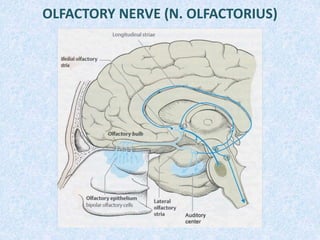
2. EXAMINATION OF THE OLFACTORY NERVE
To the patient give to smell
various odorous substances
by the each nostril (mint
drops, camphor oil, tincture
valerian, etc.). In this case it is
necessary to avoid sharp
odorous substances.
3. AFFECTION OF THE OLFACTORY TRACT
Dysfunction of sense of smell: more often observed as
reduction (hyposmia) which is accompanied by decrease of the
gustatory sense and decrease of the appetite or total loss smell
(anosmia). Affection of the olfactory bulb and tract with one
side is accompanied homolateral by loss of sense of the smell.
These dysfunction can be caused by tumors of the anterior
cranial fossa, the fracture of the skull base, the basal
arachnoiditis, the diseases mucous a nose (a rhinitis, polyps,
etc.).
In some cases the observed of sense of the smell - hyperosmia
(pregnancy), dysosmia (a perversion of sense of smell). The
irritation of a temporal lobe in region hippocamp leads of the
olfactory hallucinations or auras.
4. OPTIC NERVE (N. OPTICUS)
1st neuron – rods and cones
of the retina
2nd neuron – bipolar cells of
the retina
3rd neuron – ganglion cells
of the retina
4th neuron – lateral
geniculate body
5th neuron – thalamus
6th neuron - calcarine sulcus
and lingual gyrus
5. EXAMINATION OF THE OPTIC NERVE
Visual acuity (visus) is investigated with the
help of the special of the Sivtsev’s table on
which are represented a letters and a picture
on the decreasing size. Each eye is
investigated represent. In norm visual acuity
is equal to unit (1.0). Decrease in visual
acuity name to amblyopia, full loss –
amaurosis (blindness).
Colour sensation investigate with the help
of the color pictures and the figures. Examine
ability to distinguish colors and their shades.
The full color blindness to achromatopsia,
and the disturbances of the perception of the
individual colors - dyschromatopsia among
which daltonism - inability is most distributed
to distinguish green and red colors.
6. EXAMINATION OF THE OPTIC NERVE
(CONTINUATION)
The field of vision are investigated with the
help of Goldmann’s perimeter or with the
help of the percussion hammer. The
constriction of a field of vision from different
directions name concentric, prolapse of his
separate parts - scotoma, prolapse of the
half field of vision - hemianopsia.
8. EXAMINATION OF THE OPTIC NERVE
(CONTINUATION)
Examination of fundus of eye.
In normal the disk of optic nerve
white reddish color, accurate
confines. Position of vascular in the
central of optic disk and contour of
optic dist regular. The correlation
arteries to veins are two to three.
9. AFFECTION OF THE OPTIC NERVE
• At affection of a retina or optic nerve arises either blindness or decrease in
visual acuity, concentric narrowing of a field of vision. At affection of separate
fibres appear scotoma, on the party of the lesion focus. At the blindness
connected to affection of optic nerve, disappear reaction of a pupil to light,
since drops out afferent a part of the iris contraction reflex disappears, and
consensual reaction of a pupil remains.
• At localization of the lesion focus in area optic chiasm are observed
heteronymous hemianopsia which depend on a place of affection optic chiasm.
If the lesion focus is located in a medial part, there where occurs decussation
medial fibres of the optic tract, that drop out external half field of vision
(bitemporal hemianopsia). So is observed at tumours of a hypophysis. Affection
lateral parts of the optic chiasm result to drop out of internal half field of vision
(binasal hemianopsia).
10. AFFECTION OF THE OPTIC NERVE
(CONTINUATION)
• At affection of the optic tract after optic chiasm arise homonymous
hemianopsia. At affection of the optic tract - homonymous hemianopsia, at
affection of the Gratsiole's bundle - quadrantic hemianopsia. In such cases
research iris contraction reflex matters.
• The irritation of the visual cortex result to sensation of flicker before eyes of
luminous points (photopsy). But can arise and more complex visual
sensations: subjects seem increased (macropsia), or reduced (micropsia), or
deformed (metamorphopsia). Also visual hallucinations are observed.
16. EXAMINATION OF OCULOMOTOR NERVES
• palpebral fissures
• form and size of pupils
• mobility of eyeballs
• reaction of pupils on the light
• convergence and accommodation
17. EXAMINATION OF OCULOMOTOR NERVES
(CONTINUATION)
In norm pupils are identical, have correct, roundish form, not jag
edges. The difference of pupils in size is called anisocoria.
Check reaction of pupils on the light - their constriction at
illumination and dilation at darkening. For this purpose turn the
patient to a light source and suggest fixing a look at the remote point.
Close both eyes with palms, thus the pupils dilatation occur. Then
quickly take away one hand and observe a straight reaction to the
light. For research of consensual reactions cover one eye with a palm
and watch the consensual expansion of the other pupil. Then quickly
take away a palm and watch dilatation of both pupils.
Reaction of pupils on the light
direct consensual
18. EXAMINATION OF OCULOMOTOR NERVES
(CONTINUATION)
Examining the convergence suggest a patient to look at
forthcoming to a nose percussion hammer. At that the convergence
of eye balls takes place and concurrently constriction of pupils
accommodation.
Examining the mobility of eyeballs suggest a patient to watch at an
object moving at different directions.
19. AFFECTION OF OCULOMOTOR NERVES
Symptoms of affection of 3rd pair
divergent strabismus (it happens
due to "pulling" of an eye
outwards and downwards by
healthy muscles)
a doubling at a
sight directly
(diplopia)
exophthalmos (of an eyeball
from an orbit, due to atonia of
an eye muscles and prevalence
of a tone of smooth muscles of
an eye)
ptosis(a paralysis of m.
levator palpebrae)
the affection of nucleus of
Yakubovich and Perlia
causes the dilatation of a
pupil (mydriasis)
at disorder of
accommodation and
weakening of a reaction
of a pupil on the light
20. AFFECTION OF OCULOMOTOR NERVES
(CONTINUATION)
diplopia at a look aside
Symptoms of affection of 4th pair
impossibility to rotate
an eyeball to down and
to side
converging strabismus diplopia at a sight
down
Symptoms of affection of 6th pair
impossibility to rotate
an eyeball outwards
21. AFFECTION OF OCULOMOTOR NERVES
(CONTINUATION)
Disorder of a pupil reaction on light causes the Ardzhil – Robertson syndrome
a direct syndrome - loss of a straight
consensual reactions of a pupil to
light at preservation of convergence
and accommodation (can be met at
tabes dorsales)
a reverse syndrome - preservation of a
straight and consensual reactions of a
pupil to light at loss of convergence
and accommodation (can be met at
epidemic encephalitis)
Ophthalmoplegia
at affection of all
oculomotor nerves
develops total
ophthalmoplegia
at affection of external
muscles - external
ophthalmoplegia
at loss of function of
internal muscles of an eye
- internal ophthalmoplegia
22. TRIGEMINAL NERVE (N. TRIGEMINUS)
N. ophthalmicus – superior orbital
fissure - supraorbital notch
(incisure)
N. maxillaries – round foramen -
infraorbital canal
N. mandibullaris – oval foramen -
mental foramen
24. INNERVATIONS OF THE FACE
• N. ophthalmicus (upper floor) is innervate skin of forehead,
anterior hair part of head, superior eyelid, internal corner of
eye, dorsum of nose, mucous membrane of frontal and ethmoid
sinuses, periosteum, upper one third of face
• N. maxillaris (middle floor) is innervate skin of inferior
eyelid, external corner of eye, upper parts of cheeks, upper lip,
upper jaw and its teeth, mucous membrane of nasal cavity,
maxillary sinus
• N. mandibularis (lower floor) is innervate lower lip, lower
part of cheeks, lower jaw and its teeth, chin, lateral part of face,
mucous membrane of cheeks
25. EXAMINATION OF TRIGEMINAL NERVE
• check the chewing muscles (survey and palpate
temporal and chewing muscles, suggest a patient to
clench his teeth, open a mouth, to move the lower jaw
to the sides)
• exanimate of corneal reflex
• superficial and deep sensitivity of the face (Zelder's
zones and sensitivity of the three departments)
• revealing of painful points
26. AFFECTION OF TRIGEMINAL NERVE
• Affection of the one of branches - leads to disorder of all types of
sensitivity in peripheral type in a zone of innervations of the definite branch,
occurrence of pains, decrease or fading of corresponding reflexes (1 branch -
supraorbital, corneal and conjunctival reflexes, the 3rd branch - a mandibullar
reflex)
• Affection of the trigeminal ganglion is accompanied by disorders of all
types of sensitivity in a zone of all three branches, occurrence of pain, herpes
zoster at the face
• Affection in the field of the pons cerebri leads to dissociative disorders of
sensitivity, total affection of a nucleus sensitivity leads to the loss of
sensitivity on the half of a face on segmentary type, at partial affection of a
nucleus leads to the loss of sensitivity in certain Zelder's zones
• Affection of thalamus and a back third of the back leg of an internal
capsule - causes contralateral loss of sensitivity of the face and trunk
• At a neuralgia of a trigeminal nerve paroxismal pains in a zone of
innervation are observed
29. EXAMINATION OF FACIAL NERVE
First of all pay attention to the patient's face - to the
symmetry of the relief of the wrinkles on the forehead, equal
slant of palpebral fissures, note the differenes in the
nasolabial folders, the presence of the watering on the one
side, suggest a patient knit his brow; wrinkle up forehead, to
shut each eye by turns and both eyes together, to wrinkle a
nose, to grin, inflate cheeks, to whistle.
30. AFFECTION OF FACIAL NERVE
Symptoms of affection of facial nerve:
• xerophthalmus (dryness of eye) or watering
• hyperacusia (increased perception of sounds)
• agesia (loss of taste on front two thirds of tongue)
• facial asymmetry on side of focus
• smoothing of nasolabial and frontal folders
• lagophthalmos (hare's eye) – eye is opened and at closing it is
turned to up and to ectad, iris is left under superior eyelid
• palpebral fissure is kept open (Bell's symptom)
• eyelash sign – at close eyes tight eyes eyelashes are kept visible
• immobility of angle of mouth on affected side
• symptom of racket - at grin of teeth the form of mouth is
changed
• patient can not whistle
• hyporeflexia of corneal reflex
37. NUCLEUS OF IX AND X CN
Common nucleus:
Nucl. solitarius - gustatory nucleus
Nucl. alae cinereae - sensitive nucleus (sensitivity of larynx,
trachea, gullet, soft palate, middle ear)
Nucl. ambiguus - motor nucleus (muscles of gullet, larynx,
epiglottis, soft palate)
Different nucleus:
IX CN - nucl. salivatorius inferior (salivation)
X CN – nucl. dorsalis vagi (parasympathetic innervations of internal
organs )
38. EXAMINATION OF GLOSSOPHARYNGEAL NERVE
The taste test of perception of four basic flavoring irritants is
checked - sweet, sour, bitter, salty. For this purpose a drop of a
specified irritant placed on the limited site of mucous membrane
on the fore-part of the tongue, which is innervated with the facial
nerve, and then - on its back third. Also compared gustatory sense
on the left and right half of the tongue. Before dropping another
solution, the mouth should be carefully rinsed with water.
Then, investigated the pharyngeal reflex and a reflex from the
soft palate, note the disposition of the uvula at the central line (ask
the patient to open a mouth and to pronounce a sound "а"),
function of swallowing and an inflection of a voice.
39. EXAMINATION OF VAGUS NERVE
The attention is paid to a tone of a voice, the disposition of the
uvula and the soft palate in oral region, take an interest if the
patient chokes at taking meal, if the food fall out through the
nose, check pharyngeal and palate reflexes, pulse, the blood
pressure, frequency of breath.
41. AFFECTION OF GLOSSOPHARYNGEAL
NERVES
• Disorders of taste on a back third of the tongue as decrease in
taste (hypogeisia), losses of taste (ageisia), increase of taste
(hypergeisia). Flavouring hallucinations appear at irritation of
the gustatory area at cortex
• Dry mouth, due to the denervation of the parotid gland
• Anesthesia of the gullet and weakening of reflexes
(pharyngeal and palate) on the affected side
• The paralysis of the soft palate on the affected side
• Deviations of the uvula to the healthy side
• Choke at swallowing, the food gets into the nasopharynx and
a nose (disfagia)
• The speech acquires nasal tone of a voice (disfonia)
42. AFFECTION OF VAGUS NERVES
• Disorders of the taste perception on back walls.
• Anesthesia of the gullet, throats, tracheas on the affected
side.
• Weakening or loss pharyngeal and palate reflexes on the
affected side.
• The unilateral paralysis of the soft palate, choke at
swallowing, sagging of a voice sheaf at laryngoscoping,
hoarseness of a voice with a nasal tone (dysphagia,
dysphonia).
• Changes of the cardiac activity (a bradycardia or
tachycardia), breath (bradipnoe or tahipnoe), disorders of
activity gastrointestinal path.
44. EXAMINATION OF ACCESSORY NERVE
Inspect and palpate sternocleidomastoideus and trapezius
muscles and check their strength. Suggest patient to make
rotations of a head to the sides, to shrug shoulders, to lift hands
above a horizontal level.
AFFECTION OF ACCESSORY NERVES
The paralysis of innervated muscles on the affected side,
complication of rotation of the head to the healthy side, the
shoulder on the struck side is descended, the shoulder-blade
placed aside from a spine, shrugging with shoulders is
complicated, range of motions of arms is limited.
46. EXAMINATION OF HYPOGLOSSAL NERVE
Note the disposition of the tongue at central line, the surface
of the tongue, presence of fibrillar and fascicular twitchings,
the patient's speech.
47. AFFECTION OF HYPOGLOSSAL NERVES
Peripheral paralysis is characterized by
paresis or a paralysis of corresponding
half of the tongue, an atrophy of
muscles, at hanging out the tongue
deviates to the paralyzed side, fibrillar
twitchings are met.
At the central paralysis the
tongue deviates to the healthy
side, thus there are no atrophies
and fibrillations.
Also at affection of a nerve speech is broken. It becomes indistinct, braided
(dysarthria). The slight dysarthria is easily revealed at pronouncing hardly
articulated words. At bilateral affection of a nerve the tongue's motionless
(glossoplegia) and speech is getting impediment (anarthria), chewing and
swallowing is broken.
49. REFLEXES OF ORAL AUTOMATISM
Distant-oral reflex - is characterized by reduction
of lip and mental muscles at approach of an
object towards the patient's face.
Palm-chin reflex (Marinesku –
Radovichi’s reflex) - at strokes of
a palm observed reductions of
muscles of a chin.
Lip reflex - at percussion at an
upper lip protrusion of lips is
appeared.
Nasolabial reflex - percussion at the
nose bridge causes drawing of lips
forward.