
Recommended
More Related Content
What's hot
What's hot (20)
Similar to EP10: An Unusual Case of Lung Collapse in a patient with Arteriovenous Fistula
Similar to EP10: An Unusual Case of Lung Collapse in a patient with Arteriovenous Fistula (20)
Recently uploaded
Recently uploaded (20)
EP10: An Unusual Case of Lung Collapse in a patient with Arteriovenous Fistula
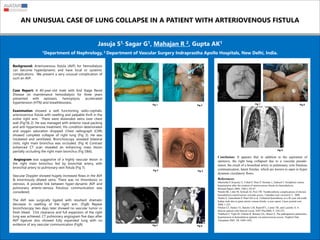
- 1. AN UNUSUAL CASE OF LUNG COLLAPSE IN A PATIENT WITH ARTERIOVENOUS FISTULA Jasuja S1, Sagar G1, Mahajan R 2, Gupta AK1 1Department of Nephrology, 2 Department of Vascular Surgery Indraprastha Apollo Hospitals, New Delhi, India. Background: Arteriovenous fistula (AVF) for hemodialysis can become hyperdynamic and have local or systemic complications. We present a very unusual complication of such an AVF. Case Report: A 40-year-old male with End Stage Renal Disease on maintenance hemodialysis for three years presented with epistaxis, hemoptysis, accelerated hypertension (HTN) and breathlessness. Examination showed a well functioning radio-cephalic arteriovenous fistula with swelling and palpable thrill in the entire right arm. There were distended veins over chest wall (Fig1& 2). He was managed with anterior nasal packing and anti-hypertensive treatment. His condition deteriorated and oxygen saturation dropped. Chest radiograph (CXR) showed complete collapse of right lung (Fig 3). He was intubated and ventilated. Bronchoscopy revealed bilateral clots; right main bronchus was occluded. (Fig 4) Contrast enhanced CT scan revealed an enhancing mass lesion partially occluding the right main bronchus (Fig 5&6). Angiogram was suggestive of a highly vascular lesion in the right main bronchus fed by bronchial artery, with bronchial artery to pulmonary vein fistula (Fig 7). Vascular Doppler showed hugely increased flows in the AVF & enormously dilated veins. There was no thrombosis or stenosis. A possible link between hyper-dynamic AVF and pulmonary arterio-venous fistulous communication was considered. The AVF was surgically ligated with resultant dramatic decrease in swelling of the right arm. (Fig8) Repeat bronchoscopy two days later showed no vascular tumor or fresh bleed. Clot clearance and full expansion of the right lung was achieved. CT pulmonary angiogram five days after AVF ligature also showed fully expanded lung with no evidence of any vascular communication (Fig9). Conclusion: It appears that in addition to the aspiration of epistaxis, the right lung collapsed due to a vascular pseudo- tumor, the result of a bronchial artery to pulmonary vein fistulous communication, latent fistulas, which are known to open in hyper dynamic circulatory flows. Fig 1 References: •Bachelda P, Kojecky Z, Utikal P, Drac P, Herman J, Zadrazil J. Peripheral venous hypertension after the creation of arteriovenous fistula for hemodialysis. Biomed.Papers 2004, 148(1), 85-87 •Smith SR, Little M, Schwab SJ, Post TW. Nonthrombotic complications of chronic hemodialysis arteriovenous vascular access. Uptodate.com version16.3, 2008 •Salim S, Ganeshram P, Patel AD et al. Unilateral hemothorax in a 46 year old south Indian male due to giant arterio venous fistula: a case report. Cases journal.com 2008, 1:225 •Diskin CJ, Stokes TJ, Dansby LM, Radcliff L, Carter TB, and Lazenby A. A dialysis patient with blurred vision. NDT Plus2008; 4: 250-252. •Nakhoul F, Yigla M, Gilman R, Reisner SA, Abassi Z, The pathogenesis pulmonary hypertension in hemodialysis patients via arteriovenous access. Nephrol Dial Transplant 2005; 20; 1686-1692. Fig 2 Fig 3 Fig 4 Fig 5 Fig 6 Fig 7 Fig 8 Fig 9