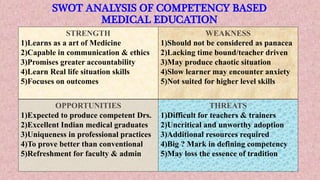
The document presents an overview of Competency-Based Medical Education (CBME) by Dr. Pradeep Kumar Dewangan, detailing its rationale, components, teaching methods, and assessment strategies. CBME focuses on developing competencies required for patient care, emphasizing learner-centered approaches and continuous assessment while addressing challenges in implementation. The document also includes a SWOT analysis and discusses the future of CBME in the context of Indian medical education.

















![AETCOM [ATTITUDE,ETHICS & COMMUNICATION IN MEDICAL EDUCATION] EDUCATION](https://cdn.slidesharecdn.com/ss_thumbnails/aetconnewpppt-200525080043-thumbnail.jpg?width=640&height=640&fit=bounds)






















































