Downloaded 1,027 times







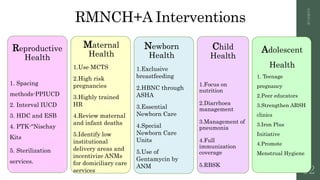

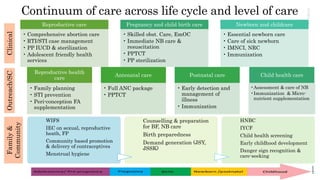


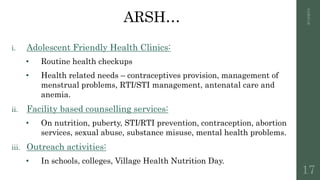



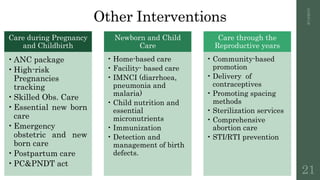



The document outlines India's strategic approach to reproductive, maternal, newborn, child, and adolescent health (RMNCH+A), initiated in 2013, aimed at reducing infant and maternal mortality rates, and improving overall health outcomes. It details specific interventions, coverage targets, and management tools directed towards underserved populations, particularly in high priority districts. The strategy emphasizes a continuum of care, linking community and facility-based services while focusing on key issues such as adolescent health, nutrition, and maternal care.













































































