More Related Content
Similar to Cardiovascular agents
Similar to Cardiovascular agents (12)
Cardiovascular agents
- 1. Cardiovascular agents
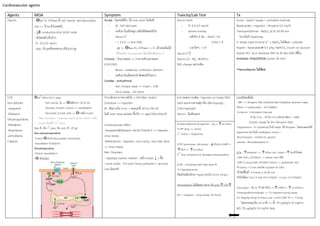
Agents MOA Symptom Toxicity/Lab Test Tx
Digoxin - ƟNa+
-K+
ATPase ที่ Cell memb. ของ Myocardial
cell => ↑กน.หัวใจหดตัว
- ↓ē conduction ผ่าน SA,AV node
- ขับไตหลัก/ตับบ้าง
-TI : 0.5-2.0 ng/ml
- abp. เร็ว,ฤทธิ์ตรงต่อกน.หัวใจ,Vd สูง
Acute : ไม่เคยได้รับ, ได้ over dose ในทันที
- GI : N/V abd pain
- ระดับยาในเลือดสูง แต่ไม่มีพิษต่อหัวใจ
- Serum K+
- < 5-5.5 => ตาย 50%
- สูง => ƟNa+-K+ ATPase => K+
เข้าเซลล์ไม่ได้
*ใช้ร่วมกับ furosemide ได้แต่ต้องติดตาม K+
Chronic : กินมาตลอด => ร่างกายขับออกลดลง
(CHF,CKD)
- Neuro : weakness, confusion, delirium
- ระดับยาในเลือดปกติ พิษต่อหัวใจมาก
Cardiac : arrhythmia
- Ven. Ectopic beat => V.tach , V.fib
- Sinus brady. , AV block
Serum level
- TI: 0.5-2.0 ng/ml
- Severe toxicity
- หลังกิน 6 ชม. : Adult >10
Child > 4
- เวลาใดๆ : >15
Serum K+
↑
Serum Ca+
, Mg+
, BUN/Scr
EKG change เพราะพิษ
Acute : Gastric lavage + activated charcoal
Bradycardia + Hypoten : Atropine 0.5 mg IV
Trachyarrhythmia : MgSO4 2g IV 20-30 min
*ยกเว้นมี Hypermag.
V. etopic beat (normal K+
+ MgSO4 ไม่ได้ผล) : Lidocain
Hyperk : Kayexalate® 0.5 g/kg, NaHCO3, insulin w/ glucose
Hypok: KCL 5g in Drextose 500 ml IV drip (EKG ดีขึ้น)
Antidote: (Fab)/DSFab (onset 20 min)
*Hemodialysis ไม่ได้ผล
CCB
Non-dihydro
-verapamil
-Diltiazem
Dihydropyridines
-Nifedipine
-Nicardipine
-amlodipine
(-dipine)
Ɵca
2+
influx ทาง L-type
- Cell memb. ใจ => Ɵไฟฟ้าจาก SA ไป AV
- Vascular smooth muscle => vasodilation
- Pancreatic ß (islet cell) => Ɵก.หลั่ง insulin
*Met. Disorders : Hypergly+lactic acido. เพราะ ก.หลั่ง
insulin ต้องใช้ Ca
2+
influx
Abp ดี, เกิด 1
st
pass, จับ prot. ดี , VD สูง
Non-duhydropyridine
-Potent ƟSA,AV,Myocardial contractility
-Vasodilator (ปานกลาง)
Dihydropyridine
-Potent vasodilation
-Ɵ หัวใจน้อย
Pt.มาด้วยอาการทางหัวใจ + DM (Met. Acido)
Overdose => Hypoten.
IR : พิษภายใน 6 hrs + หมดฤทธิ์ 24 hrs (SR x2)
ไม่มี toxic dose แน่นอน ขึ้นกับ => age,CVD,ยาร่วม,SR
Cardiovascular effect
-Verapamil&Diltiazem :ขยาย//ปานกลาง => Hypoten ,
sinus brady.
-Nifedd,amlo : Hypoten, sinus tachy, very high dose
=> sinus brady.
Met. Disorders
- Hypergly (severe marker) : หลั่ง insulin ↓ + ดื้อ
-Lactic acido : จาก poor tissue perfusion + glucose
met ผิดปกติ
อาการเด่นภาวะพิษ : Hypoten w/ brady (EKG
บอก) แยกจากสาเหตุยาอื่น (BB>Hypogly ,
CCB>Hypergly)
Serum : ยืนยันเฉยๆ
1.การรักษาทั่วไป
- ABC => Atropine ก่อน endotracheal intubation (prevent vagal
reflex => bradycardia = อาการแย่ลง)
-GI decon: 1.Activated charcoal
IR ใน 2 hrs , SR ใน 4 hrs (ต่อ24-48hrs + WBI)
2.Gastric lavage ใน 2hrs (Atropine ก่อน)
-Hypotension : IV crystalloid ถ้ามี brady. ให้ Atropine ไม่ตอบสนองให้
dopamine (ยกเว้นมี cardiogenic shock )
-Brochospasm : inhaled ß2 agonist
-seizure : Benzodiazepine IV
2.Ca : ↑extracell => ↑influx via L-type=>↑กน.หัวใจหด
-10% CaCl2 (10-20ml) -> central vein หรือ
-10% Ca gluconate (30-60ml bolus) => peripheral vein
*IV bolus > 5 min (จะเกิด Hypoten & V.fib)
*ถ้าไม่ดีขึ้นซ้้า 3-4 dose q 10-20 min
*ยังไม่ได้ผล Cacl2 IV drip 0.4 ml/kg/hr , Ca glu 1.2 ml/kg/hr
3.Glucagon : จับ ß1 ที่ MB หัวใจ =>↑cAMP=> ↑ca influx=>
+inotropic&chronotropic => Tx Hypoten+symp brady
LD: 50µg/kg (3mg) IV bolus over 1-2min (BW 70 => 3-5mg)
ไม่ตอบสนองใน 10 นาที => ซ้้า 70 µg/kg/hr (5 mg/hr)
MD: 70 µg/kg/hr (5 mg/hr) drip
4.Catecholamine (ß-agonist) : +ß1=>↑ca influx
Tx BP drop => shock
1
st
choice = Dopamine
5.PDI (amrinone, milrinone) : ↓ท้าลาย cAMP=>
↑PKA => ↑ca influx
2
nd
line combined w/ glucagons/Isoprenaline
6.HIE : combined with high dose RI
Tx Hyperglycemia
ใช้แล้วไม่ต้องรักษา Hypok (ยกเว้น K<2.5 mEq/L)
Hemodialysis ไม่ได้ผล!!!! เพราะ จับ prot.↑+VD↑
ICU = hypoten , symp brady, AV block
- 2. Agents MOA Symptom Toxicity/Lab Test Tx
BB
-propranolol
-metoprolol
-atenolol
-timolol
-labetalol
-esmolol
แย่ง E&NE จับ R => Ɵß1=>ขาด cMP=>↓ca2+
influx
Abp เร็ว , onset 20 min , peak 1-2hrs
1.MSA : overdose => Quinidine like effect, QRS กว้าง
*Propra MSA สูงสุด => coma, ชัก, hypoten, brady, AV
& QRS ผิดปกติ
2.Lipid solubility : met ที่ตับมาก , VD สูง , เข้าและแพร่
CNS เร็ว
3.ISA & ß1 selectivity : ยาที่มีคณสบ.นี้จะปลอดภัย
1.Cardiovascular effect
-Hypoten w/ brady (ยกเว้น propra จะ BP ปกติ)
-Hyperten , trachy ในยาที่มี ISA (pindolol)
-EKG => prolong PR/QT, AV block, ST/T เปลี่ยน
2.CNS effect *** ต่างจาก CCBs (propra, meto พบมาก)
-Drowsiness
-Seizure
-Coma
-ไม่นิยมตรวจระดับยาในเลือด
-EKG: Heart block, arrthmias
ที่ต่างจาก CCBs ที่เหลือเหมือนหมด
Hypoten : Pt.ที่ได้ BB w/ MSA overdose และมี QRS กว้าง/ V.
dysrhythmias => NaHCO3 1-2 mEq/kg IV
PDI : ให้ใช้หลังจาก Glucagon แล้วไม่ได้ผล (CCB จะให้ร่วมกันเลย)
ICU = เพิ่ม CHF , severe mental, coma, seizure
เฟิร์น : antiarrthymic สรุปเองแหน่จ้า .. งง TT