS
Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
convert; however, CHR clinics would benefit from assessing
negative symptoms and common secondary sources concur-
rently to capture both possibilities. Second, relatedly, findings
have implications for conversion, suggesting that the combi-
nation of negative, positive, disorganized, and general symp-
toms variables into the same predictive models may be
beneficial. If secondary factors are driving negative symptoms,
the combination of negative symptoms along with these sec-
ondary sources may enhance risk calculators; however, this
has not yet become practice in current risk prediction algo-
rithms. Incorporating next-generation measures, such as the
NSI-PR, that are capable of assessing negative symptoms per
modern conceptualizations should maximize predictive po-
tential. Third, findings have implications for understanding the
mechanisms underlying negative symptoms. It may be bene-
ficial to examine the presence of equifinality and determine
whether, much like schizophrenia (50), CHR cases can develop
32. the same negative symptom profiles due to different underlying
mechanisms. The greater preponderance of secondary nega-
tive symptoms in CHR groups makes this especially likely,
particularly given the wide range of secondary sources driving
heterogeneity in negative symptoms. Identifying the mecha-
nisms underlying these given domains will be necessary for
developing effective treatments for each distinct target.
A potential treatment avenue might include a greater focus
on adequately treating secondary sources. For example, given
the prevalence of depression and anxiety in CHR groups,
psychotherapies designed to target these comorbid condi-
tions, such as cognitive behavioral therapy, are particularly
relevant and implicated. Other treatment examples for sec-
ondary sources might include specific interventions to target
communication deficits resulting from medication side effects,
such as noninvasive brain stimulation or psychotherapy or
both, as these communicative deficits are critical for social
cognitive functions. In schizophrenia, secondary sources are
themselves responsive to treatments and, once effectively
targeted, lead to a concurrent improvement in negative
symptoms (16). Adequate assessment will be a critical step in
this process. Commonly used scales for this group, such as
the SIPS, have significant limitations in their negative symptom
items (27). However, scales based on modern conceptualiza-
tions, such as the NSI-PR, may isolate the constructs with
greater precision and allow for adequate delineation of the
contribution of secondary sources when used in combination
with additional measures assessing these factors.
While there are many strengths to the current study, there
are important limitations to discuss. In our study, we did not
examine all potential sources of secondary negative symptoms
(e.g., neurodevelopmental problems) (48); additional research
should consider assessing other types of secondary sources
as well. Further research is also needed to tease apart mech-
33. anistic pathways that may be underlying secondary sources of
negative symptoms. Another critical direction involves
assessing different types of anxiety and depressive symptoms
as well as using instruments assessing mood symptoms that
also capture resulting blunted affect and alogia; given that we
did not see depression accounting for any of the variance in
blunted affect or alogia, it is possible that this may be due to
overlap in measurement content across constructs. In our
study, most participants met inclusion criteria for attenuated
216 Biological Psychiatry: Global Open Science September
2021; 1:21
positive symptom syndrome; future work assessing these
research questions in different subgroups (e.g., genetic) is
needed. There were also site differences in negative symptom
domains, and it is possible that geographic (e.g., urban),
contextual, cultural, and other environment-related factors
may play a role in the expression and manifestation of these
symptoms; future research on these topics is warranted.
Importantly, we did not attempt to isolate a primary negative
symptom subgroup, given that the tools to make the deficit
syndrome categorization have not been developed or validated
in CHR. Future work should consider developing instruments
and tools to specifically isolate primary and enduring negative
symptoms in CHR, similar to what has been done in schizo-
phrenia. Considering both current and past medications (e.g.,
past SSRI use) and other medications (e.g., serotonin-norepi-
nephrine reuptake inhibitors, antipsychotics) is also a critical
future direction. Along these lines, additional investigation of
motor abnormalities, which are prevalent in early psychosis
even outside of medication use, is critical, as these may have
an impact on negative symptoms.
ACKNOWLEDGMENTS AND DISCLOSURES
The research reported in this article was supported by the
National Institute
of Mental Health (Grant Nos. F31MH121018-01A1 [to TG],
34. RO1MH112545
[to VAM], R01MH112613 [to LME], and R01MH112612 to
[JS]).
TG, VAM, and GPS developed the study concept and design in
consultation with JS, LME, HRC, and AP-B. TG, VAM, JS,
LME, HRC, and
AP-B contributed to data collection. TG in consultation with
HRC, VAM,
GPS, JS, LME, and AP-B conducted data analyses. TG
interpreted findings
under the supervision of VAM and GPS and in consultation with
JS, LME,
HRC, and AP-B. TG drafted the manuscript, and all authors
contributed to
revisions. All authors approved this version of the manuscript
before
submission.
The authors report no biomedical financial interests or potential
conflicts
of interest.
ARTICLE INFORMATION
From the Departments of Psychology (TG, HRC, VAM),
Psychiatry (VAM),
and Medical Social Science (VAM), and Institute for Policy
Research (VAM),
Northwestern University, Evanston, Illinois; Department of
Psychology
(GPS), University of Georgia, Athens, Georgia; Department of
Psychiatry
(AP-B), University of North Carolina at Chapel Hill, Chapel
Hill, North Car-
olina; Department of Psychology (LME), Temple University,
Philadelphia,
Pennsylvania; Department of Psychology (JS), University of
35. Maryland, Bal-
timore County, Baltimore, Maryland; and Department of
Psychological
Science (JS), University of California, Irvine, Irvine,
California.
Address correspondence to Tina Gupta, M.A., at
[email protected]
northwestern.edu.
Received Feb 2, 2021; revised Apr 30, 2021; accepted May 18,
2021.
Supplementary material cited in this article is available online
at https://
doi.org/10.1016/j.bpsgos.2021.05.008.
REFERENCES
1. Bleuler E (1950): Dementia Praecox, or the Group of
Schizophrenias.
New York: International Universities Press.
2. Kraepelin E (1919): Dementia Praecox and Paraphrenia. New
York:
Robert E. Kreiger Publishing Co., Inc.
3. Blanchard JJ, Cohen AS (2006): The structure of negative
symptoms
within schizophrenia: Implications for assessment. Schizophr
Bull
32:238–245.
4. Horan WP, Kring AM, Gur RE, Reise SP, Blanchard JJ
(2011): Devel-
opment and psychometric validation of the Clinical Assessment
0–218 www.sobp.org/GOS
37. 7. Chang WC, Strauss GP, Ahmed AO, Wong SCY, Chan JKN,
Lee EHM,
et al. (2021): The latent structure of negative symptoms in
individuals
with attenuated psychosis syndromes and early psychosis:
Support
for the 5 consensus domains. Schizophr Bull 47:386–394.
8. Ahmed AO, Kirkpatrick B, Galderisi S, Mucci A, Rossi A,
Bertolino A,
et al. (2019): Cross-cultural validation of the 5-factor structure
of
negative symptoms in schizophrenia. Schizophr Bull 45:305–
314.
9. Strauss GP, Nuñez A, Ahmed AO, Barchard KA, Granholm E,
Kirkpatrick B, et al. (2018): The latent structure of negative
symptoms
in schizophrenia. JAMA Psychiatry 75:1303.
10. Strauss GP, Esfahlani FZ, Galderisi S, Mucci A, Rossi A,
Bucci P, et al.
(2019): Network analysis reveals the latent structure of negative
symptoms in schizophrenia. Schizophr Bull 45:1033–1041.
11. Mucci A, Vignapiano A, Bitter I, Austin SF, Delouche C,
Dollfus S, et al.
(2019): A large European, multicenter, multinational validation
study of
the Brief Negative Symptom Scale. Eur Neuropsychopharmacol
29:947–959.
12. Ang MS, Rekhi G, Lee J (2019): Validation of the Brief
Negative
Symptom Scale and its association with functioning. Schizophr
Res
38. 208:97–104.
13. Strauss GP, Ahmed AO, Young JW, Kirkpatrick B (2019):
Reconsi-
dering the latent structure of negative symptoms in
schizophrenia: A
review of evidence supporting the 5 consensus domains.
Schizophr
Bull 45:725–729.
14. Carpenter WT Jr, Heinrichs DW, Wagman AM (1988):
Deficit and
nondeficit forms of schizophrenia: The concept. Am J
Psychiatry
145:578–583.
15. Kirkpatrick B, Buchanan RW, Ross DE, Carpenter WT
(2001):
A separate disease within the syndrome of schizophrenia. Arch
Gen
Psychiatry 58:165–171.
16. Kirschner M, Aleman A, Kaiser S (2017): Secondary
negative symp-
toms — A review of mechanisms, assessment and treatment.
Schiz-
ophr Res 186:29–38.
17. Fusar-Poli P, Papanastasiou E, Stahl D, Rocchetti M,
Carpenter W,
Shergill S, McGuire P (2015): Treatments of negative symptoms
in
schizophrenia: Meta-analysis of 168 randomized placebo-
controlled
trials. Schizophr Bull 41:892–899.
39. 18. Kelley ME, van Kammen DP, Allen DN (1999): Empirical
validation of
primary negative symptoms: Independence from effects of
medication
and psychosis. Am J Psychiatry 156:406–411.
19. Kulhara P, Avasthi A, Chadda R, Chandiramani K, Mattoo
SK,
Kota SK, Joseph S (1989): Negative and depressive symptoms
in
schizophrenia. Br J Psychiatry 154:207–211.
20. Lysaker PH, Salyers MP (2007): Anxiety symptoms in
schizophrenia
spectrum disorders: Associations with social function, positive
and
negative symptoms, hope and trauma history. Acta Psychiatr
Scand
116:290–298.
21. Cohen AS, McGovern JE, Dinzeo TJ, Covington MA (2014):
Speech
deficits in serious mental illness: A cognitive resource issue?
Schiz-
ophr Res 160:173–179.
22. Strauss GP, Horan WP, Kirkpatrick B, Fischer BA, Keller
WR, Miski P,
et al. (2013): Deconstructing negative symptoms of
schizophrenia:
Avolition–apathy and diminished expression clusters predict
clinical
presentation and functional outcome. J Psychiatr Res 47:783–
790.
23. Fusar-Poli P, Borgwardt S, Bechdolf A, Addington J,
40. Riecher-
Rössler A, Schultze-Lutter F, et al. (2013): The psychosis high-
risk
state: A comprehensive state-of-the-art review. JAMA
Psychiatry
70:107–120.
24. Gupta T, Cowan HR, Strauss GP, Walker EF, Mittal VA
(2021):
Deconstructing negative symptoms in individuals at clinical
high-risk
for psychosis: Evidence for volitional and diminished
emotionality
Biological Psychiatry: Global Ope
subgroups that predict clinical presentation and functional
outcome.
Schizophr Bull 47:54–63.
25. Pelletier-Baldelli A, Strauss GP, Visser KH, Mittal VA
(2017): Initial
development and preliminary psychometric properties of the
Prodro-
mal Inventory of Negative Symptoms (PINS). Schizophr Res
189:43–
49.
26. Piskulic D, Addington J, Cadenhead KS, Cannon TD,
Cornblatt BA,
Heinssen R, et al. (2012): Negative symptoms in individuals at
clinical
high risk of psychosis. Psychiatry Res 196:220–224.
27. Strauss GP, Pelletier-Baldelli A, Visser KF, Walker EF,
Mittal VA (2020):
A review of negative symptom assessment strategies in youth at
clinical high-risk for psychosis. Schizophr Res 222:104–112.
41. 28. Fusar-Poli P, Bonoldi I, Yung AR, Borgwardt S, Kempton
MJ,
Valmaggia L, et al. (2012): Predicting psychosis: Meta-analysis
of
transition outcomes in individuals at high clinical risk. Arch
Gen Psy-
chiatry 69:220–229.
29. Gupta T, Haase CM, Strauss GP, Cohen AS, Mittal VA
(2019): Alter-
ations in facial expressivity in youth at clinical high-risk for
psychosis.
J Abnorm Psychol 128:341–351.
30. Addington J, Piskulic D, Liu L, Lockwood J, Cadenhead KS,
Cannon TD, et al. (2017): Comorbid diagnoses for youth at
clinical high
risk of psychosis. Schizophr Res 190:90–95.
31. Fusar-Poli P, Nelson B, Valmaggia L, Yung AR, McGuire
PK (2014):
Comorbid depressive and anxiety disorders in 509 individuals
with an
at-risk mental state: Impact on psychopathology and transition
to
psychosis. Schizophr Bull 40:120–131.
32. Ellman LM, Schiffman J, Mittal VA (2020): Community
psychosis-risk
screening: An instrument development investigation. J Psychiatr
Brain Sci 5:e200019.
33. McGlashan TH, Miller TJ, Woods SW, Rosen JL, Hoffman
RE,
Davidson L (2001): Structured interview for prodromal
42. syndromes:
PRIME Research Clinic. New Haven, Connecticut: Yale School
of
Medicine.
34. First MB (2014): Structured clinical interview for the DSM
(SCID).
Encycl Clin Psychol 1–6.
35. Bieling PJ, Antony MM, Swinson RP (1998): The State-
Trait Anxiety
Inventory, Trait version: Structure and content re-examined.
Behav
Res Ther 36:777–788.
36. Beck AT, Epstein N, Brown G, Steer RA (1988): An
inventory for
measuring clinical anxiety: Psychometric properties. J Consult
Clin
Psychol 56:893–897.
37. Kohout FJ, Berkman LF, Evans DA, Cornoni-Huntley J
(1993):
Two shorter forms of the CES-D (Center for Epidemiological
Studies Depression) depression symptoms index. J Aging Health
5:179–193.
38. Beck AT, Steer RA, Brown GK (1996): Manual for the Beck
Depression
Inventory-II. San Antonio, TX: Psychological Corporation.
39. Chevan A, Sutherland M (1991): Hierarchical partitioning.
Am Stat
45:90–96.
40. Damme KSF, Schiffman J, Ellman LM, Mittal VA (2021):
43. Sensori-
motor and activity psychosis-risk (SMAP-R) scale: An
exploration
of scale structure with replication and validation. Schizophr
Bull
47:332–343.
41. Cohen J (1988): Statistical Power Analysis for the
Behavioral Science,
2nd ed. Hillsdale, NJ: L. Erlbaum Associates.
42. McAusland L, Buchy L, Cadenhead KS, Cannon TD,
Cornblatt BA,
Heinssen R, et al. (2017): Anxiety in youth at clinical high risk
for
psychosis. Early Interv Psychiatry 11:480–487.
43. Yung AR, Buckby JA, Cosgrave EM, Killackey EJ, Baker K,
Cotton SM,
McGorry PD (2007): Association between psychotic experiences
and
depression in a clinical sample over 6 months. Schizophr Res
91:246–
253.
44. Azar M, Pruessner M, Baer LH, Iyer S, Malla AK, Lepage
M (2018):
A study on negative and depressive symptom prevalence in in-
dividuals at ultra-high risk for psychosis. Early Interv
Psychiatry
12:900–906.
45. Stowkowy J, Colijn MA, Addington J (2013): Pathways to
care for
those at clinical high risk of developing psychosis. Early Interv
Psy-
48. Secondary Sources of Negative Symptoms and CHR Syndrome
Biological
Psychiatry:
GOS
46. Krynicki CR, Upthegrove R, Deakin JFW, Barnes TRE
(2018): The
relationship between negative symptoms and depression in
schizophrenia: A systematic review. Acta Psychiatr Scand
137:380–
390.
47. Vargas T, Ahmed AO, Strauss GP, Brandes CM, Walker EF,
Buchanan RW, et al. (2019): The latent structure of depressive
symptoms across clinical high risk and chronic phases of
psychotic
illness. Transl Psychiatry 9:229.
218 Biological Psychiatry: Global Open Science September
2021; 1:21
48. Strauss GP, Cohen AS (2017): A transdiagnostic review of
negative symptom phenomenology and etiology. Schizophr Bull
43:712–719.
49. Zhang T, Xu L, Tang Y, Li H, Tang X, Cui H, et al. (2019):
Prediction of
psychosis in prodrome: Development and validation of a simple,
personalized risk calculator. Psychol Med 49:1990–1998.
50. Strauss GP, Waltz JA, Gold JM (2014): A review of reward
processing and
motivational impairment in schizophrenia. Schizophr Bull
40:S107–S116.
0–218 www.sobp.org/GOS
http://refhub.elsevier.com/S2667-1743(21)00043-4/sref46
http://refhub.elsevier.com/S2667-1743(21)00043-4/sref46
http://refhub.elsevier.com/S2667-1743(21)00043-4/sref46
50. 2McMaster University, Hamilton, Ontario, Canada; 3Craig
Hospital,
Engelwood, Colorado; 4Washington, DC
Abstract: Individuals with spinal cord injury (SCI) continue to
have shorter life expectancies, limited ability to receive basic
health care, and unmet care needs when compared to the general
population. Primary preventive health care services remain
underutilized, contributing to an increased risk of secondary
complications. Three broad themes have been identified that
limit
primary care providers (PCPs) in providing good quality care:
physical barriers; attitudes, knowledge, and expertise; and
systemic
barriers. Making significant physical alterations in every
primary care clinic is not realistic, but solutions such as seeking
out
community partnerships that offer accessibility or transportation
and scheduling appointments around an individual’s needs can
mitigate some access issues. Resources that improve provider
and staff disability literacy and communication skills should be
emphasized. PCPs should also seek out easily accessible
practice tools (SCI-specific toolkit, manuals, modules, quick
reference
guides, and other educational materials) to address any
knowledge gaps. From a systemic perspective, it is important to
recognize
community SCI resources and develop collaboration between
primary, secondary, and tertiary care services that can benefit
SCI
patients. Providers can address some of these barriers that lead
to inequitable health care practices and in turn provide good
quality, patient-centered care for such vulnerable groups. This
article serves to assist PCPs in identifying the challenges of
providing
equitable care to SCI individuals. Key words: accessibility,
52. 1. Ensure general preventive care is up to date and be aware of
secondary complications (e.g., spasticity, bowel and bladder
dysfunction).
2. Schedule appointments according to patient cares/needs (i.e.,
later day, transportation availability, attendant care).
3. Solicit feedback from patient regarding overall clinic
accessibility.
4. Refer to rehabilitation specialists accordingly.
Case Report
John is a 50-year-old man who is a new
patient presenting for a periodic health exam. He
sustained a complete T3 spinal cord injury (SCI),
American Spinal Injury Association Impairment
Scale (AIS) B, at age 30. Since being discharged
from rehabilitation 20 years ago, he has rarely seen
a primary care physician (PCP). He reports that he
has “put on a few pounds” and is coming in for a
check-up; he’s been having difficulty with a wound
on his buttocks that does not seem to be healing.
He comes in his full-time manual wheelchair and
80 Topics in spinal cord injury rehabiliTaTion/spring 2020
contact within the health care system, and they
have the unique opportunity to help manage SCI
patients’ comprehensive health needs and serve as
a link between the individual and multiple health
care providers. However, the literature has shown
53. that individuals with SCI are less likely to receive
the same basic health care when compared to their
peers and have unmet health care needs.4
The Institute of Medicine states that primary care
is “the provision of integrated, accessible health
care services by clinicians who are accountable for
addressing a large majority of personal health care
needs, developing a sustained partnership with
patients, and practicing in the context of family
and community.”5(p500) SCI patients have special
longitudinal physical and psychosocial needs
that are often not adequately managed within a
primary care setting. Most common issues for their
visit to PCPs include pressure sore management,
bowel and urinary tract dysfunctions, shoulder
pain, spasticity, and autonomic dysreflexia (AD).6
The care is often relationship-based and involves
PCPs and specialists. The special needs often lead
to inadequate treatment of their health issues
and secondary complications, fewer preventive
screenings, and less general health promotion.5,7
This article aims to describe and advocate for
standardized care plans and address barriers that
limit quality primary care for SCI patients.
Barriers to Primary Care
Physical barriers
John may find it hard to get to his family
physician because the clinic may be unsuitable for
easy access. A cross-sectional observation study
looked at barriers to health care access for 108
individuals with SCI (53% with paraplegia, 44%
with tetraplegia) who use wheelchairs as their
54. primary means of mobility. Approximately 91.1%
of participants reported facility, clinic, and exam
room barriers during primary care visits. There
were similar findings with speciality care visits;
80.2% of the participants reported accessibility
issues.8 Despite the Americans with Disability Act
and Rehabilitation Act of 1973, significant barriers
to primary care remain to individuals with physical
disabilities. The box at the beginning of the article
outlines a general health maintenance checklist for
addressing these barriers.
Having accessible parking, ramps, working
elevators, restroom access, and wide doorways
and hallways can markedly improve accessibility.
Approximately one in four patients mentioned
that typically primary care clinics did not account
for the presence of a wheelchair and that the
patients had trouble accessing the examination
table.7,8 In many clinics, the examination tables
require an uphill transfer onto a narrow surface
that usually is not able to be raised or lowered.
The average cost of a high–low examination table
is upwards of $2,000, which is a barrier for many
clinicians. Patients have reported a lack of transfer
aids such as transfer boards, sling, and lifts and
staff who have limited knowledge on how to use
or assist with these safe transfers.7-9 A resource
for office accessibility has been developed by the
Canadian Disability Policy Alliance.10
In the earlier discussed survey of 108 adults with
SCI, 89% reported that they did not have their
weight examined, 88% were not asked to change
into gowns or undress to be thoroughly examined,
55. and 85.2% never got on the examination table.8
A wheelchair-accessible scale can help track a
patient’s weight and body mass index (BMI) and
can provide useful clinical information for the
management of a patient’s overall health. Local or
federal programs can provide financial assistance
for PCPs to improve care accessibility, safety, and
clinical efficiency.11
Transportation is often cited as a major
accessibility barrier in the US SCI community,
and it is a greater problem for patients located in
rural settings because of the long distance to urban
centers.11,12 Understanding and accommodating
client transportation barriers (eg. travel time,
distance, and cost) can lead to improved patient-
centered care. One accommodation could be
proactive outreach to community-centered
partnerships with local buses, access-a-ride,
accessible public transportation, and accessible
Uber/Lyft resources. The willingness of the PCPs
to accommodate afternoon visits and involve care
partners are other ways to address such barriers.13
Primary care staff can advocate by helping
patients navigate a complex system to improve
their transport options. In exceptional cases,
Accessibility After SCI 81
an adapted vehicle that includes hand controls,
adjustable seats, and/or ramps to access the
vehicle can be purchased by patients who
can afford it and want to drive on their own.
56. State-funded programs such as vocational
rehabilitation agencies can be utilized. Hand
controls and other equipment, once purchased,
are transferable to newer vehicles, and most
private companies offer a variety of discounts to
facilitate such transfers. This is important for SCI
patients as it helps them achieve independence
and improve their life satisfaction. PCPs can
facilitate referrals to occupational therapists
or specialty clinics who may provide assistance
with the process of using an adapted vehicle.14
Participants in SCI focus groups have also
advocated for increased use of internet resources
to decrease transportation barriers.13 One such
resource is the development of an online portal
that lists accessible provider directories and their
ratings. Major rehabilitation centers have such
information, but it is not widespread or easily
accessible. A centralized platform can better
inform both patients and PCPs of clinics nearby
that tailor their practice to include individuals
with disability.
These barriers to accessibility have broader
implications. John may not have had any routine
preventive care screenings.4,8,15 The lack of
accessibility and proper equipment not only
in the clinician’s office but also in health care
facilities has resulted in patients receiving fewer
preventive measures, including pap smears, pelvic
examinations, colonoscopies, and mammograms,
compared to non-SCI patients.16 Limited
accessibility has also hindered preventive screening
in other areas such as bone health and dental
care.9,15
57. The development of secondary complications
and the lack of appropriate care pose another
significant set of health care problems. These
complications involve issues related to bowel,
bladder, pain, adaptive equipment, skin, and
spasticity. Up to 34% of all such secondary
complications are preventable with good support
in primary care.17 Other broader issues such
as psychological, sexual, reproductive, lifestyle,
and community functioning contribute to poor
standards of care among SCI patients.15
Attitudes, knowledge, and expertise
The negative stigma, marginalization, and lack
of knowledge surrounding SCI patients often lead
to isolation, exclusion, lack of acceptance, and
embarrassment. These broad themes can result in
inaccurate preconceptions and biases that lead to
delays in diagnosis and treatment and decreased
support. Practitioners need to be aware of and
comfortable in communicating about disability.
Patronizing encounters and the lack of courtesy,
sensitivity, and respect have been frequently
reported by patients.13 Resources that improve
provider disability literacy and communication
should be emphasized.18 Good disability etiquette
such as spending more time with patients, having
a face-to-face conversation, and good support
during physical exams can dramatically improve
the care and perceptions of SCI individuals. When
referring care to other practitioners, providing
resources about disability as part of patient referral
package may help in dispelling misperceptions
and increase awareness of the specific disability
and specific patient needs.13 Empowering PCPs
58. through education and exposure may mitigate
such preconceptions.
PCPs are often uncomfortable in managing
care for SCI patients due to lack of training, low
patient volumes, and the perception of the process
as being time consuming.7,12 This is further
highlighted by 47% of emergency room residents
not having adequate knowledge in six categories
of post-SCI care (autonomic dysreflexia, urinary
tract infection, posttraumatic syringomyelia,
gastrointestinal system problems, pulmonary
disturbances, and cardiac complications).19
Many individuals with SCI have been educated
on some of these aspects of their care in inpatient
rehabilitation centers, and so it is important for
PCPs to demonstrate willingness to collaborate
and build capacity in managing these issues.
Evidence consistently shows that patients with
SCI have a 40% to 60% prevalence of obesity,
which puts them at higher risk for cardiovascular
disease (CVD), cancer, and other metabolic
issues.20 They are 200% more likely to have
cardiovascular issues than their non-SCI peers.21
Body mass index (BMI) is commonly used
among the able-bodied population to calculate
82 Topics in spinal cord injury rehabiliTaTion/spring 2020
risk for CVD, however, this calculation may
give an inaccurate picture of SCI patients’ risk.
Following SCI, patients lose a significant portion
of their lean body mass due to atrophy, and
59. consequently they have a higher percentage of fat
mass that is not represented in a BMI calculation.
Based on the decrease in lean mass and increase
in fat mass, a BMI of >22 has been recommended
to signify risk for obesity and obesity-related
chronic diseases.22 The most accurate way to
assess fat mass would be to use bioelectrical
impedance analysis (BIA), but this requires access
to special equipment and for patients to prepare
for the analysis by fasting. Waist circumference
is a more practical method that can be utilized
without special tools or preparation and has more
recently been utilized to look at obesity and risk
factors in patients with SCI. A recent study found
that a waist circumference measurement of >94
cm correlated to CVD risk factors.23 A limitation
of this cutoff is that waist circumference was
measured in supine at the smallest part of the
waist, which requires the patient to transfer to a
mat or table; this again highlights the importance
of a high–low table and the ability to transfer a
more dependent patient using a lift.
In 2016, a Primary and Community Care Spinal
Cord Injury Summit was conducted in Ontario,
Canada, with the goal of understanding key needs
and future directions.6 The summit involved
key stakeholders such as PCPs, individuals with
SCI, researchers, allied health, policy makers,
and funders. The summit yielded five areas of
recommendation for improving primary care to
individuals with SCI:
• Application of best practices
• Improved knowledge translation and
60. dissemination of information/resources
• Improve accessibility and system issues
• Enhanced SCI research in primary care
• Improved communication between health
sectors
It has been suggested that novel approaches are
needed in managing the care for individuals with
SCI.15 The Mobility Clinic in Ontario, Canada,
has developed an accessible interprofessional
clinic with the objective of facilitating care for
individuals and their PCPs. Resources such as
the Spinal Cord Injury Primary Care Toolkit
(SCIPCT) and accredited Case-Based Learning
Modules (CBLMs) have been developed to help
improve primary care knowledge, and training
other PCPs is a priority.24,25
The needs of individuals with SCI are often
complex and require involvement of more than
the PCP alone. Allied health professionals such as
occupational therapists, physiotherapists, assistive
technology professionals, and dietitians have
specific expertise to assist in providing quality
care for individuals with SCI. They can provide
wheelchair adjustments, home visits, exercise
regimens, rehabilitation, and share community
resources that improve day-to-day functioning
of patients. They often have gone beyond the role
of health providers by using strategies to combat
social isolation and encouraging community
participation.26 Unfortunately, these services are
not uniformly accessible by patients and PCPs
due to issues such as insufficient funding, wait
61. lists, and recruitment challenges, particularly in
rural settings. PCPs and their staff can advocate
for community engagement and can establish
partnerships to share local facilities.26 Therapists
have a vital role in facilitating as social partners,
arranging for peer mentors, bringing together
family and friends, engaging patients in the
community, and problem solving, and they need
to be seen within the context of providing good
primary care.
Primary care delivery model
Despite improvements in care over the last two
decades, there has been limited consensus on a
robust primary care delivery model that supports
content, pathway, and delivery. There are 14 SCI
Model Systems that manage, admit, and advance
the treatment for SCI patients in the United States.2
The US Department of Veterans Affairs Spinal Cord
Injuries and Disorders System of Care consists of
a national network of hubs and spokes. There are
24 hubs that provide primary and specialty care.
Primary care is often delivered at the local “spokes”
sites.27 For example, annual comprehensive exams
are done at the spoke or local clinics compared to
Accessibility After SCI 83
colonoscopy, cancer screening, and management
of refractory secondary complications that are
coordinated with the hub or specialized centers.
This hub and spoke model of care is different
from other models of care employed in Canada
62. and Europe.27 The model has been successful, but
there is little research on its long-term outcomes
compared to the private system of SCI in the
United States.
Due to the complexity of care involved with SCI
patients, interdisciplinary collaboration is needed
within and between settings. Interviews conducted
among health care providers, community-
based non-health providers, and policy makers
managing chronic neurological conditions
including SCI found that there was increased
competition for scarce resources, and there
was duplication of services, limited leadership,
and lack of proper handouts, knowledge, and
expertise.28 Sharing electronic health records and
aligning services across regions also appears to
be a challenge. The goal of educating patients
and their families, having a proactive team of
primary care providers, and having a person-
centered health advocacy can lead to better health
outcomes with SCI.
Case Resolution
John was able to independently transfer
onto the high–low examination table in the
clinic room. On examination, he has a stage 1
pressure injury over the right ischial tuberosity.
You counsel him on proper nutrition, weight
shifts, and use of pressure-reducing devices
and surfaces. A referral to an occupational
therapist to evaluate his wheelchair cushions,
mattress, and bed would be appropriate. Using a
wheelchair-accessible scale, you calculate his BMI
to be 24, which would be considered within the
63. normal weight range for the general population.
However, using a cutoff of 22 for people with
SCI, he now falls at the risk category for obesity
and obesity-related diseases. You recommend a
referral to a nutritionist to discuss dietary and
caloric requirements and encourage him to
exercise. Referral to a physical therapist who can
provide a tailored exercise regimen for home
or the gym can be useful. Lastly, as a PCP you
schedule a follow-up with John in a few weeks
to monitor his pressure injury care and overall
cardiovascular health.
Conclusion
SCI and other physical disabilities are complex,
chronic conditions that often lead to inappropriate
use of health care services, increased health care
costs, and fragmented care. More importantly,
these conditions often lead to poorer overall
individual health outcomes. PCPs need to consider
the physical, attitudinal, knowledge-based, and
systemic barriers that exist and be proactive
in addressing them. Novel and collaborative
approaches are needed to change the trajectory
of care for persons with physical disabilities. By
addressing these barriers and incorporating an
informed team-based approach, PCPs can improve
the quality of patient care and improve individual
health outcomes.
Key Take Home Points
1. Ensure an accessible clinic and equipment
with knowledge of proper use for SCI
64. patients to provide comprehensive care.
2. Be vigilant for common secondary compli-
cations of SCI (primarily bowel, bladder,
autonomic dysreflexia, spasticity, and skin
changes) in addition to diseases that affect
the general population.
3. Identify local rehabilitation centers and
associated assessible clinics near you.
Proactively seek referral sources and
knowledge of community resources such
as rehabilitation centers, local gyms, and
assistive technology professionals.
4. Educate staff about removing attitudinal and
physical barriers in primary care clinic.
Acknowledgments
The authors report no conflicts of interest.
84 Topics in spinal cord injury rehabiliTaTion/spring 2020
REFERENCES
1. Granger C V, Karmarkar AM, Graham JE, et al. The
Uniform Data System for Medical Rehabilitation:
Report of patients with traumatic spinal cord injury
discharged from rehabilitation programs in 2002-
2010. Am J Phys Med Rehabil. 2012;91(4):289-
299. doi:10.1097/PHM.0b013e31824ad2fd
2. Somers MF. Spinal Cord Injury: Functional
65. Rehabilitation. 3rd ed. Upper Saddle River, NJ:
Prentice Hall; 2010.
3. Biering-Sørensen F, DeVivo MJ, Charlifue S, et al.
International Spinal Cord Injury Core Data Set
(version 2.0)-including standardization of reporting.
Spinal Cord. 2017;55(8):759-764. doi:10.1038/
sc.2017.59
4. Noreau L, Noonan VK, Cobb J, Leblond J, Dumont FS.
Spinal cord injury community survey: Understanding
the needs of Canadians with SCI. Top Spinal Cord
Inj Rehabil. 2014;20(4):265-276. doi:10.1310/
sci2004-265
5. Ho CH. Primary care for persons with spinal cord injury -
not a novel idea but still under-developed. J Spinal
Cord Med. 2016;39(5):500-503. doi:10.1080/
10790268.2016.1182696
6. Milligan J, Lee J, Smith M, et al. Advancing primary
and community care for persons with spinal cord
injury: Key findings from a Canadian summit. J Spinal
Cord Med. December 2018:1-11. doi:10.1080/
10790268.2018.1552643
7. Milligan J, Lee J. Enhancing primary care for persons
with spinal cord injury: More than improving physical
accessibility. J Spinal Cord Med. 2016;39(5):496-
499. doi:10.1179/2045772315Y.0000000041
8. Stillman MD, Frost KL, Smalley C, Bertocci G,
Williams S. Health care utilization and barriers
experienced by individuals with spinal cord injury.
Arch Phys Med Rehabil. 2014;95(6):1114-1126.
doi:10.1016/j.apmr.2014.02.005
66. 9. Lofters A, Chaudhry M, Slater M, et al. Preventive care
among primary care patients living with spinal cord
injury. J Spinal Cord Med. 2018:1-7. doi:10.1080/
10790268.2018.1432308
10. Canadian Disability Policy Alliance. Primary Care
Accessibility Checklist. http://69.89.31.83/~disabio5/
wp-content/uploads/2012/09/FHT-access-chklst-24-
Jun-111.pdf. Accessed June 25, 2019.
11. Canadian Disability Policy Alliance. Improving
Accessibility of Family Health Teams Evaluation
Report. http://www.disabilitypolicyalliance.ca/
wp-content/uploads/2014/01/Family-Health-
Teams.pdf. Accessed June 25, 2019.
12. McMillan C, Lee J, Milligan J, Hillier LM, Bauman C.
Physician perspectives on care of individuals with severe
mobility impairments in primary care in Southwestern
Ontario, Canada. Health Soc Care Community.
2016;24(4):463-472. doi:10.1111/hsc.12228
13. Kroll T, Jones GC, Kehn M, Neri MT. Barriers
and strategies affecting the utilisation of primary
preventive services for people with physical
disabilities: A qualitative inquiry. Health Soc Care
Community. 2006;14(4):284-293. doi:10.1111/
j.1365-2524.2006.00613.x
14. Biering-Sørensen F, Hansen RB, Biering-Sørensen
J. Mobility aids and transport possibilities 10-45
years after spinal cord injury. Spinal Cord.
2004;42(12):699-706. doi:10.1038/sj.sc.3101649
67. 15. McColl MA, Aiken A, McColl A, Sakakibara
B, Smith K. Primary care of people with spinal
cord injury: Scoping review. Can Fam Physician.
2012;58(11):1207-1216, e626-35. http://www.
ncbi.nlm.nih.gov/pubmed/23152456.
16. Song SH, Svircev JN, Teng BJ, Dominitz JA, Burns
SP. A safe and effective multi-day colonoscopy bowel
preparation for individuals with spinal cord injuries. J
Spinal Cord Med. 2018;41(2):149-156. doi:10.108
0/10790268.2016.1258968
17. van Loo MA, Post MWM, Bloemen JHA, van Asbeck
FWA. Care needs of persons with long-term spinal cord
injury living at home in the Netherlands. Spinal Cord.
2010;48(5):423-428. doi:10.1038/sc.2009.142
18. United Spinal Association. Disability Etiquette, Tips
on Interacting with People with Disabilities. https://
www.unitedspinal.org/pdf/DisabilityEtiquette.pdf.
Accessed September 25, 2019.
19. DiPonio L, Roth R, Gater D, et al. The management of
patients with chronic spinal cord injury in emergency
departments: Utilization and a knowledge survey of
emergency medicine residents. Top Spinal Cord Inj
Rehabil. 2011;17:38-45.
20. Shojaei MH, Alavinia SM, Craven BC. Management
of obesity after spinal cord injury: A systematic
review. J Spinal Cord Med. 2017;40(6):783-794.
doi:10.1080/10790268.2017.1370207
21. Gorgey AS, Gater DR. Prevalence of obesity after
spinal cord injury. Top Spinal Cord Inj Rehabil.
2007;12(4):1-7. doi:10.1310/sci1204-1
68. 22. Laughton GE, Buchholz AC, Martin Ginis KA, Goy
RE, SHAPE SCI Research Group. Lowering body
mass index cutoffs better identifies obese persons with
spinal cord injury. Spinal Cord. 2009;47(10):757-
762. doi:10.1038/sc.2009.33
23. Ravensbergen HRJC, Lear SA, Claydon VE. Waist
circumference is the best index for obesity-related
cardiovascular disease risk in individuals with spinal
cord injury. J Neurotrauma. 2014;31(3):292-300.
doi:10.1089/neu.2013.3042
24. CFFM FHT Primary Care Mobility Clinic. Provider
Educational Materials. http://mobilityclinic.ca/provider-
educational-materials/. Accessed June 25, 2019.
25. Milligan J, Lee J, Hillier LM, Slonim K, Craven C.
Improving
primary care for persons with spinal cord injury:
Development of a toolkit to guide care. J Spinal Cord
Med. 2018:1-10. doi:10.1080/10790268.2018.
1468584
26. Price P, Stephenson S, Krantz L, Ward K. Beyond my
front door: The occupational and social participation
of adults with spinal cord injury. OTJR Occup Particip
Heal. 2011;31(2):81-88. doi:10.3928/15394492-
20100521-01
27. Donnelly C, McColl MA, Charlifue S, et al. Utilization,
access and satisfaction with primary care among
people with spinal cord injuries: A comparison of
three countries. Spinal Cord. 2007;45(1):25-36.
doi:10.1038/sj.sc.3101933
69. 28. Jaglal SB, Guilcher SJT, Bereket T, et al. Development
of a Chronic Care Model for Neurological Conditions
(CCM-NC). BMC Health Serv Res. 2014;14(1):409.
doi:10.1186/1472-6963-14-409
Copyright of Topics in Spinal Cord Injury Rehabilitation is the
property of Thomas Land
Publishers Incorporated and its content may not be copied or
emailed to multiple sites or
posted to a listserv without the copyright holder's express
written permission. However, users
may print, download, or email articles for individual use.