
Recommended
More Related Content
Similar to A liposarcoma of the retroperitoneum causing bowel obstruction
Similar to A liposarcoma of the retroperitoneum causing bowel obstruction (20)
More from SinzianaIonescu1
More from SinzianaIonescu1 (20)
Recently uploaded
Recently uploaded (20)
A liposarcoma of the retroperitoneum causing bowel obstruction
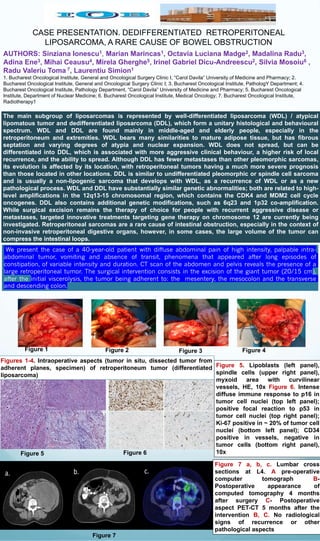
- 1. CASE PRESENTATION. DEDIFFERENTIATED RETROPERITONEAL LIPOSARCOMA, A RARE CAUSE OF BOWEL OBSTRUCTION AUTHORS: Sinziana Ionescu1, Marian Marincas1, Octavia Luciana Madge2, Madalina Radu3, Adina Ene3, Mihai Ceausu4, Mirela Gherghe5, Irinel Gabriel Dicu-Andreescu2, Silvia Mosoiu6 , Radu Valeriu Toma 7, Laurentiu Simion1 1. Bucharest Oncological Institute, General and Oncological Surgery Clinic I, “Carol Davila” University of Medicine and Pharmacy; 2. Bucharest Oncological Institute, General and Oncological Surgery Clinic I; 3. Bucharest Oncological Institute, PathologY Department; 4. Bucharest Oncological Institute, Pathology Department, “Carol Davila” University of Medicine and Pharmacy; 5. Bucharest Oncological Institute, Department of Nuclear Medicine; 6. Bucharest Oncological Institute, Medical Oncology; 7. Bucharest Oncological Institute, Radiotherapy1 Figure 5. Lipoblasts (left panel), spindle cells (upper right panel), myxoid area with curvilinear vessels, HE, 10x Figure 6. Intense diffuse immune response to p16 in tumor cell nuclei (top left panel); positive focal reaction to p53 in tumor cell nuclei (top right panel); Ki-67 positive in ~ 20% of tumor cell nuclei (bottom left panel); CD34 positive in vessels, negative in tumor cells (bottom right panel), 10x Figures 1-4. Intraoperative aspects (tumor in situ, dissected tumor from adherent planes, specimen) of retroperitoneum tumor (differentiated liposarcoma) Figure 1 Figure 2 Figure 3 Figure 4 Figure 5 Figure 6 Figure 7 Figure 7 a, b, c. Lumbar cross sections at L4. A pre-operative computer tomograph B- Postoperative appearance of computed tomography 4 months after surgery C- Postoperative aspect PET-CT 5 months after the intervention B, C. No radiological signs of recurrence or other pathological aspects The main subgroup of liposarcomas is represented by well-differentiated liposarcoma (WDL) / atypical lipomatous tumor and dedifferentiated liposarcoma (DDL), which form a unitary histological and behavioural spectrum. WDL and DDL are found mainly in middle-aged and elderly people, especially in the retroperitoneum and extremities. WDL bears many similarities to mature adipose tissue, but has fibrous septation and varying degrees of atypia and nuclear expansion. WDL does not spread, but can be differentiated into DDL, which is associated with more aggressive clinical behaviour, a higher risk of local recurrence, and the ability to spread. Although DDL has fewer metastases than other pleomorphic sarcomas, its evolution is affected by its location, with retroperitoneal tumors having a much more severe prognosis than those located in other locations. DDL is similar to undifferentiated pleomorphic or spindle cell sarcoma and is usually a non-lipogenic sarcoma that develops with WDL, as a recurrence of WDL or as a new pathological process. WDL and DDL have substantially similar genetic abnormalities; both are related to high- level amplifications in the 12q13-15 chromosomal region, which contains the CDK4 and MDM2 cell cycle oncogenes. DDL also contains additional genetic modifications, such as 6q23 and 1p32 co-amplification. While surgical excision remains the therapy of choice for people with recurrent aggressive disease or metastases, targeted innovative treatments targeting gene therapy on chromosome 12 are currently being investigated. Retroperitoneal sarcomas are a rare cause of intestinal obstruction, especially in the context of non-invasive retroperitoneal digestive organs, however, in some cases, the large volume of the tumor can compress the intestinal loops.