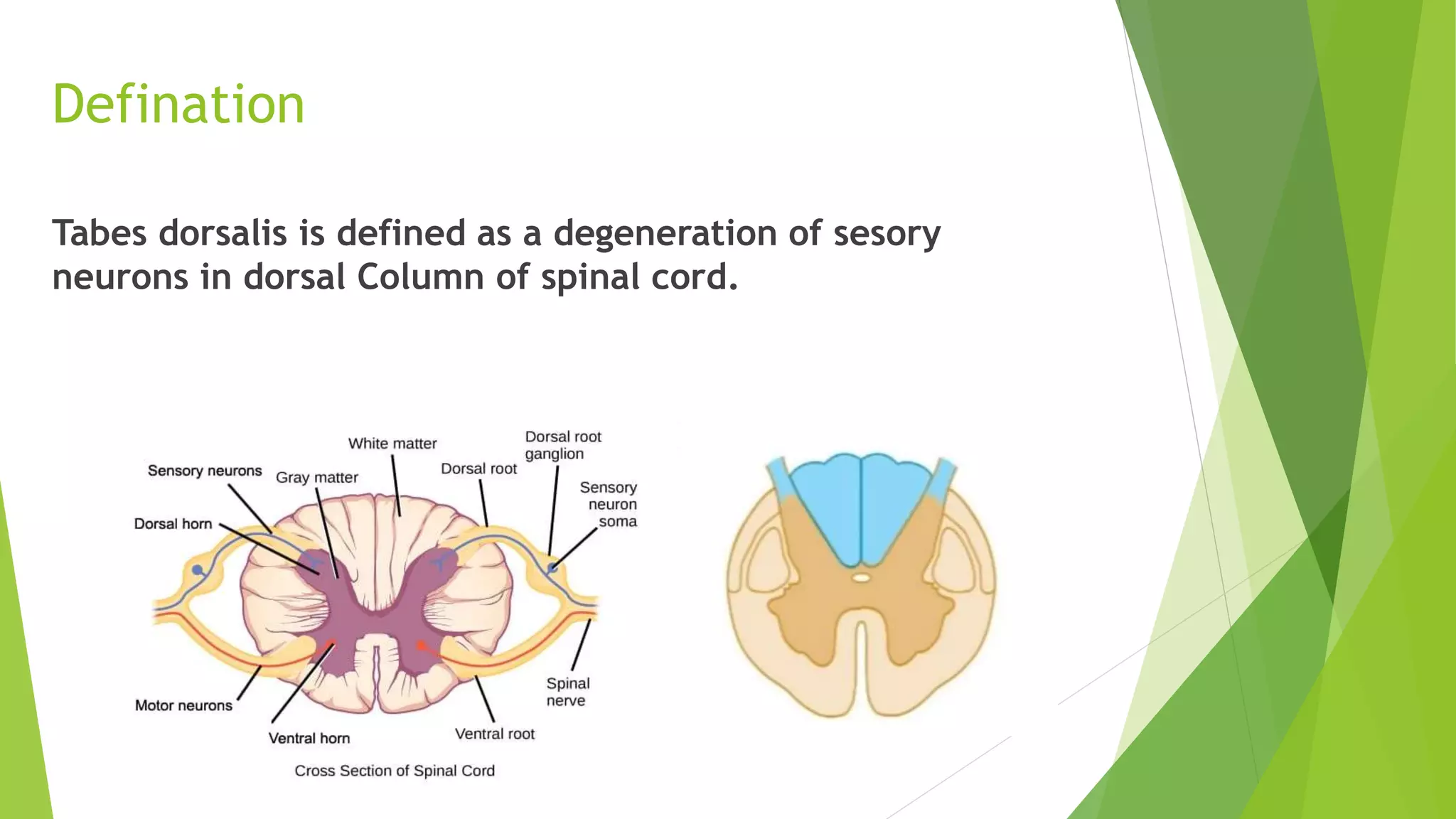
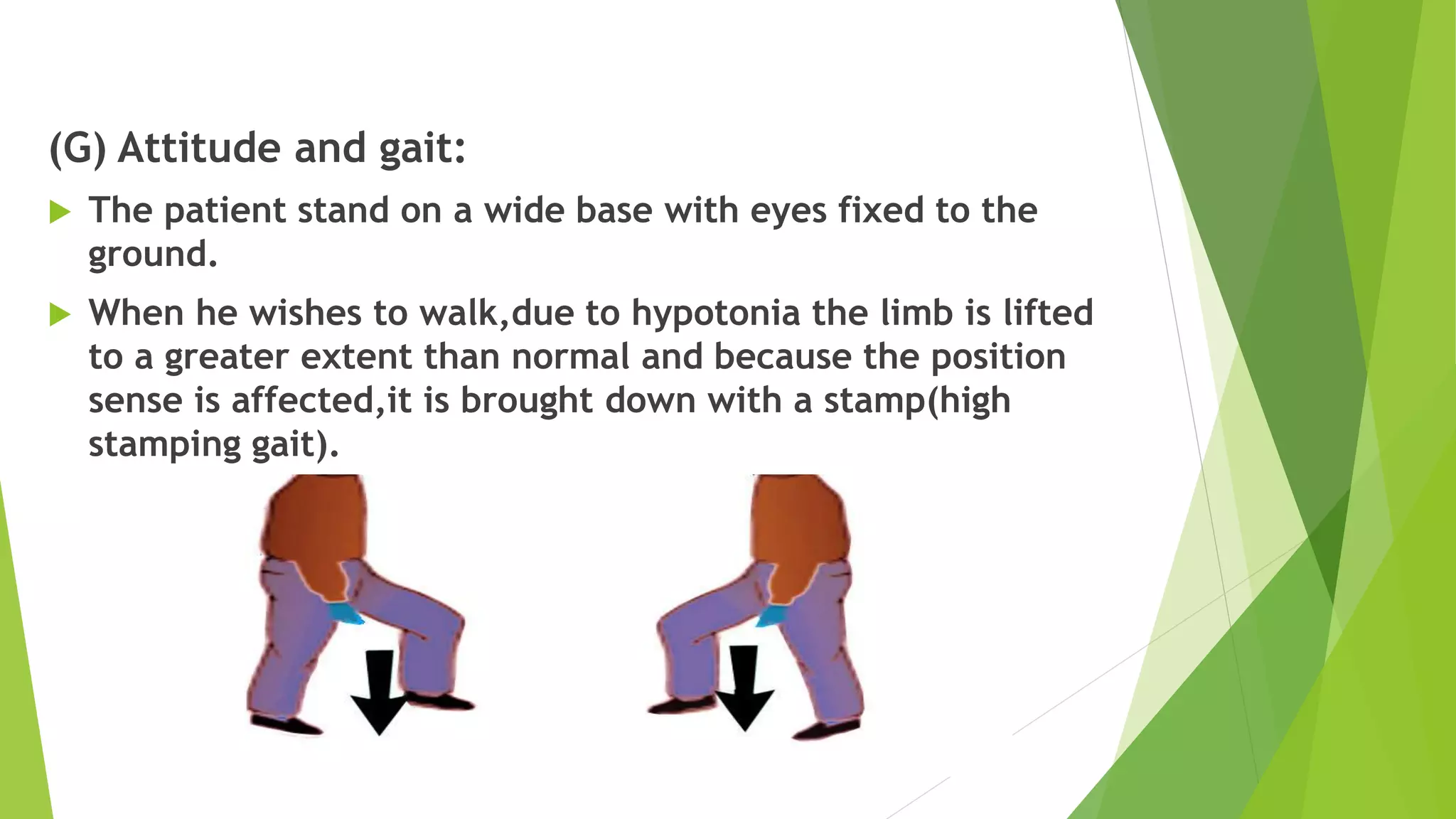
Tabes dorsalis is a degeneration of the sensory neurons in the dorsal column of the spinal cord caused by untreated syphilis. It primarily affects males during mid-life. Clinical features include sensory disturbances like lightning pains, root pain, and tabetic crises. Objective findings include loss of position and vibration sense in the lower limbs and sensory ataxia. Deep reflexes like ankle jerks are lost. Treatment involves penicillin injections to treat the underlying syphilis infection along with medications for pain management and physiotherapy.