
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Yaws.pptx
Similar to Yaws.pptx (20)
More from Shivaraj Kumbar
Recently uploaded
Recently uploaded (20)
Yaws.pptx
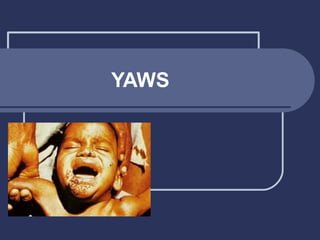
- 1. YAWS
- 2. YAWS • Yaws is also known as framboesia, buba, pian and Pain • Yaws is a chronical contagious, nonvenereal, treponemal infection in humans • It is caused by T. pertenue • It is characterized by a primary skin lesion followed by generalized eruption and a late stage of destructive lesions of the skin.
- 3. • The has been reported in India from the tribal communities living in hilly forests and difficult to reach areas in 49 districts of 10 states namely Andra Pradesh, Assam, Chattisharh, Gujatrat, Jharkhand, Madhya Pradesh, Maharashtra, Orissa Tamilnadu and Uttar Pradesh.
- 4. Epidemiological Determinants Agent Factors 1. Agent: • Yaws is caused by T.pertenue. • It measures 20 µ in length with 8 to 12 rigid spirals. • Treponema pertenue is morphologically identical to Treponema pallidum.
- 5. Reservoir of infection • Man is the only one reservoir of yaws. • Clinical lesions may relapse 2 to 3 times or more during the first five years of infection, and serve as a source for new infection. • The source of infection is usually skin lesions and exudates from early lesions.
- 6. Host Factors • Age: yaws is primarily a disease of childhood and adolescents. Over 75 % cases occurs within the age of 15 years. • Sex: Generally the prevalence among males is greater than females. • Immunity: Man has no natural immunity. Acquired immunity develops slowly and may take months or years to develop fully unless suppressed by treatment.
- 7. Environmental Factors • Climate: Yaws is endemic in warm and humid regions • Social Factors: Yaws is mostly endemic among the tribal people in India, whose way of living favour its transmission.
- 8. Mode of transmission • Direct Contact: By contact with secretions from infectious lesions. • Fomites: The organism may remain alive on fomites or on the floor in hot and humid conditions • Vector: There are some evidence that small flies and other insects feeding on the lesion may possibly convey the infection mechanically. • INCUBATION PERIOD: 3 To 5 Weeks
- 9. Clinical manifestations EARLY YAWS- - Primary lesion (Mother Yaws) appears at the site of inoculation after 3-5 weeks. - Seen on exposed parts of body - Lymph glands are enlarged. - With in next 3-6 weeks generalised eruption appears consists of large yellow, crusted, granulomatous eruptions .
- 10. During next five years, mucous membrane, periosteal and bone lesions develop, subside and relapse. - The early lesions are highly infectioous
- 11. • LATE YAWS - Destructive and deforming lesions of skin, bone and periosteum develop. CRAB Yaws – lesions of palm and soles Gangosa – lesions of soft palate, hard palate and nose
- 12. CONTROL OF YAWS 1. SURVEY: • Clinical survey of all families in endemic area. Should not cover less than 95% of total population. 2. TREATMENT • Single dose of Azithromycin or single long acting Penicillin will cure infection • Simultaneous treatment of cases and their likely contacts in the community will interrupt transmission
- 13. WHO has recommended 3 treatment policies- TOTAL MASS TREATMENT- In hyperendemic areas(> 10% prevalence of clinically active Yaws). Entire population treated with Pen G. JUVENILE MASS TREATMENT – In mesoendemic areas(5-10% prevalence). Treatment given to cases, contacts and all children below 15 years SELECTIVE MASS TREATMENT – In hypoendemic areas(<5% prevalence) Treatment to cases, household and other obvious contacts
- 14. 3. RESURVEY AND TREATMENT • Resuveys every 6-12 months to assess problem magnitude. 4. SURVEILLANCE • Surveillance and Containment measures for affected villages, households and contacts of known Yaws cases. • Epidemiological investigations to trace possible sources of infection, prophylactic treatment of contacts, follow up of cases
- 15. 5. ENVIRONMENT IMPROVEMENT • Recurrence of the disease is possible to occur unless environmental improvement is promoted. • Eg: Improvement of personal and domestic hygiene, adequate water supply, liberal use of soap , better housing conditions etc.
- 16. THANK YOU