
Recommended
More Related Content
What's hot
What's hot (20)
Similar to steroidal sex hormones
Similar to steroidal sex hormones (20)
Recently uploaded
Recently uploaded (20)
steroidal sex hormones
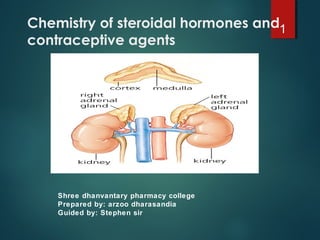
- 1. Chemistry of steroidal hormones and contraceptive agents Shree dhanvantary pharmacy college Prepared by: arzoo dharasandia Guided by: Stephen sir 1
- 2. Adrenocortical Hormones Adrenal gland: Medulla: produces Epinephrine (stimulated by sympathetic impulse) Cortex: Zona glomerulosa – produces Aldosterone (stimulated by Angiotensin II and ACTH) Zona fasciculata – produces Glucocorticoids (stimulated by ACTH = Corticotropin) Zona reticularis – produces Androgens 2
- 3. Adrenocortical Hormones Glucocorticoids (GC): Inhibit all phases of inflammatory reaction Promote fetal development (lungs) Unregulate lipocortin => inhibits PLA2 => no PG and LT synthesis Undesirable effects of increased GC: Immune suppression Increased glucose release (=> “steroid diabetes”) Glucose coverted to fat => adiposity Increased protein catabolism => muscle atrophy Salt and water retention (increased GC lead to reduction in ACTH => decreases levels of aldosterone) => hypertension Osteoporosis 3
- 4. Adrenocortical Hormones Glucocorticoids (GC): Hydrocortison (= Cortisol) Main glucocortocoid in humans Also binds mineralocorticoid receptor (Cortison does NOT) Used for replacement therapy (Addison’s Disease) 4
- 5. Topical Hydrocortisone Hydrocortisone is a topical steroid. It reduces the actions of chemicals in the body that cause inflammation, redness, and swelling. Hydrocortisone topical is used to treat inflammation of the skin caused by a number of conditions such as allergic reactions, eczema, or psoriasis. Hydrocortisone topical may also be used for other purposes .it do not give any antibacterial activity. 5
- 6. Hydrocortisone oral Hydrocortisone is also used to treat low hydrocortisone levels caused by diseases of the adrenal gland (such as Addison's disease, adrenocortical insufficiency). Corticosteroids are needed in many ways for the body to function well. They are important for salt and water balance and keeping blood pressure normal. 6
- 7. Female sex hormone and hormonal drugs 7
- 8. Hormones involved in ovulation process Gonadotropin Releasing Hormone (GnRH) = Gonadoliberin stimulates release of Follicle stimulating hormone (FSH) = Follitropin and Luteinising Hormone (LH) = Lutropin which trigger production of Estrogens (E) and Gestagens (G) which in turn negatively regulate Pituitary (E+G) and Hypothalamus (G) hormone production 8
- 9. How estrogen and progesterone are produced and involved in female reproductive cycle Cycle length varies from 21-35 days Menstruation 3-6 days First (= Proliferative) phase: Variable (7-21 days) FSH and LH promote follicle development One follicle becomes the Graafian follicle (the rest degenerate) Graaffian Follicle: Consists of thecal and granulosa cells which surround the ovum FSH-stimulated granulosa cells produce estrogens from androgen precursors generated by LH-stimulated thecal cells Estrogens are responsible for the proliferative phase: increase in thickness and vascularity of endometrium; secretion of protein+ carbo-rich mucus Constant low estrogen inhibits LH/FSH production BUT high estrogen cause surge of LH production => swelling and rupture of Graafian follicle = Ovulation 9
- 10. Sex Steroids Female reproductive cycle Second (= Secretory) phase: Secretory phase constant (~ 14 days) LH-stimulated ruptured follicle develops into Corpus luteum which secrets Progesterone Progesterone (Pg) is responsible for the secretory phase: endometrium becomes suitable for implantation; mucus thickens Thermogenic effects of Pg => body temperature increase 0.5º C Without implantation: Pg secretion stops => menstruation is triggered With implantation: continued Pg production which (via inhibition of LH and FSH prod.) blocks further ovulation Chorion (“precursor” of placenta) secretes human chorionic gonadotropin (HCG) which maintains endometrium lining throughout pregnancy (HCG -> see pregnancy test) 10
- 11. Sex Steroids 11
- 12. ESTROGENS All produced from androgen precursors Three main endogenous estrogens: Estradiol Primary estrogen in humans Breast development Improving bone density Growth of the uterus Accelerating bone maturation Development of the endometrium to support pregnancy Promoting vaginal mucosal thickness and secretions Increase HDL Estrone 1/3 active than estradiol Estriol only during pregnancy (made by fetus) 12
- 13. NATURAL ESTROGENS 13 HO OH OH HO O HO OH 17β-estradiol Estrone Estriol
- 14. Sar of estrogens 14 Aromatic ring with C-3-OH is essential for activity. Steroidal structures is not essential for activity. The intensity of activity changesif route of administration changes, e.g.,for oral route: Estriol > estradiol > estrone. For subcutaneous route: estradiol > estrone > estriol. Alkylation of the aromatic ring decrease the activity. The 17β-hydroxyl with constant distance from 3-OH is essential for activity. The group between the two hydroxyl must be hydrophobic. Unsaturation of ring B decreases the activity. 17α- and 16 position when modified enhance the activity. Example: mestranol.
- 16. Estradiol: Estradiol is rapidaly oxidized in the liver to form estrone, which is ineffective. Ethinyl estradiol: 15- 20 more potent than estradiol orally. Adding a 17β-ethiny to estradiol blocks this oxidation and makes the compound orally active. 16
- 17. Synthetic or non-steroidal estrogens Diethylstilbesterol: The trans form is the active one. Advantages: As active as Estradiol. Longer duration of action. Orally active Cheap. Disadvantages: Increase the risk of uterine cancer. Uses: Treatment of prostate cancer. 17 OH HO
- 18. ESTROGEN ANTAGONISTS Tamoxifen Antiestrogenic effects on mammary tissue Weak estrogenic effects on bone and lipid metabolism Clomiphene Inhibits estrogen binding in the pituitary => prevention of negative feedback=> ovulation Clinical uses of anti-estrogens: Breast cancer therapy (Tamoxifen) Infertility (Clomiphen) 18
- 19. progesterone Progesterone Inhibits rhythmic contractions of the myometrium Not suitable for oral administration (rapid hepatic elimination) => stable derivatives: Hydroxyprogesterone Medroxyprogesterone 19
- 20. Sar of progesterone Steroidal nucleus essential for activity. Have some androgenic activity. Removal of the 19 CH3 increase activity. Unsaturation of ring B or C increase the activity.e.g., megestrole acetate. Removal of the keto function remove androgenic activity. 20
- 21. progesterone Semisynthetic progestine with pure progesterone activity Norethindrone Norgestrel 21 O O Progesterone (Natural) OH Lynesrenol (Synthetic) C CH
- 23. Male sex hormones Gonadotropin Releasing Hormone (GnRH) = Gonadoliberin stimulates release of Follicle stimulating hormone (FSH) (Stimulates Sertoli cells => promotes gametogenesis) and Luteinising Hormone (LH) = Interstitial Cell Stimulating Hormone (ICSH) which triggers production of Testosterone (T) (by Leydig cells) which in turn negatively regulates Pituitary and Hypothalamus hormone production 23
- 24. SAR 24
- 26. androgens Testosterone Primary androgen in humans Possesses androgenic and anabolic effects: Androgenic effects: Growth and development of male sex organs Important for (male) sex drive and performance Development of secondary sexual characteristics Important role in spermatogenesis Anabolic effects: Development of muscle mass Reverse catabolic or tissue-depleting processes Dihydro-Testosterone Active metabolite Mediates most of testosterone actions CH3 OH O CH3 CH3 OH O CH3 H 26
- 27. androgens Testosterone Hepatic elimination after oral administration Also short half-life after injection => ester derivatives: Proprionate, enanthate, cypionate… Fluoxymesterone Hepatic elimination after oral administration CH3 OH O CH3 OH F CH3 CH3 OH O CH3 R 27
- 28. Anabolic androgens Testosterone derivatives: anabolic effects dominant Nandrolone Injection Stanozolol oral administration CH3 OH O CH3 H OH O CH3 CH3 OH N CH3 CH3 NH H 28
- 29. Anti androgens Flutamide Non-steroidal receptor antagonist Used in prostate cancer treatment Finasteride Inhibits 5α-reductase => prevent conversion of testosterone into the more potent dihydrotestosterone (DHT) Used to treat prostate gland enlargement and hair loss (bald man have higher average levels of DHT) NH CF3 O CH3 NO2 CH3 CH3 CH3 N H O O N H CH3 CH3 CH3 H 29
- 30. 30