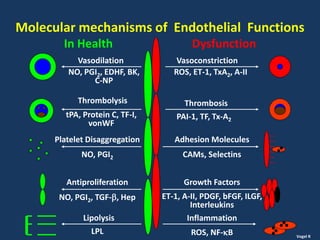
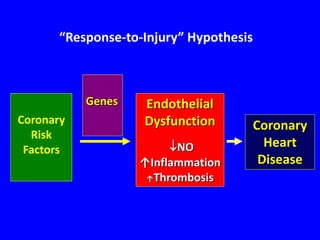
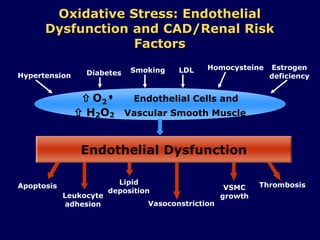
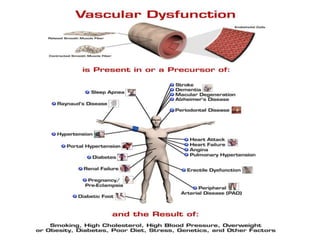
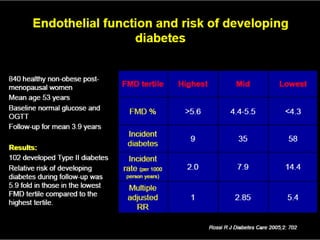
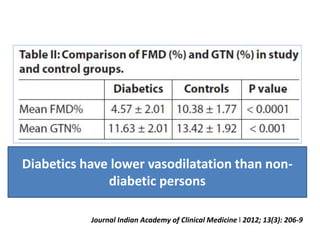
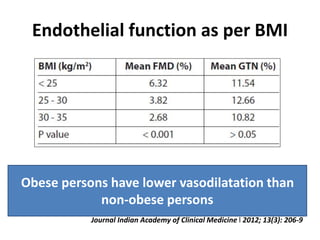
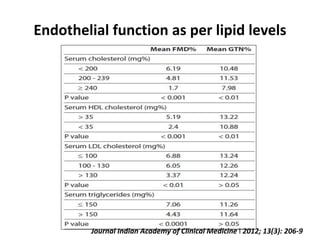
Endothelial dysfunction is prevalent in the Indian population, which suffers from a higher incidence of cardiovascular diseases, diabetes, and hypertension correlated with factors such as obesity and dyslipidemia. Studies show that diabetics have worse endothelial function compared to non-diabetics, with specific assessments indicating lower vasodilation in affected individuals. Understanding and modifying endothelial dysfunction may provide a pathway to reducing cardiovascular risk in India.