
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Salivary glnds ppt
Similar to Salivary glnds ppt (20)
Recently uploaded
Recently uploaded (20)
Salivary glnds ppt
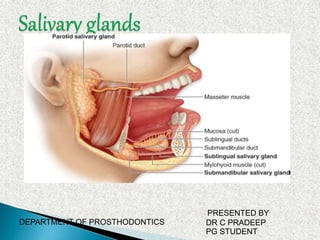
- 1. DEPARTMENT OF PROSTHODONTICS PRESENTED BY DR C PRADEEP PG STUDENT
- 2. Contents Introduction classification Development of Salivary Glands Anatomy Parotid gland Submandibular gland Sublingual gland Minor salivary gland CLINICAL CONSIDERATION PROSTHODONTIC IMPLICATIONS References
- 3. Introduction Salivary glands are compound, tubuloacinar exocrine glands whose ducts open into the oral cavity. They secrete saliva, a fluid which Lubricates food to assist deglutition, Moistens the buccal mucosa, which is important for speech, and Provides an aqueous solvent necessary for taste. Contains digestive enzymes, e.g. salivary amylase Antimicrobial agents e.g. IgA, lysozyme etc
- 4. .Based on size Based on type of secretory cells
- 5. 1. Major salivary glands 2. Minor salivary glands 1. Major salivary glands Collection of secretory cells aggregated into large bilaterally paired extra oral glands with extended duct system through which the gland secretions reach the mouth. - Parotid - Submandibular - Sublingual
- 6. Collection of secretory cells scattered throughout the mucosa & submucosa of the oral cavity with short ducts opening directly onto mucosal surface. - Serous glands of Von Ebner. - Anterior lingual glands. - Lingual, buccal, labial, palatal glands, glossopalatine and retromolar glands
- 7. 1. Serous : Parotid 2. Mixed (seromucous): Submandibular 3. Mucous: Minor salivary glands.
- 8. Development of Salivary Gland During the fetal life each salivary gland is formed at specific location in the oral cavity The submandibular and sublingual develop in the floor of the stomodeum.
- 9. Individual salivary glands arise as a proliferation of oral epithelial cells, forming a focal thickening that grows into underlying ectomesenchyme. Continued growth results in formation of a small bud connected to the surface by a trailing cord condensing around the bud.
- 10. Lumen formation may involve apoptosis of centrally located cells in the cell cord. Following development of lumen in terminal buds, the epithelium consists of two layers of cells. Inner layer Cells of inner layer differentiate into secretory cells of mature glands. Outer layer (Some cells) form the contractile myoepithelial cells that are present around the secretory end pieces & intercalated duct.
- 11. Connective tissue Salivary gland has connective tissue component that diminishes as parenchyma expands; Even so every terminal end piece and every duct remain supported by tenuous connective tissue component carrying blood vessels and nerves. (The presence of functional innervations is also essential to proper growth & maintenance of salivary glands structure.)
- 12. Post natal growth The glands continue to grow postnatally with the volume proportion of acinar tissue increasing up to2 yr of age. The volume proportion of ducts, connective tissue and vascular elements decreasing up to 2 yr of age.
- 14. Ductal system of a salivary gland: Main excretory duct opens into the oral cavity. Excretory ducts are mostly located in the interlobular connective tissue. Striated ducts are the main intralobular ductal component. Intercalated ducts vary in length and connect the secretory end pieces with the striated ducts. Intercellular canaliculi are extensions of the lumen of the end piece between adjacent secretory cells that serve to increase the luminal surface area available for secretion.
- 16. The paired parotid glands are the largest of the salivary glands. The gland is an irregular, lobulated, yellowish mass, lying largely below the external acoustic meatus between the mandible and sternocleidomastoid muscle.
- 17. The gland also projects forwards on the surface of masseter. In 20% of cases, a small, usually detached, part called the accessory parotid gland lies between the zygomatic arch above and the parotid duct below.
- 18. From medial to the lateral side these are: Arteries: External carotid artery Maxillary artery Superficial temporal vessel Posterior auricular artery Veins: Retromandibular vein Facial nerve
- 19. Maxillary artery leaves the gland through its anteromedial surface. Superficial temporal vessel: emerge at the anterior part of the superior surface Posterior auricular artery may arise within the gland.
- 20. Veins : The Retromandibular vein is formed within the gland by the union of superficial temporal and maxillary veins.
- 21. Nerves: Facial nerve enters the gland through the upper part of its posteromedial surface. The nerve divides into its terminal branches within the gland.
- 22. Parotid duct The parotid duct begins by the confluence of two main tributaries within the anterior part of the gland. It appears at the anterior border of the upper part of the gland and passes horizontally across masseter, approximately at the level midway between the angle of the mouth and the zygomatic arch.
- 23. While crossing masseter it can receive the accessory parotid duct and lies between the upper and lower buccal branches of the facial nerve. The duct is 5 cm long and its lumen is 3 mm wide.
- 24. The arterial supply to the parotid gland is from the external carotid artery and its branches within and near the gland. The veins drain to the external jugular vein via local tributaries.
- 25. Lymph nodes are found both in the skin overlying the parotid gland (preauricular nodes) and in the substance of the parotid gland itself. There are usually 10 lymph nodes present in the gland. The majority are found in the superficial part of the gland lying above the plane related to the facial nerve.
- 26. The deeper part of the parotid gland beneath the branches of the facial nerve contains one or two lymph nodes. Lymph from the parotid gland drains to the upper deep cervical lymph nodes.
- 27. Parasympathetic nerves(secretomotor) Inferior salivatory nucleus Glossophyrengal nerve.(tympanic branch) Tympanic plexus Lesser petrosal nerve Otic ganglion Auriculotemporal nerve Parotid gland
- 28. Sympathetic nerve supply: Vasomotor -Derived from the plexus around the external carotid artery Sensory nerve supply: Auriculotemporal nerve
- 29. Because of fibrous fascia is covering the parotid, its inflammatory swelling is tense and hard. Parotid duct is slightly larger along their course than at their caruncle. This permits storage of secretions so that a ready flow may be available on stimulation without waiting for secretory process.
- 30. The submandibular gland is irregular in shape and about the size of a walnut. It consists of a larger superficial and a smaller deep part, continuous with each other around the posterior border of mylohyoid. It is a seromucous (but predominantly serous) gland.
- 31. 2nd largest salivary gland • Shape & size – roughly J shaped & about the size of a walnut • Weight – 8 to 10gm each • Location – posterior part of the floor of the mouth, tucked up against the medial aspect of the body of mandible • Secretory duct – Wharton’s duct -
- 32. The arteries supplying the gland are branches of the facial and lingual arteries. The lymph vessels drain into the deep cervical group of lymph nodes (particularly the jugulo-omohyoid node), interrupted by the submandibular nodes.
- 34. Also known as Wharton's duct. The submandibular duct is 5 cm long and has a thinner wall than the parotid duct. It begins from numerous tributaries in the superficial part of the gland and emerges from the medial surface of this part of the gland behind the posterior border of mylohyoid. It traverses the deep part of the gland, passes at first up and slightly back for 5 mm, and then forwards between mylohyoid and hyoglossus.
- 35. It next passes between the sublingual gland and genioglossus to open in the floor of the mouth on the summit of the sublingual papilla at the side of the frenulum of the tongue. It lies between the lingual and hypoglossal nerves on hyoglossus, but, at the anterior border of the muscle, it is crossed laterally by the lingual nerve, terminal branches of which ascend on its medial side. As the duct traverses the deep part of the gland it receives small tributaries draining this part of the gland.
- 36. The secretomotor supply Superior salivatory nucleus Facial nerve Chorda tympani Submandibular ganglion Postganglionic parasympathetic fiber supplying gland.
- 37. Sensory nerve supply: Lingual nerve Vasomotor nerve supply: Plexus around the facial artery
- 38. The arteries supplying the gland are branches of the facial and lingual arteries. The veins drain into the common facial or lingual vein. The lymph vessels drain into the deep cervical group of lymph nodes (particularly the jugulo-omohyoid node), interrupted by the submandibular nodes.
- 39. The entire submandibular gland and duct system lies in a dependent position, which predisposes it to retrograde invasion by oral flora. Similar to the parotid duct, the Wharton’s duct is also wider before reaching the papilla. This can lead to stangulation of saliva and the organic matter. The sharp bends of Wharton’s duct at the posterior border of the mylohyoid muscle allows stasis of the saliva favoring the formation of salivary stones.
- 40. The sublingual gland is the smallest of the main salivary glands: each gland is narrow, flat, shaped like an almond, and weighs 4 g. The sublingual gland lies on mylohyoid, and is covered by the mucosa of the floor of the mouth, which is raised as a sublingual fold. The anterior end of the contralateral sublingual gland lies in front, and the deep part of the submandibular gland lies behind.
- 41. The mandible above the anterior part of the mylohyoid line, the sublingual fossa, is lateral, and genioglossus is medial, separated from the gland by the lingual nerve and submandibular duct. The sublingual glands are seromucous, but predominantly mucous.
- 42. The arterial supply is from the sublingual branch of the lingual artery and the submental branch of the facial artery. Lymphatic drainage is to the submental nodes.
- 43. The sublingual gland has 8-20 excretory ducts. Smaller sublingual ducts open, usually separately, from the posterior part of the gland onto the summit of the sublingual fold (a few sometimes open into the submandibular duct). Small rami from the anterior part of the gland sometimes form a major sublingual duct (Bartholin's duct), which opens with, or near to, the orifice of the submandibular duct. This duct may be visualized occasionally in a submandibular sialogram.
- 44. Minor salivary glands are found throughout the oral cavity, except in the anterior part of the hard palate & the gingiva. The minor salivary glands of the mouth include: Labial , Buccal , Palatoglossal , Palatal Lingual glands. The labial and buccal glands contain both mucous and serous elements. The palatoglossal glands are mucous glands and are located around the pharyngeal isthmus.
- 45. LABIAL / BUCCAL GLANDS • Gland on lips and cheeks. • Mixed type GLOSSOPALATINE GLANDS • Principally localized in the region of isthmus in glossopalatine fold. • Pure mucous gland
- 46. The palatal glands are mucous glands and occur in both the soft and hard palates. The anterior and posterior lingual glands are mainly mucous. The anterior glands are embedded within muscle near the ventral surface of the tongue and open by means of four or five ducts near the lingual frenum and the posterior glands are located in the root of the tongue.
- 47. The sublingual gland and the minor salivary glands have short ducts, where the chances of stasis are less. Thus, obstructive lesions do not occur in the glands. Since minor salivary glands are placed superficially, the traumatic lesions such as Mucoceles commonly affect these glands.
- 48. Xerostomia: Drugs- central or peripheral inhibition of salivary secretion. Destruction of salivary gland: -Radiotherapy -Chemotherapy -Bone marrow transplant -Autoimmune diseases (sjogren’s syndrome)- invasion of lymphocytes & destruction of epithelial cells. Psychological factors Malnutrition
- 49. Refers to excess saliva production. Causes: -Gastrointestinal irritants -Drugs (Pilocarpine) -Cerebro vascular accident -Pt. with a severe neurologic deficit -Pt. who have undergone extensive oral surgical procedures.
- 50. 1.Sialolith (stones) Mostly in submandibular gland 2.Mucous plugging in minor salivary glands due to trauma. Age changes: Parenchymal cells are replaced by adipose tissue. Decreased saliva production Resting saliva(unstimulated) is in normal range, while stimulated saliva is less.
- 51. Viral( mumps) & bacterial infections- painful swelling .
- 52. Diabetes : Parotid gland swelling may occur Salivary flow is reduced. Changes in salivary proteins. Autoimmune diseases may cause destruction of salivary glands & reduced salivary flow. Sjogren’syndrome Rheumatoid arthritis Graft-verus host diseases Patients with adrenal disease may have altered electrolyte composition.
- 53. Decreased flow rates. Lower levels of immunoglobulins in saliva Parotid enlargement – lympathedenopathy and lymphoepithelial cysts Genetic diseases: Cystic fibrosis: Na+ & Cl- conc. are increased and mucous secreting glands may develop mucous plugs. Benign & malignant tumours.
- 54. • From the prosthodontists point of view, salivary glands are of great importance both anatomically and physiologically. Extension of denture base: Stenson's duct - it is rare for a maxillary denture to cause obstruction to this duct. • Wharton’s duct - extension of the lingual flange in this region can lead to obstruction – patient complains of swelling under the tongue while eating. Sublingual - it is rare for a denture to cause any significant obstruction
- 55. In complete denture • Procedures -aim at optimizing retention and stability. • Use dentures with metal bases. • Use of soft liners to improve comfort. • Use of denture adhesives to augment retention. • Frequent recall – As more prone to candida infections. • Fabrication of intra oral artificial salivary reservoirs.
- 56. Excessive salivation due to sub mandibular and sublingual gland causes difficulty in impression making of complete dentures. Administration of drugs should be done before making impression. Excessive secretion from the mucous glands in the palate region causes distortion of the impression material. To counteract this problem, the palate may be massaged to encourage the glands to empty, the mouth may be irrigated with astringent and the palate may wiped with gauze
- 57. Palatal wax removed2-mm thick modeling wax Prosthodontic Management of Xerostomic Patient: A Technical Modification Complete denture with salivary reservoir
- 58. Putty adapted over the central area to form the reservoir Lid and the denture cured separately Lid permanently Attached with autopolymerizing acrylic resin Inlet and outlet holes
- 59. Artificial saliva substitute (wet mouth, ICPA Health Products Ltd., MUMBAI, INDIA) was then used for filling the reservoir space
- 60. Various postinsertion instructions provided to the patient are: Guidelines were given to the patient with respect to oral care and denture maintenance Instructions were given to the patient regarding the cleaning of the reservoir space. The patient was schooled to clean the reservoir daily with a small brush and a fine orthodontic wire The patient was advised to flush out the reservoir with 1% sodium hypochlorite solution once a week The patient was told to fill the reservoirs 3–4 times a day with artificial saliva It was advised to drink at least eight glasses of water, lemon juice, or milk
- 61. In Removable partial denture • Anti sialagogues administered 1to 2 days before treatment. • Impression making: mouth irrigated with an astringent. • Mouth washed prior to investing impression material. • Fast setting impression material is used. • Patient’s mouth should be packed with 4x4 inch gauze that has been folded to form an absorptive strip. • “ Tandem” impression technique.
- 62. • • Failure to remove saliva from the impression will result in an inaccurate cast • Thin, serous saliva to be washed under cool tap water. If running tap water is not effective, the saliva can be removed using a soft camel hair brush and a mild detergent. • Thick, ropy saliva- a thin layer of dental stone be sprinkled the surface of the impression
- 63. When an impression is made or a restoration is cemented, great degree of dryness is required • Achieved by using- • Rubber dam, high-volume vacuum, saliva ejector, antisialagogues. Methantheline bromide (banthine) and propantheline bromide (pro-banthine).
- 64. The components of saliva act as a mirror of the body’s health. • The multi factorial role of salivary components continue to represent a focused area of dental research. • The knowledge of normal salivary composition, flow & function is extremely important on a daily basis when treating patients. • Dental health professionals spend untold hours removing this precious natural resource to perform therapy, with little regard to its value until flow is significantly reduced. • Whether saliva occurs in quantities large or small , recognition should be given to the many contributions it makes to the preservation & maintenance of oral & systemic health.
- 65. References Ten Cate’s Oral histology Development, Structure nd Function Sixth Edition General Anatomy 3rd vol. by B. D. Chaurasia Maxillary reservoir denture to overcome radiation-induced xerostomia – Light at the end of the tunnelSudhanshu Srivastava1, Preety Negi2, Devendra Chopra1, Sumit Misra Prosthodontic Management of Xerostomic Patient: A Technical Modification Haraswarupa Gurkar, Omprakash Yadahally Venkatesh, JagadeeshMandya Somashekar, Muthuraj Hariharapura Lakshme Gowda, Madhavi Dwivedi, and Ishani Ningthoujam Edgerton M, Tabak LA, Levine MJ. Saliva: A significant factor in removable prosthodontic treatment. J Prosthet Dent. 1987; 57(1): 57-66.