
Downloaded 120 times



![Reference
• World Wide Web page Richard. R, Physical
examination of Chest [online] May 1, 1996
[cited 2000 Dec 19]. Available from: URL:
http://medinfo.ufl.edu/year1/bcs/clist/chest.html
• Bickly L.S, B.(2011) Bates guide to physical
examination and history taking (10th
ed).Philadelphia: J.B.Lippincott
74](https://image.slidesharecdn.com/respiratorysystemexamination-171221151227/85/Respiratory-system-examination-74-320.jpg)

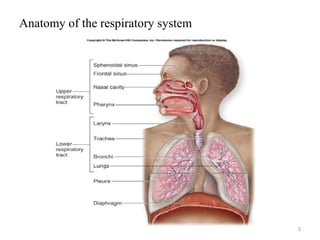
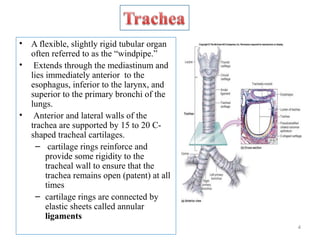
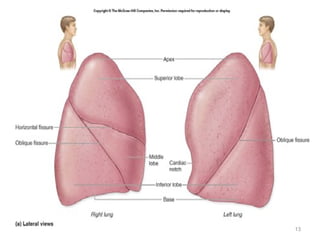
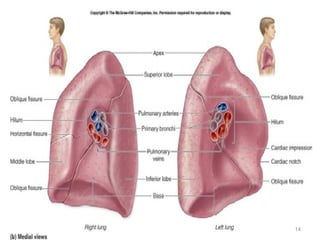
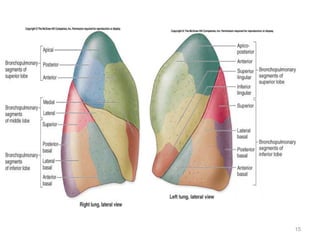
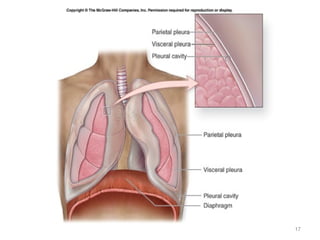
The document describes the anatomy and physiology of the respiratory system. It discusses the upper and lower respiratory tract, including the structures that make up the conducting and respiratory portions. It then provides detailed descriptions of specific structures like the trachea, bronchi, bronchioles, alveoli and lungs. It also covers the symptoms, signs and approach to examining patients presenting with respiratory complaints.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










