
Recommended
Recommended
More Related Content
Similar to Research QuestionORGANIZATIONAL ISSUESCaruana, A. an.docx
Similar to Research QuestionORGANIZATIONAL ISSUESCaruana, A. an.docx (20)
More from gholly1
More from gholly1 (20)
Recently uploaded
Recently uploaded (20)
Research QuestionORGANIZATIONAL ISSUESCaruana, A. an.docx
- 1. Research Question ORGANIZATIONAL ISSUES Caruana, A. and Pitt, L.(1997). INTQUAL-an internal measure of service quality and the link between service quality and business performance. European Journal of Marketing, 31(8), 604-616 Frese, M.(2008). The world is out: we need an active performance concept for modern workplaces. Industrial and Organizational Psychology, 1, 67-69 Frost, F. and Kumar, M.(2001). Service quality between internal customers and internal suppliers in an international airline. International Journal of Quality & Reliability Management, 18(4), 371-386 Graen, G.(2008). Enriched engagement through assistance to systems' change: a proposal. Industrial and Organizational Psychology, 1, 74-75 Johnson, J.(2008). Process models of personality and work behavior. Industrial and Organizational Psychology, 1, 303- 307 Lipman-Blumen, J. and Leavitt, H.(2009). Beyond typical teams: hot groups and connective leaders. Organizational Dynamics, 38(3), 225-233 Macey, W. and Schneider, B.(2008). The meaning of employee engagement. Industrial and Organizational Psychology, 1, 3- 30 Miles, R., Snow, C., Fjestad, O., Miles, G. and Lettl, C.(2010). Designing organizations to meet the 21st century opportunities and challenges. Organizational Dynamics, 39(2), 93-103
- 2. Reynoso, J. and Moores, B.(1995). Towards the measurement of internal service quality. International Journal of Service Industry Management, 6(3), 64-83 A. Independent Variable -social network tie quality B. Dependent Variable -Effectiveness of change Initiatives B1. On time implementation VS resistance B2. The extent to which the new system is applied VS stuck with past Literature and theories Research Method Combination of descriptive and causal researchSurvey-questionnaireQuestions based on scale (Likert)Secondary data (organizational chart, HR statistics, quality dept statistics) Sample (random sampling) Maximum 4 5 star hotels located in Greece, operate on annual basis, family owned or hotel chainsEmployees from all the hierarchy levels General managers or HR managers Important references
- 3. For further information For those of you who are interested in learning more or exchanging thoughts and ideas please feel free to contact me !! Please contact me through Research proposal Control station HOSPITALITY Brownell, J.(2008). A commentary on "Leading change with the 5-p model: complexing the swan and dolphin hotels at Walt Disney World. Cornell Hospitality Quarterly, 49(2), 206-210 Humborstad, S. et al.(2008). Burnout and service employees‘ willingness to deliver quality service. Journal of Human Research in Hospitality & Tourism, 7(1), 45-64 Kim, Y.(2006). Managing workforce diversity: developing a learning organization. Journal of Human Resources in Hospitality & Tourism, 5(2), 69-90 Koutoulas, D.(2009). The 2009 Greek hotel branding report. Athens, GREECE Kuslavan, S. et al.(2010). The human dimension; a review of human resources management issues in the tourism and hospitality industry. Cornell Hospitality Quarterly, 51(2), 171- 214
- 4. Liu, W.P. et all.(2009). Individual change schemas, core discussion network, and participation in change: an exploratory study of Macau casino employees. Journal of Hospitality and Tourism Research, 33(1), 74-92 Poulston, J.(2008). Hospitality workplace problems and poor training: a close r relationship. International Journal of Contemporary Hospitality Management, 20(4), 412-427 Ravichandran, S. et al.(2007). Organizational citizenship behavior research in hospitality: current status and future research directions. Journal of Human Resources in Hospitality & Tourism, 6(2), 59-78 CHANGE Amis, H. , Slack, T. and Hinings, C.R.(2004). The pace, sequence and linearity of radical change. Academy of Management Journal, 47(1), 15-39 Erwin, D. and Garman, A.(2010). Resistance to organizational change: linking research and practice. Leadership & Organization Development Journal, 31(1), 39-56 Ford, JD., Ford, L.W. and McNamara, R.T.(2002). Resistance and the background conversations of change. Journal of Organizational Change Management, 15(2), 105-121 Fucate, M., Kinicki, A. and Prussia, G.E.(2008). Employee coping with organizational change: an examination of alternative theoretical perspectives and models. Personnel Psychology, 61, 1-36 Martin, A.J. et al.(2006). Status differences in employee adjustment during organizational change. Journal of Managerial Psychology, 21(1/2), 145-162 Nerina, L. et al.(2009).Psychological predictors of intentions to engage in change supportive behaviors in an organizational context. Journal of Change Management, 9(3), 233-250 Peus, C. et al.(2009). Leading and managing organizational change initiatives. Management Revue, 20(2), 158-175
- 5. Raferty, A.E and Simons, R.H.(2006). An examination of the antecedents of readiness for fine tuning and corporate transformation changes. Journal of Business and Psychology, 20(3), 325-350 Sherman, S.W. and Garland, G.E.(2007). Where to burry the survivors? Exploring possible ex post effects of resistance to change. SAM Advanced Management Journal, 72(1), 52-62 Vales, E.(2007). Employees can make a difference! Involving employees in change at Allstate Insurance. Organizational Development Journal, 25(4), 27-31 SOCIAL NETWORKS Balkundi, P. and Harrison, D.A.(2006). Ties, leaders, and time in teams: Strong inference about network structure's effects on team viability and performance. Academy of Management Journal, 49(1), 49-68 Borgatti, S. and Cross, R.(2003). A relational view of information seeking and learning in social networks. Management Science, 49(4), 432-445 Brass, D.J. et al.(2004). Taking stock of networks and organizations: A multilevel perspective. Academy of Management Journal, 47(6), 795-817 Bruque, S., Moyano, J. and Eisenberg, J.(2009). Individual adaptation to IT-induced change: The role of social networks. Journal of Management Information Systems, 25(3), 177- 206 Cross, R. and Cummings, J.N.(2004). Tie and network correlates of individual performance in knowledge-intensive work. Academy of Management Journal, 47(6), 928-937 Cummings, J.N. and Higgings, M.C.(2006). Relational
- 6. instability at the network core: Support dynamics in developmental networks. Social Networks, 28, 38-55 Friedkin, N.E. and Johnsen, E.C.(1997). Social positions in influence networks. Social Networks, 19, 209-222 Smith, J.(2009). Solidarity networks: What are they? And why should we care? The Learning Organization, 16(6), 460-468 Tenkasi, R.V.(2003). Social networks and planned organizational change: The impact of strong network ties on effective change implementation and use. The Journal of Applied Behavioral Science, 39(3), 281-300 Totterdell, P. et al.(2004). Affect networks: A structural analysis of the relationship between work ties and job related affect. Journal of Applied Psychology, 89(5), 854-867 “Does employees’ social network tie quality affect the effectiveness of change interventions?” Course, Students names, semester, Variables *Balkundi,P. and Harisson,D.: tie structure and tie content (density, leader centrality) Borgatti, S. and Cross,R.: relational characteristics influencing information seeking *Cummings, J. and Higgins, M.: developmental networks and tie stability *Erwin,D. and Garman,A.: relationships (agent-manager) affect resistance to change *Ford, J. and Ford. L.: resistance and engagement, *Parasuraman, A., Zeithaml, V.A. and Berry, L.L.:SERVQUAL and TERRA *Peus et al.: Uncertainty-fear of failure-discipline in sense making (resistance to change) *Rafferty ,A. and Simmons, R.: readiness for change (factors)
- 7. *Sherman, s. and Garland,G.: resistance to change/cognitive/behavioral/emotional states *Tenkasi, R. and Chesmore, M.: knowledge transfer and network strong ties Relationships 1a.Tie quality 2a. Tie quality 3a. Tie quality 4a. Individuals that create high Quality ties 5a. Individuals that create high quality ties 1b.Resistance to change 2b. Successful application of the new system 3b. Hierarchy levels 4b.Tend to “build” centrality position 5b. Tend to affect the performance of their network members
- 8. This case was prepared by Abeel A. Mangi, EMBA Class of 2016, Cate Reavis, Associate Director, Curriculum Development, and Professor Roberto Fernandez. Names and certain data have been disguised. Copyright © 2016, Abeel A. Mangi, Cate Reavis, and Roberto Fernandez. This work is licensed under the Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 Unported License. To view a copy of this license visit http://creativecommons.org/licenses/by-nc-nd/3.0/ or send a letter to Creative Commons, 171 Second Street, Suite 300, San Francisco, California, 94105, USA. 15-167 May 7, 2016 Conserving Blood During Cardiac Surgery at Huntington University Hospital (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez Patients who underwent cardiac surgery often required a blood transfusion or other blood products. In order for surgeons to work upon or inside the heart, certain parts of the heart or great vessels surrounding it needed to be opened and then repaired with suture material. Opening a chamber of the heart disrupted its hermetic seal and permitted blood to spill out and into the surrounding space. While bleeding was undesirable for obvious reasons, restoring blood via transfusions was not a panacea. According to a 2006 study published in the Annals of Thoracic Surgery, a cardiac patient who received a blood transfusion after an aortic valve replacement (AVR) or a coronary artery bypass
- 9. grafting (CABG) had a 30% lower chance of survival at six months and a 50% lower chance at 10 years.1 The 10-year survival rate without a transfusion was 90%.2 On average, 48.9% of patients in the United States who underwent an AVR or a CABG required a blood transfusion.3 At Huntington University Hospital (HUH), where 500 patients underwent an AVR or CABG annually, the percentage of patients who received blood transfusions in 2011, 2012, and 2013 was around 71%. This was happening at a time when the Affordable Care Act of 2010 was forcing hospitals to provide quality care in a cost efficient way. Dr. Frank Young, who joined HUH’s for Cardiac Medicine in 2011 and whose patients were among the hospital’s sickest, wanted to help bring down the Center’s transfusion rate by leading a blood 1 Koch, C.G., et al. “Transfusion in CABG Is Associated with Reduced Long-Term Survival,” Annals of Thoracic Surgery, 2006, 81:1650-1657. 2 Ibid. 3 Ibid. 2 Ibid. 3 Ibid. CONSERVING BLOOD DURING CARDIAC SURGERY AT HUNTINGTON UNIVERSITY HOSPITAL (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez May 7, 2016 2
- 10. conservation project involving the medical teams that worked together during the intra- and post- operative phases. The goal was to reduce the hospital’s blood product4 utilization during cardiac surgery and after by two-thirds within one year, by the end of 2014, thereby bringing transfusion rates down to the national average and resulting in annual cost savings of $2.5 million. More importantly, it would save the lives of an additional 125 people per year over 10 years. Young knew he faced an uphill battle in convincing his fellow surgeons and the medical teams that accompanied them during surgeries to make changes to their surgical routines. Autonomy was critically important to physicians and he was attempting a professional intervention of sorts. Furthermore, he was a new arrival to HUH, especially considering some of his senior colleagues had spent their entire careers there. Then there was the challenge posed by the complex organizational structure inherent in most teaching hospitals: fellow cardiac surgeons aside, few, if any, members of the medical teams Young worked with during and after surgery reported to him. He would have to convince colleagues, over whom he had no formal influence, that one, there was a problem and, two, that it could be solved as long as they were willing to change their ways. Huntington University Hospital With 7,500 employees including 2,800 nurses, 2,400 university and community physicians, and 400 resident physicians practicing more than 75 medical specialties,
- 11. HUH was the primary teaching hospital for Huntington University Medical School, one of the most renowned medical schools in the United States. In 2013, the hospital generated $1.3 billion in revenue and $120 million in net income. HUH’s Center for Cardiac Medicine, where Young worked, included seven surgeons who together conducted over 900 heart surgeries a year, contributing $130 million in revenue and $12 million in net income. Young joined HUH in 2011 as the surgical director for the Center’s Heart Failure and Cardiac Transplant Program. Prior to joining HUH, he spent two years as a cardiac surgeon at one of the world’s top cardiac care hospitals where medical teams carried out over 4,000 open heart operations a year. Huntington University hired Young to rejuvenate the Center’s heart transplantation program where the number of patients coming in was on the decline and outcomes were unsatisfactory. One medical survey conducted in 2013 ranked HUH #39 for cardiology and heart surgery, giving it very low scores when it came to patient safety and success in preventing major postsurgical bleeding. Despite the poor score, patient safety was a critically important value at HUH. Every month, an email was sent out to the entire hospital staff recognizing specific employees for making a meaningful contribution to patient safety. 4 Blood products include packed red blood cells, fresh frozen plasma, platelets and cryoprecipitate.
- 12. CONSERVING BLOOD DURING CARDIAC SURGERY AT HUNTINGTON UNIVERSITY HOSPITAL (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez May 7, 2016 3 Organizational Structure As Young was getting to know HUH in the first weeks after he arrived, one thing that confounded him was its complex organizational structure. Every cardiac operation involved a 20-person functional team, which included the cardiac anesthesiologist, perfusionist,5 cardiac surgeon, operating room (OR) nurses, intensive care unit (ICU) physicians, physician assistants, and fellows and residents. The functional grouping enabled people with deep expertise and highly specialized knowledge to work together in a coordinated fashion, much like a symphony, as one ICU physician explained, and intermittently allowed for the exchange of human capital from one OR to another when necessary. The time of intra-operative care for heart surgery patients was typically four to six days. From an organizational perspective, there were few formal connections among the members of the team that carried out cardiac surgeries and oversaw a patient’s recovery. Physicians, which included cardiologists, surgeons, anesthesiologists, and ICU physicians, were hired by the medical school and were grouped by function with discrete and hierarchical
- 13. reporting relationships. Young, for example, reported to a section chief. The section chief reported to the chair of the department who in turn reported to the dean of the medical school. Physicians also had opaque compensation and incentive arrangements. Salaries were individually negotiated. There was no group incentive plan for surgeons. The medical school awarded surgeons multi-year contracts and paid the teaching portion of physician salaries, which amounted to less than 7% of their total compensation. Through a complicated arrangement, HUH paid the majority of physician compensation based on how much revenue they generated, which, in the case of heart surgeons, was a considerable amount. The salary structure also helped ensure that HUH and its medical school attracted and retained top talent. Young believed this type of organizational and compensation structure encouraged competition among surgeons and did little to foster camaraderie and teamwork. In contrast, other hospitals, like the one Young worked at prior to HUH, offered yearly contracts and paid everyone a fixed salary. This was thought to encourage group decision- making in the best interest of the patient and discourage competition among surgeons for patients. Meanwhile, perfusionists, nurses, physician assistants, and fellows and residents, all members of a typical surgical team, were hired by the hospital. Like the physicians, these specialists were grouped by function and reported through their own individual chains of commands. Specifically, nurses ultimately reported to the chief nursing officer and perfusionists reported to the director of the
- 14. operating rooms. No one reported to the surgeons. These specialists were paid fixed salaries and were not incentivized by volume. The absence of formal alignment between the two groups meant that there was no formal chain of 5 A perfusionist manages a patient’s physiological status during cardiac surgery and other surgeries that require cardiopulmonary bypass by using a heart-lung machine. CONSERVING BLOOD DURING CARDIAC SURGERY AT HUNTINGTON UNIVERSITY HOSPITAL (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez May 7, 2016 4 authority in the operating room. “I have no direct control over any of the nursing staff,” Young explained. “But, there is recognition of a certain hierarchy in terms of who ultimately controls the trajectory of patient care.” Nevertheless, in the case of heart surgeries, certain key decisions about a patient’s care could be made without immediately notifying the surgeon. In a non-emergency, various members of the medical team, including nurses, could make the decision on whether a patient should receive a blood transfusion. The cardiac surgeon did not need to be notified before his or her patient received a transfusion, a practice that took Young by surprise. In his previous job, it was mandatory that the surgeon be notified before his or her patient had a blood transfusion.
- 15. The Blood Conservation Project In December 2013, Young, who was known for his dual interests in improving outcomes and lowering costs, and intention of enrolling in an MBA program, was asked to sit on the Center for Cardiac Medicine’s newly constituted Committee for Operational Excellence (COE). The 20-person committee, co-headed by a cardiologist and a heart surgeon, was comprised of hospital administrators and medical staff, and physicians from the medical school. One of its main goals, as explained in a press bulletin that was sent out to HUH staff, was to bolster the hospital’s reputation by making the Center for Cardiac Medicine a world-class destination populated with multidisciplinary teams of top rated clinicians and educators. Part of the committee’s work involved exploring various growth strategies for HUH and finding ways to improve quality outcomes while bringing down costs. The hospital was looking for $80 million in savings. The Affordable Care Act of 2010’s Hospital Value- Based Purchasing Program rewarded acute care hospitals with incentive payments for the quality of care they provided to Medicare patients, how closely best clinical practices were followed, and how well hospitals enhanced patients’ experiences of care during hospital stays.6 By the same token, hospitals that veered in the opposite direction, for example those that had excessive 30-day readmission rates, were penalized.7 Pay-for- performance was replacing fee-for-service. As one HUH director explained, hospitals were being challenged with getting medical providers to “move in a
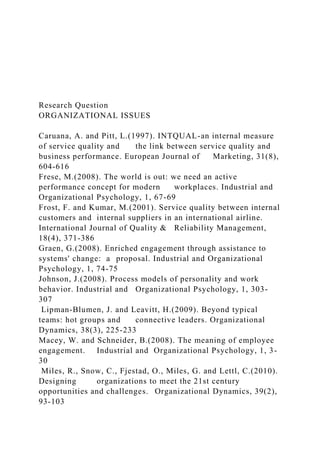
- 16. direction that’s productive not only for their patients but for the institution.” Young was nominated to chair COE’s cost and value- positioning sub-committee, which was charged with looking at quality outcomes in relation to costs. One surprising statistic the committee unearthed was that 51% of the patients that came through the Center for Cardiac Medicine had some sort of bleeding-related complication and, of those, most had come through the Center’s operating room where the number of blood transfusions taking place for AVR and CABG averaged 65% in 2013.8 (See Figure 1.) 6 http://www.cms.gov/Outreach-and-Education/Medicare- Learning-Network- MLN/MLNProducts/Downloads/Hospital_VBPurchasing_Fact_S heet_ICN907664.pdf, accessed June 22, 2015. 7 http://www.naemt.org/docs/default-source/ems-health-and- safety-documents/article_valuebasedpurchasing.pdf?sfvrsn=2, accessed June 22, 2015. 8 Between 2011 and 2013, 71% of the 500 patients who had an AVR or CABG at HUH received a blood transfusion: 69% in 2011, 79% in 2012, and 65% in 2013. CONSERVING BLOOD DURING CARDIAC SURGERY AT HUNTINGTON UNIVERSITY HOSPITAL (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez May 7, 2016 5
- 17. Figure 1 Blood Product Usage, Intra-and Post Operative Participant 12219 Like Group 2013 STS 2013 2011 2012 2013 Intraop/Postop Products Used 69.7% 78.8% 64.5% 52.3% 48.2% Total Number of Blood Product Units 1 Red Blood Cell Unit 13.5% 13.2% 14.6% 13.2% 9.5% 2 Red Blood Cell Units 20.2% 20.8% 13.8% 12.1% 13.5% 3 Red Blood Cell Units 9.6% 11.5% 6.9% 7.1% 6.2% 4+ Red Blood Cell Units 18.3% 23.6% 14.3% 14.0% 13.1% 1+ Fresh Frozen Plasma Units 27.9% 42.4% 31.5% 15.1% 13.9% 1+ Cryoprecipitate Units 1.4% 3.1% 2.6% 5.5% 4.9% 1+ Platelet Units 37.5% 56.3% 42.1% 22.1% 20.5%
- 18. Missing 0.0% 0.0% 0.0% 0.0% 0.1% Like Group = Large, academic, tertiary care medical centers STS = Society of Thoracic Surgeons Compared to similar-sized academic teaching hospitals offering AVR and CABG, HUH spent several million dollars more on blood products during cardiac surgery. Meanwhile, the total direct costs associated with bleeding-related complications for HUH was nearly $8 million in 2013, of which cardiac surgery accounted for nearly half. From a value-based purchasing perspective, Young knew the practice was not sustainable and he believed there were several quick techniques that medical teams could employ to bring down the use of blood products, assuming his colleagues would be willing to comply. In addition to ensuring that there was no bleeding from the heart before the chest cavity was closed, autologous blood harvest and retrograde autologous priming were two blood conservation techniques Young knew about and had practiced. See Figure 2 for descriptions of each. Figure 2 Autologous Blood Harvest and Retrograde Autologous Priming Autologous blood harvest drew off a pre-determined volume of blood from the patient and was stored in the OR with the goal of returning it to the patient immediately at the conclusion of surgery. The advantage of using the patient’s own blood was that its clotting elements would not have been degraded by exposure to the heart-lung machine.
- 19. Retrograde autologous priming, or RAP, removed saline fluid, which could amount to as many as two liters of fluid, from the heart-lung machine and replaced it with the patient’s own blood. Doing so prevented the profound dilutional effect when saline solution mixed in with the patient’s circulating blood, often leading to a falling blood count. Source: Dr. Frank Young. CONSERVING BLOOD DURING CARDIAC SURGERY AT HUNTINGTON UNIVERSITY HOSPITAL (A) Abeel A. Mangi, Cate Reavis, and Roberto Fernandez May 7, 2016 6 In most organizations like HUH, the chief of cardiac surgery would likely lead a project that sought to change cardiac-related operating procedures. However, HUH’s Chief Medical Officer asked Young, who had impressed him with his enthusiasm, the respect his peers had for his clinical capabilities, and the work he was doing on the OLC to lead the blood conservation project. Supporters and Skeptics Fortunately for Young, there were many obvious supporters of the project. One of his most important supporters was Anil Gupta, a cardiac anesthesiologist and intensivist who joined HUH in 2003 and became director of the Center for Cardiac Medicine’s cardiothoracic ICU unit in 2010. For some time, Gupta had been concerned about the amount of blood
- 20. products being used in the peri-operative period, in the OR and in the ICU, and had raised the issue with colleagues before Young joined HUH. “I thought we were misusing these products,” he said. “A blood product is considered a medication.” Approximately, 40% of blood transfusions took place in the ICU. Young’s support network also included hospital administrators, nurses, perfusion staff, cardiologists, and a couple of Young’s surgical colleagues. As Gupta noted, “People were actually hungry to see something new happening and to see that we wanted to change the way medicine had been practiced in our area for the past two or three decades. They understood that it was truly the best thing for patients.” The skeptics of the blood conservation project included several veteran heart surgeons who didn’t understand why they needed to change their ways, eliciting intial reactions like, “Why are we bothering to do this? We’ve been doing it this way for 20 years and we haven’t had any problems.” Young elaborated on their reaction: “The way most cardiac surgeons function is every operation has a certain rhythm to it. People don’t want to be disrupted from their usual routine. Even the imposition of a couple of minutes can seem like an eternity to people who are not accustomed to it,” especially, he added, since surgeons had historically been compensated for the number of surgeries performed, and had practiced medicine with little incentive to think about cost implications. One of the administrative staff who Young spoke to about the
- 21. project told him that he supported the effort and then said, “I wish you luck,” which Young took to mean the culture of the organization was such that there were far easier cost saving efforts to take on. Conclusion As Young studied the latest numbers for blood product usage in the OR and ICU, he knew that HUH’s Center for Cardiac Medicine’s surgical teams could do better and had to do better. As the appointed leader of the Blood Conservation Project which would require changing the behavior of a number of his colleagues, Young had to decide where to start, who to involve, and when, and how to explain the problem so that the skeptics would become full-on supporters. Finally, he had to ensure that the changes stuck. American University of Kuwait College of Business and Economics HR 205 – Human Resources Management Group Project-Case study Spring Semester 2018 Format: Poster L. O.s Covered by this Assessment: SLO 1- Become familiar with human resource (HR) management techniques used in work organizations; SLO 2- Be able to evaluate the effectiveness of HR management techniques. SLO 3- Practice applying HR management techniques with cases. SLO 4- Develop problem-solving and communication skills
- 22. needed for effective HR management. % of Final Grade: 15% Total Marks Available: 100 Students’ names: ____________________________________________ Students’ IDs: Section #: HR 205 / 100 Academic Integrity Policy : See the college’s Student Code of Conduct in catalogue. Task Based on the Sloan Business School Case Study “Conserving Blood During Cardiac Surgery at Huntington University Hospital (A)” written byAbeel A. Mangi, Cate Reavis, and Roberto Fernandez Please do a thorough reading of the case and answer the following questions relevant to it. Your answers should be
- 23. written on the Power Point Poster document that was emailed to you. You can also include graphs or images/pictures based on the way you answering. There are no optional questions so make sure that you answer all of them before you submit your group project. The deadline is Tuesday 8 of May, 2018 from 2:00 pm to 3:30 pm, Office A-418. Please answer the following questions: · What was the problem that HUH Hospital was facing? (Brief description) · Identify four groups of stakeholders relevant to the problem. Briefly describe the reasoning of choosing them as stakeholders. · What kind of project the hospital decided to implement and what was the goal of it? · What were the two major restraining factors that Dr. Young needs to consider seriously on the change he was about to initiate in HUH? (Explain) · What were the main weaknesses/potential improvement points relevant to organizational structure identified by Dr. Young? · What was the major issue revealed from the Sceptics group and why was important for the whole project?(Explain) · Dr. Young had to decide where to start, who to involve, and when, and how to explain the problem so that the Skeptics would become full-on Supporters. If you were a business consultant what would you recommend to him (you can include any HRM practice or tool you think appropriate) on these important issues that can actually define the success of the project?
- 24. Page 2 of 2