
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to DYSTOCIA.ppt
Similar to DYSTOCIA.ppt (20)
Recently uploaded
Recently uploaded (20)
DYSTOCIA.ppt
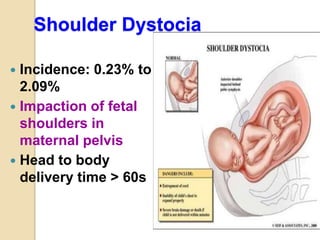
- 1. Shoulder Dystocia Incidence: 0.23% to 2.09% Impaction of fetal shoulders in maternal pelvis Head to body delivery time > 60s
- 2. Definition “…a delivery that requires additional obstetric maneuvers following failure of gentle downward traction on the fetal head to effect delivery of the shoulders.” ACOG, Practice Bulletin 40 (November 2002)
- 3. Definition “Prolonged head-to-body expulsion time” Objectively defined as 60 seconds Deliveries with head-to-body interval of > 60 seconds more commonly have higher birth weight, shoulder dystocia, and low 1 minute Apgar scores Beall et al 1998; Spong et al 1995
- 4. Functional Definition A delivery in which the shoulders do not follow the head as usual, but rather are delayed in delivering or require the use of ancillary obstetric maneuvers to effect delivery. The anterior shoulder may be impacted behind the symphysis pubis, or (less commonly) the posterior shoulder behind the sacral promontory
- 5. Dystocia is the consequence of 3 abnormalities that may exist singly or in combination 1-Abnormalities of the powers uterine contractility maternal expulsive forces 2-Abnormalities of the passage maternal boney pelvis the soft tissue of the reproductive tract 3-Abnormalities of the passenger presentation position development of the fetus size
- 6. How to assess these factors? Adequate powers contractions that -last for 60 sec -reach 20-30 mmHg of pressure -occur every 1-2 min Hypotonic contractions are responsible for 2/3 of nulliparous dystocia If powers are adequate check Passage for size & abnormal shape and check the Passenger for size & malpresentation
- 7. Aetiology 1. Large baby/ fetal macrosomia 2. Anencephaly 3. Contracted pelvis 4. Failure of the shoulder to rotate into the anterior-posterior diameter of the outlet following delivery of the head. 5. Foetal Ascitis
- 8. INTRODUCTION Definition: Dystocia is difficult labor or abnormally slow progression of labor ≥ 4 hrs of < 0.5 cm/ hr dilatation in the 1st stage ≥ 1 hr with no descent in the 2nd stage It can occur in 2 forms A-Primary dysfunctional labour B-Secondary arrest Expressions used to describe dystocia CPD, failure to progress (lack of progressive Cx dilatation or lack of fetal descent)
- 9. FETAL CONSEQUENCES Shoulder dystocia may be associated with significant fetal morbidity and even mortality. Gherman and co-workers (1998) reviewed 285 cases of shoulder dystocia and found 25 percent were associated with fetal injuries. Transient Erb or Duchenne brachial plexus palsies were the most common injury, accounting for two thirds;38 percent had clavicular fractures; and 17 percent sustained humeral fractures. There was one neonatal death, and four newborns had persistent brachial plexus injuries.
- 10. Complications A. Fetal :- 1.Birth asphyxia II. Traumatic injury 1.Fractures of Humerus or clavicle 2.Erb’s palsy Brachial plexus injuries a) Short term complication 1. Metabolic acidosis 2.Shock 3.Renal failure 4. CNS depression 5. Seizures b) Long term complication 1.Mental Retardation 2.Cerebral palsy 3.Seizures disorder 4.Speech defect
- 11. B. Maternal:- 1. Prolonged labour 2. Obstructed labour 3. Lacerations of the cervix, Vagina & perineum 4. Rupture of Uterus 5. PPH 6. Shock , death
- 12. Complications of Shoulder Dystocia Maternal ◦ Postpartum hemorrhage ◦ Rectovaginal fistula ◦ Symphyseal separation or diathesis, with or without transient femoral neuropathy ◦ Third- or fourth-degree episiotomy or tear ◦ Uterine rupture Fetal ◦ Brachial plexus palsy ◦ Clavicle fracture ◦ Fetal death ◦ Fetal hypoxia, with or without permanent neurologic damage ◦ Fracture of the humerus
- 13. MATERNAL CONSEQUENCES Postpartum hemorrhage, usually from uterine atony, but also from vaginal and cervical lacerations, is the major maternal risk
- 14. Anatomy of the Brachial Plexus Nerve roots from C5-C8 and T1 Merge into three trunks ◦ Superior (C5, C6) ◦ Middle (C7) ◦ Inferior (C8, T1) Each splits into anterior and posterior divisions
- 15. Anatomy of the Brachial Plexus The six divisions regroup into three cords ◦ Posterior – all 3 posterior trunk divisions (C5-T1) ◦ Lateral – anterior divisions of upper and middle trunks (C5-C7) ◦ Medial – continuation of lower trunk (C8, T1)
- 16. Anatomy of the Brachial Plexus
- 18. Brachial Plexus Injuries Strain or stretch Partial disruption Complete avulsion
- 19. Brachial Plexus Injuries Injury primarily to lateral trunk (C5,6, 7) leads to Erb’s palsy – adducted shoulder, extended elbow, and flexed wrist (“waiter’s tip”) Injury primarily to the medial trunk (C8, T1) leads to Klumpke’s palsy – paralyzed hand with good shoulder and elbow function
- 20. Maternal Complications Post-partum hemorrhage occurs in 11% 4th degree laceration occurs in 3-4%
- 21. Diagnosis •head recoils against perineum, ‘turtle’ sign •spontaneous restitution does not occur •failure to deliver with expulsive effort and usual gentle direction
- 22. Shoulder Dystocia-The turtle sign Mother is pushing with each contraction and the baby’s head starts to come out. However, with each push, the baby’s head comes out and then retracts back in towards the perineum. You quickly recognize this as the “turtle sign”
- 24. HELPERR Mnemonic The HELPERR mnemonic is a clinical tool that offers a structured framework for coping with shoulder dystocia. These maneuvers are designed to do one of three things: ◦ Increase the functional size of the bony pelvis through flattening of the lumbar lordosis and cephalad rotation of the symphysis (i.e., the McRoberts maneuver) ◦ Decrease the bisacromial diameter, the breadth of the shoulders, of the fetus through application of suprapubic pressure. ◦ Change the relationship of the bisacromial diameter within the bony pelvis through internal rotation maneuvers. Next Slide
- 25. H Call for Help: This refers to activating the pre-arranged protocol or requesting the appropriate personnel to respond with necessary equipment to the labor and delivery unit E Evaluate for episiotomy: Episiotomy should be considered throughout the management of shoulder dystocia but is necessary only to make more room if rotation maneuvers are required. Shoulder dystocia is a bony impaction, so episiotomy alone will not release the shoulder. Because most cases of shoulder dystocia can be relieved with the McRoberts maneuver and suprapubic pressure, many women can be spared a surgical incision. L Legs (the McRoberts maneuver): This procedure involves flexing and abducting the maternal hips, positioning the maternal thighs up onto the maternal abdomen. This position flattens the sacral promontory and results in cephalad rotation of the pubic symphysis. Nurses and family members present at the delivery can provide assistance for this maneuver. P Pressure (Suprapubic): The hand of an assistant should be placed suprapubically over the fetal anterior shoulder, applying pressure in a cardiopulmonary resuscitation style with a downward and lateral motion on the posterior aspect of the fetal shoulder. This maneuver should be attempted while continuing downward traction. H E L P E R R
- 26. E Enter maneuvers (internal rotation): These maneuvers attempt to manipulate the fetus to rotate the anterior shoulder into an oblique plane and under the maternal symphysis. 1. Rubin II At vaginal examination apply pressure as indicated. If shoulders move into the oblique diameter, attempt delivery. 2. Rubin II + Woods corkscrew maneuver If unsuccessful, add the Woods corkscrew maneuver and continue rotation in the same direction. Use both hands and apply pressure as indicated. If shoulders now move into the oblique, attempt delivery. If this is unsuccessful, continue rotation 180 degrees and deliver. 3. Reverse Woods corkscrew maneuver If the last maneuver is unsuccessful, change to reverse Woods corkscrew maneuver. Slide fingers down to back of posterior shoulder and attempt 180-degree rotation in the opposite direction. H E L P E R R
- 27. R Remove the posterior arm: Removing the posterior arm from the birth canal also shortens the bisacromial diameter, allowing the fetus to drop into the sacral hollow, freeing the impaction. The elbow then should be flexed and the forearm delivered in a sweeping motion over the fetal anterior chest wall. Grasping and pulling directly on the fetal arm may fracture the humerus. R Roll the patient: The patient rolls from her existing position to the all-fours position. Often, the shoulder will dislodge during the act of turning, so that this movement alone may be sufficient to dislodge the impaction. In addition, once the position change is completed, gravitational forces may aid in the disimpaction of the fetal shoulders. H E L P E R R
- 28. Management An experienced obstetrician, should be available on the labour ward for the second stage of labour when shoulder dystocia is anticipated. However, it is recognized that not all cases can be anticipated and therefore all birth attendants should be ready with the techniques required to facilitate delivery complicated by shoulder dystocia. Timely management of shoulder dystocia requires prompt recognition.
- 29. Immediately after recognition of shoulder dystocia, extra help should be called. In a hospital setting, this should include further assistance, an obstetrician, a pediatric resuscitation team and an anesthetist. Maternal pushing should be discouraged, as this may lead to further impaction of the shoulders, thereby exacerbating the situation. The woman should be maneuvered to bring the buttocks to the edge of the bed. How should shoulder dystocia be managed?
- 30. Episiotomy Episiotomy is not necessary for all cases. Some obstetrician have advocated that episiotomy is an essential part of the management in all cases but it does not affect the outcome of shoulder dystocia. The episiotomy does not decrease the risk of brachial plexus injury with shoulder dystocia. An episiotomy should therefore be considered but it is not mandatory.
- 31. McRoberts’ manoeuvre The McRoberts’ manoeuvre is the single most effective intervention, with reported success rates as high as 90%. It has a low rate of complication and therefore should be employed first.
- 32. The McRoberts’ manoeuvre is flexion and abduction of the maternal hips, positioning the maternal thighs on her abdomen. It straightens the lumbo-sacral angle, rotates the maternal pelvis cephalad and is associated with an increase in uterine pressure and amplitude of contractions. McRoberts’ manoeuvre
- 33. No increase in pelvic dimensions. Decrease in the angle of pelvic inclination P=0.001 Straightening of the sacrum P= 0.04% Tends to free the impacted anterior shoulder McRoberts manoeuvre: X ray pelvimetry study
- 34. Supra-pubic pressure can be employed together with Mc Roberts’ manoeuvre to improve success rates. External supra-pubic pressure is applied in a downward and lateral direction to push the posterior aspect of the anterior shoulder towards the fetal chest . It is advised that this is applied for 30 seconds. Supra-pubic pressure reduces the bi-sacromial diameter and rotates the anterior shoulder into the oblique pelvic diameter. The shoulder is then free to slip underneath the symphysis pubis with the aid of routine traction.
- 35. . Mc Roberts’ manoeuvre + Supra-pubic pressure
- 36. Advanced manoeuvres should be used if the McRoberts’ manoeuvre and suprapubic pressure fail. If these simple measures fail, then there is a choice to be made between the all-fours- position and internal manipulation. For a slim mobile woman without epidural anaesthesia and with a single attendant, the all fours- position is probably the most appropriate. For a less mobile woman with epidural anaesthesia in place and a senior obstetrician in attendance, Internal rotation manoeuvres (Woods manoeuvre ) are more appropriate.
- 37. Deliver posterior arm (Barnum Maneuver) grasp the posterior arm and sweep it across the anterior chest to deliver
- 38. . Woods manoeuvre: •The hand is placed behind the posterior shoulder of the fetus. •The shoulder is rotated progressively 180 d in a corkscrew manner so that the impacted anterior shoulder is released.
- 39. Wood's Screw maneuver First described in the literature in 1943, this procedure involves the progressive rotation of the posterior shoulder in corkscrew fashion to release the opposite impacted anterior shoulder. In its classic description, pressure is applied on the posterior shoulder's anterior surface. A variation of this -- the Rubin's maneuver -- involves pushing on the posterior surface of the posterior shoulder. In addition to the corkscrew effect, pressure on the posterior shoulder has the advantage of flexing the shoulders across the chest. This decreases the distance between the shoulders, thus decreasing the dimension that must fit out through the pelvis.
- 40. Rubin’s maneuver Apply pressure to the fetal scapula to effect rotation of the shoulders out of the vertical orientation As fetus rotates, anterior shoulder should pass under symphysis May be a good first choice for a right- handed operator when the fetal occiput is directed to the maternal left
- 41. Advanced manoeuvres should be used if the McRoberts’ manoeuvre and suprapubic pressure fail. If these simple measures fail, then there is a choice to be made between the all-fours- position and internal manipulation. For a slim mobile woman without epidural anaesthesia and with a single attendant, the all fours- position is probably the most appropriate. For a less mobile woman with epidural anaesthesia in place and a senior obstetrician in attendance, Internal rotation manoeuvres (Woods manoeuvre ) are more appropriate.
- 42. By inserting a hand into the posterior vagina and ventrally rotating the arm at the shoulder delivery over the perineum Delivery of the posterior arm.
- 43. What measures should be taken if first- and second-line manoeuvres fail? Third-line manoeuvres require careful consideration to avoid unnecessary maternal morbidity and mortality. It is difficult to recommend a time limit for the management of shoulder dystocia, as there are no conclusive data available.
- 44. What measures should be taken if first- and second-line manoeuvres fail? Third-line manoeuvres require careful consideration to avoid unnecessary maternal morbidity and mortality. It is difficult to recommend a time limit for the management of shoulder dystocia, as there are no conclusive data available.
- 45. Zavanelli manoeuvre Cephalic replacement of the head, and delivery by caesarean section has been described but success rates vary. Zavanelli manoeuvre may be most appropriate for rare bilateral shoulder dystocia, where both the shoulders impact on the pelvic inlet, anteriorly above the pubic symphysis and posteriorly on the sacral promontory.
- 46. The maternal safety of this procedure is unknown, however, and this should be borne in mind, knowing that a high proportion of fetuses have irreversible hypoxia-acidosis by this stage. Zavanelli manoeuvre
- 47. fracture the anterior clavicle by pushing it against the pubic ramus or using a closed pair of scissors Clavicular Fracture The anterior clavicle is pressed against the ramis of the pubis. Care should be taken to avoid puncturing the lung by angling the fracture anteriorly. Theoretically, a fracture of the clavicle is less serious than a brachial nerve injury and often heals rapidly.
- 48. Symphysiotomy There is a high incidence of serious maternal morbidity and poor neonatal outcome. After delivery, the birth attendants should be alert to the possibility of postpartum haemorrhage and third- and fourth-degree perineal tears. Vesicovaginal Fistula Osteitis Pubis Retropubic Abscess Stress Incontinence Long Term Walking Disability / Pain Complications Associated with Symphysiotomy
- 51. Shoulder Dystocia AOCG Guidelines 1) Call for help - assistants, anesthesiology, pediatrician. Initiate gentle traction of the fetal head at this time. Drain the bladder if distended. 2) Generous episiotomy. 3) Suprapubic pressure with normal downward traction on fetal head. 4) McRoberts maneuver. Then, if these maneuvers fail, 5) Wood's screw maneuver. 6) Attempt delivery of posterior arm.
- 52. SHOULDER DYSTOCIA Summary 1.cannot be predicted or prevented-no accurate methods 2.ultrasonic measurements to estimate macrosomia have limited accuracy 3.planned c/sec due to macrosomia -not reasonable strategy 4.planned c/sec may be reasonable -nondiabetes (>5,000g) -diabetes (4,5000g)
- 53. SHOULDER DYSTOCIA Management :shoulder dystocia-cannot be predicted :well versed in the management principles :great importance to survival -reduction in the interval of time from delivery of the head to body :gentle traction, assisted by maternal expulsive effort next, large episiotomy, analgesia, clear the infant’s mouth and nose
- 54. SHOULDER DYSTOCIA 1.Moderate suprapubic pressure -by an assistant while downward traction 2.McRoverts maneuver -flexing the legs upon the abdomen -not increase pelvic diameter straightening of the sacrum symphysis pubis-toward the maternal head decrease the angle of pelvic inclination
- 56. SHOULDER DYSTOCIA 3.Woods corkscrew maneuver -rotating the posterior shoulder 180 degrees -anterior shoulder could be released
- 57. SHOULDER DYSTOCIA 4.Delivery of the posterior shoulder -post. arm: across the chest then delivery -next, shoulder girdle rotation into one of the oblique diameters of the pelvis delevery of ant. shoulder
- 58. SHOULDER DYSTOCIA 5.Rubin maneuver -1st, the fetal shoulder are rocked from side to side by applying force to the abdomen -if not successful, push the ant. shoulder toward the anterior surface of the chest
- 59. SHOULDER DYSTOCIA 6.Hibbard (1982) -press the fetal jaw and neck in the direction of the maternal rectum -strong fundal pressure anterior shoulder delivery -only fundal pressure, absence of other maneuver :77% complication fetal prthoprdic and neurologoc damage
- 60. SHOULDER DYSTOCIA 7.Zavanelli maneuver -cephalic replacement into the pelvis and then c/sec -return fetal head flex head push head back into vagina -terbutaline: Ut relaxation -fetal injury neonatal death stillbirth, brain damage
- 61. SHOULDER DYSTOCIA 8. Fracture of the clavicle -pressing the anterior clavicle against the ramus of the pubis -heal rapidly -not nearly as serious as a brachial nerve injury 9.Cleidotomy -cutting of the clavicle -usually used on the a dead fetus
- 62. SHOULDER DYSTOCIA 10. Symphysiotomy -maternal morbidity increased -urinary tract injury
- 63. SHOULDER DYSTOCIA Shoulder dystocia drill 1.call for help 2.generous episiotomy 3.suprapubic pressure -simple, only one assistant -while normal downward traction 4.McRoverts maneuver -two assistants resolve most case if fail, next steps may be attempted
- 64. SHOULDER DYSTOCIA Shoulder dystocia drill 1.call for help 2.generous episiotomy 3.suprapubic pressure -simple, only one assistant -while normal downward traction 4.McRoverts maneuver -two assistants resolve most case if fail, next steps may be attempted
- 65. HYDROCEPHALUS AS A CAUSE OF DYSTOCIA Hydrocephlus is an excessive accumulation of cerebrospinal fluid with consequent cranial enlargement :associated defects are common (neural tube defect) #head circumference: 32-38cm, fluid: 500-1500ml hydrocephalus: 50-80cm, fluid: 5l :1/3-breech, but whatever presentation, gross CPD and serious dystocia
- 66. HYDROCEPHALUS AS A CAUSE OF DYSTOCIA Diagnosis :sonography -compare the diameter of the lateral ventricle to the BPD of the head -evaluate the thickness of the cerebral cortex -compare the size of the head to that of the thorax and abdomen
- 67. HYDROCEPHALUS AS A CAUSE OF DYSTOCIA Diagnosis :sonography -compare the diameter of the lateral ventricle to the BPD of the head -evaluate the thickness of the cerebral cortex -compare the size of the head to that of the thorax and abdomen
- 68. HYDROCEPHALUS AS A CAUSE OF DYSTOCIA Technique of cephalocentesis #cephalic presentation -Cx :3-4cm dilatation vetricle may be tapped (8-inch, 17-gauge needle) #breech presentation -after breech and trunk delivered the face toward the martenal back transvaginally, below the ant. vaginal wall protect the birth canal
- 69. HYDROCEPHALUS AS A CAUSE OF DYSTOCIA #via martenal abdomen into the fetal head -bladder: empty skin: cleansed the needle: in the midline below the maternal umbilicus -before oxytocin stimulation -more successfully: sono-guided
- 70. FETAL ABDOMEN AS A CAUSE OF DYSTOCIA Enlargement of the fetal abdomen :greatly distended bladder ascites enlargement of the kidney or liver edematous fetal abdomen :before delivery, decision is made :but, prognosis is very poor
- 71. Shoulder Dystocia Management Suprapubic Pressure
- 72. Shoulder Dystocia Management Wood’s Screw Maneuver – high risk for humeral fx
- 73. Shoulder Dystocia Management Wood’s Screw Maneuver
- 74. Release of the anerior shoulder is initiated by firm pressure against the infant's jaw and neck in a posterior and upward direction. An assistant is poised, ready to apply fundal pressure after proper suprapublic pressure As the anterior shoulder slips free, fundal pressure is applied, and pressure against the neck is shifted slightly toward the rectum. Proper suprapubic pressure is continued. The Hibbard Maneuver
- 75. The Hibbard Maneuver Continued fundal and suprapublic pressure results in an upward- inward rotation of the newly freed anterior shoulder and a further descent in a position beneath the pubic symphysis.
- 76. As a result of the previous maneuvers, the transverse diameter of the shoulders is reduced. Lateral (upward) flexion of the head releases the posterior shoulder into the hollow of the sacrum. The Hibbard Maneuver