HYPOSPADIAS
•Download as PPTX, PDF•
40 likes•3,673 views

The document discusses hypospadias, which is an abnormal opening of the urethra on the ventral side of the penis. It provides details on the embryology, anatomy, causes, investigations and surgical techniques for repairing hypospadias. Common techniques mentioned include MAGPI, TIP, dorsal onlay graft and two-stage repair. The goal of surgery is to create a straight penis with the urethral meatus at the tip of the glans penis and provide symmetrical skin coverage.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to HYPOSPADIAS
Similar to HYPOSPADIAS (20)
Recently uploaded
Recently uploaded (20)
HYPOSPADIAS
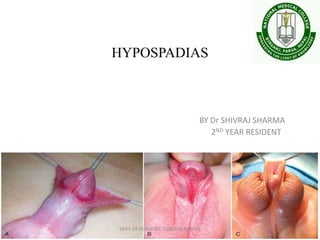
- 1. HYPOSPADIAS BY Dr SHIVRAJ SHARMA 2ND YEAR RESIDENT DEPT OF PEDIATRIC SURGERY,NMCTH
- 2. • Definition : An abnormal ventral opening of urethral meatus located anywhere from the ventral aspect of glans penis to perineum. • Due to arrested penile development • always associated with An abnormal ventral curvature of penis (chordee) An abnormal distribution of foreskin with a hood present dorsally and deficient foreskin ventrally DEPT OF PEDIATRIC SURGERY,NMCTH
- 3. Embryology Two embryonic structures play an important part in the development of urogenital system: • Intermediate mesoderm • Cloaca Cloaca has two parts separated by urorectal septum: • Dorsal: primitive rectum • Ventral: primitive urogenital sinus (UGS) DEPT OF PEDIATRIC SURGERY,NMCTH
- 4. DEPT OF PEDIATRIC SURGERY,NMCTH
- 5. DEPT OF PEDIATRIC SURGERY,NMCTH
- 6. Primitive urogenital sinus : 2 parts Cranial : vesico uretheral part Caudal : definative urogenital sinus At the junction of these lies the opening of mesonephric duct Definitive urogenital sinus : 2 parts Cranial : pelvic Caudal : phallic DEPT OF PEDIATRIC SURGERY,NMCTH
- 7. Development of male external genitalia • With formation of urorectal septum, coacal memb divides into urogenital memb and caudal anal memb • Urogenital memb elongates longitudinally • On its both sides, mesoderm heaps up to form 2 longitudinal elevations called primitive urethral folds, and 3 other elevations: genital tubercle, rt. & lt. genital swellings • Genital tubercle becomes cylindrical and enlarges greatly to form penis • By epithelial ingrowth, glans is formed and then coronal sulcus appears • Prepuce is formed by the reduplication of ectoderm, covering the distal part of phallus DEPT OF PEDIATRIC SURGERY,NMCTH
- 8. Development of urethra DEPT OF PEDIATRIC SURGERY,NMCTH
- 9. Development of urethra DEPT OF PEDIATRIC SURGERY,NMCTH
- 10. • Proposed by Glenister in 1954 • Urogenital memb lies in a linear groove • On its either sides are primitive urethral folds • Groove elongates with the phallus and extends on its undersurface, lined by ectoderm Called primitve urethral groove (PUG) • At 10 mm stage, (4th week) thickening of anterior wall of endodermal cloaca • Solid mass of endodermal cells derived from the UGS extends into the phallus Called urethral plate • PUG is now fully formed . Urethral plate has now enlarged and extends deeper in the phallus DEPT OF PEDIATRIC SURGERY,NMCTH
- 11. • Urogenital memb has broken down so that endoderm of caudal part of UGS is seen from outside • Degeneration of core cells of urethral plate leads to deeper groove k/a definitive urethral groove. Its margins are k/a definitive urethral folds • At 11th week, 50 mm stage, Leydig cells of testis increase in no., size, and function and under the effect of androgens the definitive urethral folds grow towards each other and fuse to form a median raphe • In this way DUG is converted into a tube which is urethra DEPT OF PEDIATRIC SURGERY,NMCTH
- 12. • A pre-requisite of urethral fold fusion is the canalisation of the solid urethral plate • formation of urethral groove bounded on each sides by the urethral folds • If any of the above is abnormal, urethral fold fusion is likely to be impaired. • The fusion starts caudally and progresses cranially • This extends only upto glans penis. DEPT OF PEDIATRIC SURGERY,NMCTH
- 13. • The elongating phallus is covered externally by the ectoderm that gives rise to te penile skin • Most of the penis is derived from the mesodermal cells forming the corporal bodies,connnective tissue and dermis • Corporal tissue is first recognised as distinct dense mesenchymal condensations within the shaft of the developing penis. DEPT OF PEDIATRIC SURGERY,NMCTH
- 14. • At 40 mm stage, preputial tissue did not uniformly surround the phallus in the form of a circle but in the form of an oblique orientation, radiating out on either side of phallus from the point of urethral opening • The urethral opening is placed well back on the ventral surface of the phallus • Preputial tissue appears as a hood dorsally and gradually become less well marked ventrally as it approaches the meatus • Complete covering of the glans occurs at 130 mmm stage or 20th week of development DEPT OF PEDIATRIC SURGERY,NMCTH
- 15. Anatomy of penis Five layers of tissue cover the penis: • Penile skin • Superficial layer of penile fascia (Dartos fascia) • Tela subfascialis • Deep layer of penile fascia (BUCK’S fascia) • Tunica albuginea Two Ligaments • Superficial fundiform ligament • Suspensary ligament proper DEPT OF PEDIATRIC SURGERY,NMCTH
- 16. Penile skin Properties • Movable • Expandable • Adaptable to urinary contact Advantageous for urethral tube reconstruction b/c it is: • Available • Vascular • Distensible DEPT OF PEDIATRIC SURGERY,NMCTH
- 17. Penis : arterial and venous supply DEPT OF PEDIATRIC SURGERY,NMCTH
- 18. DEPT OF PEDIATRIC SURGERY,NMCTH
- 19. • Incidence: 1: 300 males • Risk is 13 fold in 1st degree relatives • 8% patients have father with hypospadias, 14% have male siblings with hypospadias • Risk of hypospadias in next child, when one child is affected with hypospadias: • 12% with negative family history • 19% if cousin or uncle has hypospadias • 26% if father or sibling has hypospadias • 8.5 times more risk in monozygotic twins DEPT OF PEDIATRIC SURGERY,NMCTH
- 20. Other risk factors: • Placental dysfunction • Low birth weight • Preterm birth • Pre-pregnancy maternal obesity • Extremes of maternal age ( <24 and >40) • Assistive Reproductive techniques DEPT OF PEDIATRIC SURGERY,NMCTH
- 21. ASSOCIATED ANOMALIES • Undescended testes- 9% • Inguinal hernias- 9% • Upper urinary tract anomalies 1-3% • Utriculus masculinus- Incomplete mullerian duct regression • Cryptorchidism- intersexuality needs to be ruled out especially in cases of non palpable testis DEPT OF PEDIATRIC SURGERY,NMCTH
- 22. Clinical findings • c/o difficulty directing the urinary stream and stream spraying • Chordee • Perineal or penoscrotal hypospadiasis necessitates voiding in sitting position • Proximal forms of hypospadiasis results in infertility in adults • Abnormal hooded apperance of penis • Associated undescended testicles DEPT OF PEDIATRIC SURGERY,NMCTH
- 23. Investigations • Diagnosis is clinical . • Imaging is not required in cases of isolated hypospasdias, regardless of surgery • In penoscrotal and perneal hypospadias , pt often present with bifid scrotum and ambiguous genitalia : buccal smear and karyotyping are indicated to help establish genetic sex. • urethroscopy and cystoscopy will aid in evaluating development of internal reproductive organs. DEPT OF PEDIATRIC SURGERY,NMCTH
- 24. Treatment HISTORICAL DESCRIPTION DEPT OF PEDIATRIC SURGERY,NMCTH • Carl thiersch,1869 and Duplay 1880 described use of buried skin tube as neo urethra • Sir Denis Browne 1950, popularised this procedure ,still used as two stage procedure BURIED SKIN TUBE • Ombredanne 1932,suggested making circular flap with hypospadic meatus at its centre Perimeata l flaps • Nove Josserand 1897 and later Mcindoe : produce urethra by an inlay free graft of penile tunnel • Devine and Hortan elaborated technique Inlay free graft
- 25. • Bucknall , formation of tube fom penile and scrotal skin and burying the penis1907 • Broadbent 1951 used full thickness oblique strip of skin from prepuce and penile skin Single stage operation • Byars ; first successful two stage repair • First stage : chordee correction and redistribution of dorsal penile skin onto ventrum • Second stage : neourethra formed using ventral penile skin Two stage repair DEPT OF PEDIATRIC SURGERY,NMCTH
- 26. Present day concept of hypospadias repair Goal : to produce a straight penis and the external urinary meatus at the tip of conicl glans To provide symmetrical skin cover with minimal ,short and long term compication The procedure is preferably performed in one stage as a day case and at the young age. Earlier till 60s, it was generally argued that cosmetic considerations are secondary and are more concern of the parents of child and chordee corrected by staged procedure 18 months onwards before school going is ideal time • DEPT OF PEDIATRIC SURGERY,NMCTH
- 27. Common operative techniques MAGPI ( Meatal Advancement and Glanuloplasty) Tubularised incised urethral plate Dorsal free graft Inlay Onlay transverse preputial skin patch Two stage repair DEPT OF PEDIATRIC SURGERY,NMCTH
- 28. Meatal Advancement And Glanuloplasty (MAGPI) • IDEAL patient : glanular hupospadias with a flat or convex glans and thick and healthy skin proximal to meatus without chordee • It can be contemplated in pts with coronal hypospadias without or with very mild chordee which can be corrected by dorsal plication or in pts who have retrussive meatus after previous surgery. • Should be avoided in pts with subcoronal or more proximal hypospadias with wide meatus or concave or grooved glans with considerable chordee DEPT OF PEDIATRIC SURGERY,NMCTH
- 29. DEPT OF PEDIATRIC SURGERY,NMCTH
- 30. • A circumcoronal icision is given and chordee is excluded by artificial erection. • A vertical incision is given in dorsal plate of glans distal to meatus and the glanular plate is mobilised starting from the meatus to the proposed site at tip. • Vertical incision closed by two or three transverse sutures of 6/0 absorbable. • Glans is carefully undermined on both sides of distal urethra between tunica and glans tissue after dividing fanned out spongiosa to expose the tunica underneath. DEPT OF PEDIATRIC SURGERY,NMCTH
- 31. • The dissection in the midline must be careful and fairly superficial so as to avoid injury to underlying urethra • Glans wings are approximated by two or three vicryl 6/0 sutures after excising redundant free margin with compromising the lumen of urethra • Skin cover is provided after excising the redundant skin andgiving oblique cut dorsally if required • Skin sutures by 6/0 chromic catgut,preferably subcuticular • 6fr catheter is introduced and light pressure dressing applied. DEPT OF PEDIATRIC SURGERY,NMCTH
- 32. Tubularised Incised Urethral Plate (TIP) :SNODGRASS • Best suited for pts of distal penile hypospadias with a wide concave (wide groove) ,wide meatus, healthy thick urethral plate ,healthy skin/mucosa ventrally proximal to meatus and without chordee. • Can be done in pts having minimal chordee , corrected by dorsal plication • Avoided in those with more proximal hypospadias with flat glans ,narrow urethral plate , moderate chordee and when skin proximal to thin and attenuated. DEPT OF PEDIATRIC SURGERY,NMCTH
- 33. DEPT OF PEDIATRIC SURGERY,NMCTH
- 34. • Penis is degloved by a circumcoronal incision incorporating meatus. • Absence of chordee assesed by artificial eerection • Urethral plate is incised dorsally in midline from meatus to tip of glans penis • Glans wings are raised on either side of urethral plate upto midglans level only • Tubularisation on a catheter is performed by a continous suture of 6/0 chroic catgut • Redundant and thinned out margins of penile skin are excised and dorsal oblique cut is given on outer preputial skin • Skin closure ad catheter is secured. DEPT OF PEDIATRIC SURGERY,NMCTH
- 35. A DORSAL FREE GRAFT ON INCISED URETHRAL PLATE • Pts with distal penile hypospadias with a flat glans and a narow but healthy urethral plate • Meatus narrow or wide ,with no chordee • Also performed for those with proximal hypospadias with above criteria and minimal chordee. • Procedure similar to Snodgrass except that after incising the urethral plate , two half of the plate are mobilised partially from underneath the tunica and anchored to tunica. • The raw are between two halves of urethral plate is coered with an inlay dorsal free graft. DEPT OF PEDIATRIC SURGERY,NMCTH
- 36. Onlay transverse preputial skin patch • Can be applied to pts who have narrow urethral plate from distal penile meatus to proximal penile meatus and with attenuated ventral skin. • Glans may be flat or convex and there is no chordee DEPT OF PEDIATRIC SURGERY,NMCTH
- 37. The two stage repair of hypospadias • The two stage repair is suitable for patients with marked chordee and meatus suited far proximally. • Also suitable if there is no or adequate prepuce or if there is preference of the surgeon. • FIRST STAGE A circumcoronal incision ,circumscribing the external urethral opening is applied leaving 5 to 6mm corona Degloving is done and chordee correction is done. Glans is laid open and glans wings are raised. The dorsal penile skin is incised in the midline upto an appropriate level o as to cover the degloved penis with care while not injuring the superficial dorsal vessels. DEPT OF PEDIATRIC SURGERY,NMCTH
- 38. • Suturing is started from the tip of the laid open glans to the meatus proximally proximally by 6/0 chromic catgut and the two edges of the covering skin lying in midline. SECOND STAGE usually done after 6 months Assessment is made for width of laid open glans ,the quality of the ventral penile skin, the meatal area for stenosis or for any hair bearing area. After assesment ,a 14f catheter is passed. Two parrallel incisions are given on ventral penile skin, circumscribing the meatus upto midglans . The width of ventral penile skin should ideally be equal to the calibre of 14F catheter. DEPT OF PEDIATRIC SURGERY,NMCTH
- 39. Leaving ventral penile skin strip intact ,the rest of the covering penile skin is mobilised after leaving a cuff of 4 to 5 mm corona and degloving is done. Byars cut is now given on dorsal penile skin in such a way that the covering skin suture line will fall eccentrically. a tube is made of the ventral penile strip by 6/0 subcuticular chromic catgut sutures. Skin suturing is provided in two layers ,inner subcuticular by 5/0 chromic and outer skin to skin 5/0 chromic . DEPT OF PEDIATRIC SURGERY,NMCTH
- 40. DEPT OF PEDIATRIC SURGERY,NMCTH
- 41. DEPT OF PEDIATRIC SURGERY,NMCTH
- 42. DEPT OF PEDIATRIC SURGERY,NMCTH
Editor's Notes
- Supf fundiform: Thickening of scarpa fascia, originating at linea alba,splits to surround the base of penis and joins Colles’ fascia Suspensory liagament proper: beneath the fundiform ligament, attaches to symphysis pubis, maintains penile position during coitus