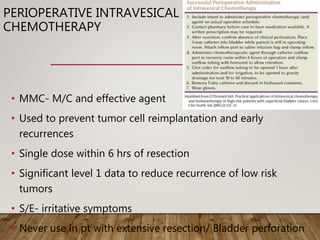
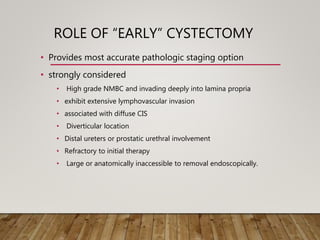
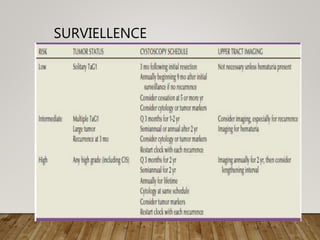
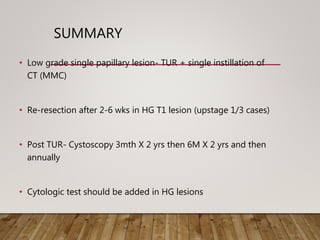
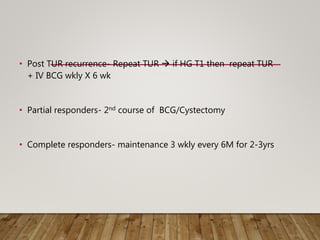
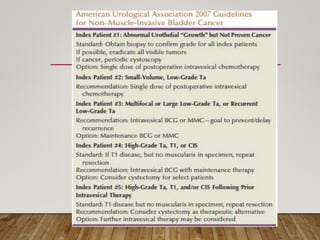
Non-muscle invasive bladder cancer is the most common type of bladder cancer. It is typically treated with transurethral resection of the bladder tumor followed by a single dose of intravesical chemotherapy within 6 hours to prevent reimplantation of tumor cells. For high risk non-muscle invasive bladder cancer, such as carcinoma in situ, multiple tumors, or high grade tumors, intravesical immunotherapy with bacillus Calmette-Guerin is recommended following resection. Early cystectomy may be considered for refractory high grade disease that does not respond to initial treatment. Long term surveillance cystoscopy is important for monitoring recurrence and progression.























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















