Cancer of larynx
•Download as PPTX, PDF•
37 likes•15,582 views

Every medical personnel spread your knowledge..... to prevention of cancer of larynx.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cancer of larynx
Similar to Cancer of larynx (20)
More from MR. JAGDISH SAMBAD
More from MR. JAGDISH SAMBAD (20)
Recently uploaded
Recently uploaded (20)
Cancer of larynx
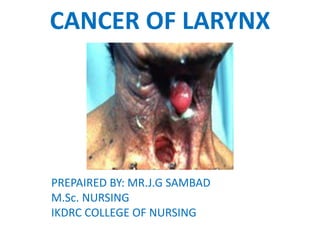
- 1. CANCER OF LARYNX PREPAIRED BY: MR.J.G SAMBAD M.Sc. NURSING IKDRC COLLEGE OF NURSING
- 3. CANCER OF LARYNX • Cancer of larynx accounts for 2% to 3% of all malignancies. Squamous cell carcinoma is the most common malignant tumor of the larynx arising from the membrane lining the respiratory tract.
- 5. Etiology and risk factors – • Smoking • Alcohol • Tobacco chewing • Occupational exposure to asbestos, wood dust, mustard gas, petroleum products • Inhalation of noxious fumes • Chronic laryngitis • Voice abuse • Nutritional deficiency (rivoflavin) • Age after 60 years • Gender (more common in men than woman) • Low immunity
- 7. Clinical manifestation • Hoarseness of voice • Persistant cough • Sore throat • Throat pain • Throat burning (when consuming hot liquids or citrus fruit juice) • Lump is felt in the neck • Dysphagia • Dyspnea • Unilateral nasal obstruction • Nasal discharge • Foul breathing
- 8. Diagnostic evaluation • History taking – family, environmental, habits of alcohol, smoking • Endoscopy (laryngoscopy) • CT scan • MRI • PET • Biopsy
- 9. Medical management • Chemotherapy – for patient with more advanced disease, cisplastin based chemotherapy and radiotherapy protocol have been used. 5 fluorouracil (5-FU) is also used commonly. • Radiation therapy – the goal of chemotherapy is to eradicate the cancer and preserve the function of the larynx. Radiation therapy can be used preoperativy and postoperatively. Radiation therapy is combined with surgery in advanced laryngeal cancer as adjunctive therapy to surgery or chemotherapy and as palliative measure.
- 11. Surgical management 1. Vocal cord stripping – stripping of vocal cord is used to treat dysphagia, hyperkeratosis and leukoplakia. The procedure involves removal of the mucosa of the edge of the vocal cord by using an operating microscope. 2. Cordectomy – surgical removal of vocal cord, is usually performed via transoral laser. 3. Laser surgery – when the tumor size is of small, small tumors are eradicated with the use of laser. Microelectrodes are useful for surgical resection of small tumors of lung.
- 13. 4. Partial laryngectomy – a partial laryngectomy is often used smaller cancers of larynx (small tumor). It is recommended in the early stage of cancer in the glottis area when only one vocal cord is involved. In this, a portion of the larynx is removed, along with vocal cord and the tumor, all other structures remain. 5. Total laryngectomy – in total laryngectomy, the laryngeal structures are removed, including the hyroid bone, epiglottis, cricoids cartilage and two or three rings of trachea. 6. Total laryngectomy results in permanent loss of the voice and a change in the airway, requiring a permanent tracheostomy.
- 14. Nursing management (Pre-operative) 1. Risk for aspiration related to surgical removal of epiglottis and excessive secretion after surgery. 2. Ineffective airway clearance related to excessive secretions after surgery 3. Risk for impaired gas exchange related to excessive secretions after surgery 4. Altered nutrition less than body requirement related to dysphagia.
- 15. Swallowing techniques after a partial larygectomy • Being with soft or semi solid foods • Stay with a nurse or swallowing therapist during meals until you master the technique of swallowing without choking • Be patient, learning to swallow again is frustrating • Follow these steps in sequence – • Take a deep breath • Bear down to close the vocal cords • Place food into your mouth • Swallow • Cough to rid the closed cord of accumulated food particles • Swallow • Cough • Breathe
- 16. Nursing management of patient after larygectomy 1. Nutrition – immediately after surgery, the client’s nutrition is supplemented with tube feedinds. The client continues to receive tube feedings until edema has subsided and suture line healing has occurred. When the client can swallow saliva, oral feedings can begin. The diet usually begins with liquid or semi-soft foods and progresses as healing occurs.
- 17. 2. Communication • Communication – for the first few days after surgery, the client should communicate by writing. Even though the client cannot speak, conversation should still include the client’s input through nodding and pointing and not be directed only to others, such as the family. Avoiding conversation or excessive talking with client because of difficulty in communication is demeaning to the client and leads to frustration.
- 18. 3. Artificial larynx • An artificial larynx may me used as early as 3 to 4 days after surgery. these battery-operated speech devices are held alongside the neck or can be adapted with a plastic tube that is inserted in the mouth. The air inside the mouth is vibrated, and the client articulates as usual. The speech quality is monotone and mechanical-souding but intelligible.
- 19. 4. Esophageal speech • esophageal speech is a technique that requires the client to swallow and hold air in the upper esophagus. By controlling the flow of air, the client can pronounce as many as 6 to 10 words before stopping to swallow more air. The voice is deep but is oud and effective once the technique is mastered.
- 20. 5. Tracheoesophagial Puncture (TEP) • it is a surgical technique that also restores speech. A small puncture is made into the upper tracheostoma to the cervical esophagus for creation of a fistula. After the fistula tract has healed, a small one-way valve, or voice prosthesis, is inserted. • By occlusion of the prosthesis, air can be shunted into the esophagus and used to produce speech. The TEP may be done concurrently with a total laryngectomy or as secondary procedure after healing and radiation therapy. • These devices require maintenance, therefore only clients who are highly motivated, who are able to perform self-care, and who have good manual dexterity are eligible for this procedure.
- 22. SPEECH THERAPY • To plan postoperative communication strategies and speech therapy, the speech therapist or pathologist conduct a preoperative evaluation. During this time, the nurse discusses with the patient and family about methods of communication that will be available in the immediate post-operative period. • These include writing, lip speaking and reading, and communication or word boards. In addition, a long term postoperative communication plan for alaryngeal communication is developed.
- 23. • The important common techniques of alaryngeal communication are- electrolarynx, esophageal speech and tracheoesophageal puncture.