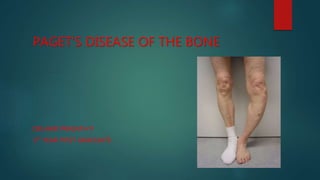
2. INTRODUCTION
The condition was initially described by Dr. James Paget in 1877
Also called as Osteitis Deformans
Partial or complete involvement of a single or multiple bones by
exaggerated rates of resorptive and osteogenic activity leading to bony
thickening and deformity.
Schmorl believed that approximately 3% of everyone above 40 years had
osteitis deformans
3. INTRODUCTION (Cont)
It has a predilection for the axial skeleton
Pelvis>tibia > Femur > Skull>spine >clavicle
But any bone may be affected
Paget disease is common in Europe, North America
It is rare in Asia and Africa
4. ETIOLOGY
UNKNOWN
Occasionally hereditary influence is noted on chromosome 18q
On electron microscopy of bone biopsies has demonstrated nuclear
inclusions,
similar to those found in viral diseases (Paramyxoviridae family) are found
in the highly nucleated osteoclasts
Endocrine and metabolic disturbances are unlikely because despite
extensive involvement , many bones are free of disease
5. PATHOPHYSIOLOGY
3 Phases:
i) Lytic
ii) mixed Lytic and Blastic
iii) Sclerotic
Different skeletal lesions may progress at different rates.
At a given time, multiple stages of disease may be demonstrated in
different skeletal regions of same patient
6. LYTIC PHASE
Disease begins with lytic phase
The bone is resorbed by osteoclasts that are more numerous, larger, and
have more nuclei (upto 100)
Bone turnover rate increased as much as 20times normal
7. Mixed Lytic and Blastic phase
Rapid increase in bone formation from numerous osteoblasts
Morphologically osteoblasts are normal
The newly formed bone is abnormal with collagen fibers deposited in
haphazard fashion rather than linear
As osteoclastic and osteoblastic activity repeats, high degree of bone turn
over occurs
8. Sclerotic Phase
The bone formation dominates and has a disorganized woven pattern and
is weaker than normal bone
Woven pattern allows the bone marrow to be infiltrated by excessive
fibrous connective tissue and blood vessels leading to hyper vascular bone
state
Eventually osteoblastic activity also declines and enters a sclerotic or
burned-out phase
Continued bone resorption is minimal or absent
19. Blade of Grass or Candle flame sign:
begins as a subchondral area of lucency with advancing
tip of V-shaped osteolysis, extending towards the
diaphysis
23. TREATMENT
Inactive lesions doesn’t require any intervention
Goals of treatment:
Suppression of Active disease
Relief of Pain
Prevention of Deformity and fractures
High output cardiac dysfunction
Reducing the Sarcomatous transformation
24. Suppressive Agents
BISPHOSPHONATES
2nd generation bisphosphonates like Tiludronate, Alendronate, risendronate
produces longer remission at lower doses.
Pamidronate – 30mg IV/day over 3hours for 3days
Zolidronic Acid- 5mg IV over 5 mins
First choice where rapid mineralization is required
in neurological symptoms, severe bone pain, risk of fracture
prior to elective surgery
Vitamin D and calcium supplements
It normalizes the ALP in 6 months
Bisphosphonates should not be used in patients with renal impairment
25. Calcitonin
Dosage – 100 IU / day SC/IM for 6-18 months
reduced to 50 IU / day x 3/week
Calcitonin therapy can temporarily arrest active disease
ALP, urine Hydroxyproline is reduced
Positive Calcium balance
High output heart failure is improved
Bone pain relieved
Surgical treatment is reserved for fractures, correction of bone deformity,
THR, Spinal surgery
Preoperatively and postoperatively calcitonin therapy gives good results and
reduces bleeding