
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Antidiabetic agents.pptx
Similar to Antidiabetic agents.pptx (20)
More from SDSHANMUGAKUMAR
Recently uploaded
Recently uploaded (20)
Antidiabetic agents.pptx
- 1. CHAPTER -11 : ANTIDIABETIC DRUGS Prepared and submitted by S.D.Shanmugakumar, M.Pharm., Ph.D Associate professor, Department of Pharmaceutical Chemistry Jyothishmathi Institute of Pharmaceutical sciences, Thimmapur, Karimnagar - 505527
- 2. Chapter -11 : Antidiabetic agents Antidiabetic agents comprise a chemically and pharmacologically heterogeneous group of drugs. The objective in treating diabetes mellitus is to prevent undue rises in blood glucose throughout each successive 24-hour period, without producing clinical hypoglycemiaHollander (1998). It is now widely accepted that good control of blood glucose prevents the development of microvascular (retinopathy, nephropathy) and neuropathic long-term complications of the disease in both type 1. In type 1 diabetes, where there is absent or little endogenous beta-cell function, insulin treatment is essential to prevent diabetic ketoacidosis, and the aim is the precise replacement of insulin in the fasting state and after meals. In type 2 diabetes, a choice of treatments, including insulin, is available. These comprise drugs that increase insulin secretion (sulfonylureas, such as glibenclamide, glipizide, gliclazide, and the meglitinide-like drugs, such as repaglinide and nateglinide), drugs that improve insulin sensitivity (biguanides, e.g., metformin), the thiazolidinediones, such as rosiglitazone, pioglitizone, and troglitazone), and drugs that reduce carbohydrate absorption (acarbose). In type 2 diabetes, choice of therapy depends on several factors (pregnancy and presence of obesity) and combinations of agents are often used to achieve better control than when one agent is used alone (e.g., insulin plus sulfonylurea, sulfonylurea plus metformin). Within each category of agent, choice is often related to pharmacokinetic considerations (gliclazide is short acting, whereas chlorpropamide and glibenclamide have long half-lives; there are numerous formulations of insulin producing a very short duration of action to an extremely long duration of action). Theoretically, an ideal agent would be one with a short duration of action and administered in association with each meal. However, patient convenience may take precedence over tight blood glucose control. New approaches include the use of glucagon-like peptide 1 (GLP-1) and its long-acting natural and synthetic analogues such as exendin 4, LY315902, and NN2211, which are undergoing evaluation.
- 4. Types of diabetes : Polydipsia, polyurea, ketnemia and ketourea. 1. Insulin dependent diabtes mellitus ( Type –I ) diabetes - It is an auto –immune disease caused by the pancreatic islet cells. 2. Non –Insulin dependent diabetes mellitus ( Type –II daibetes) – Due to insulin resistance and loss of secretory fucntion by pancreatic –Beta cells. HbA1C = below 7%
- 5. Hypoglycemic agents Hypoglycemic agents or antidiabetic agents lower the blood sugar and are used to treat the symptoms of diabetes mellitus. Pharmacological treatment of type –I diabetes requires intensive insulin therapy. The large number of short and long acting insulin are used for multiple doses for reducing sugars before and after food. Medical treatment of type 2 diabetes requires the management of hyperglycemis at the patients HbA1C below 7%. Classification: Drugs for diabetes mellitus - Insulin Long acting Intermediate Rapid Lispro NPH lente glargine
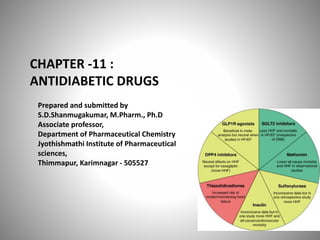
- 6. Non-Insulin antidiabetic drugs 1. Insulin secretagogues – Glipizide 2. Biguanides – Metformin 3. alpha –Glucosidase inhibitors – acarabose 4. Thiazolidine diones – Pioglitazone 5. Amylin analogs –Pramlinitidine 6. Incretin Modulators 7. Sodium glucose co-transporter 2 inhibitors – Dapagliflozin, Canagliflozin 8. DPP4- inhibitors – Vidagliptin, Saxgliptin, sitagliptin 9. GLP-1 ( Glucagon –like peptide -1) – Exenatide, Lixisenatide 10. Glucokinase inhibitors –Hexokinase –IV 11. DUAL PPAR agonists – Saroglitazar 12. Dopamine – 2- receptor agonist.
- 7. Insulin and its preparations The insulin molecule consists of two chains – Polypetide A and B. they are linked together by two disulfide bonds : 1. Chain A = 21 amino acids 2. Chain B = 30 amino acids Molcular weight – 5734 daltons It is biosynthesized from beta –cells of the pancreas from pre pro insulin – 110 amino acids chains with 12,000 daltons. It get cleaved in the endoplasmic reticulum losing a 24 amino acids from the N- terminal. It has a losing four basic amino acids – ArgB31, Arg B32, LysA64 and prohormone convertases PC1 and PC2.
- 10. Sources : It is obtained from bovine –based or porcine –based insulin. The biosynthetic insulins are : Biosynthetic human, semisynthetic human and analogs of human insulin. Types of insulin: 1. Rapid acting insulin anlogs : Insulin lispro, Insulin aspart, Insulin glulisine. Insulin lispro – lysB29 switched with Pro B 28 ( 5-15 min) Insulin aspart – The pro B 28 has substituted with Asp (5-15min) Insulin Glulisine – Val B3 is substituted with a Lys ( 15 min) Lys B29 coupled with glutamate. Short-acting insulin: Insulin NPH – Equal amounts of the positively charged polypeptide protamine to regular insulin (30-60min) Insulin lente (30-60min) –regular insulin and zinc in an acetate buffer.
- 11. Long acting insulin : Insulin gargline: Replacement of AsnA21 by glycine and the two Arg amino acids to the C-terminus of the B chain ( 0.8-2hrs). Insulin ultralente : Long-acting insulin that is 4-zinc acetate crystalline product. Insulin detemer : N-acetylation of Lys B29 with the 14- carbon mystic acid. Premixed insulins : Mixture of NPH and lispro can be 50:50 or 75:25
- 12. Oral hypoglycemic agents The insulin secretagogues includes the sulfonyl ureas and meglitinides both increase insulin release from the pancreas by a common mechanism: Mechanism of Action: All of the sulfonyl ureas and meglinides are stimulate the release of insulin from B- cells of the pancreas. These cells metabolize glucose in mitochondria to produce ATP. The intracellular ratio of ATP/ADP, resulting in the closure of the ATP – Sensitive K+ channel on the plasma membrane. Closure of this channel triggers the opening of Voltage – sensitive Ca2+ channels leading to rapid influx of Ca2+. Increased intracellular Ca2+ causes an alteration in the cytoskeleton and stimulates translocation of insulin – containing granules to the plasma membrane and the exocytotic release of insulin. ATP- Sensitive K+ channel has two units of the binding site for both sulfonyl ureas and ATP designated as the sulfonyl urea receptor – type -1 (SUR1)an inwardly rectifying K+ channel.
- 16. Sulfonyl ureas First generation : Tolbutamide, chlorpropamide Second generation : Glipizide, Glimepiride 1. The benzene ring should contain one substituent, preferably at the para position (R). 2. The substituents that seem to enhance hypoglycemic activity are methyl, amino, methyl, acetyl, chloro, bromo, methylthio, and trifluoromethyl groups. 3. Compounds with P-( β-arylcarboxamido ethyl) substituents have better activity than the first generation agents. 4.The group attached to the terminal nitrogen (R2) should be certain size and should impart lipophilic properties to the molecule.
- 17. Adverse effects : Sulfonyl ureas are associated with weight gain, though less so than insulin. Tolbutamide 3-Butyl-1- ( 4-methyl benzene sulkfonyl) urea
- 18. Metabolism Metabolized in the liver principally via oxidation of the P-methyl group producing the carboxyl metabolite. Many of the metabolized to 4- hydroxy tolbutamide. Uses: For treatment of NIDDM – Non –insulin dependent diabetes mellitus) Synthesis :
- 20. Chlorpropamide 1-(4- chlorobenzene sulfonyl) -3- propyl urea Meatbolism : Chlorpropamide has a considerabley longer half –life than the other sulfonyl ureas and has a greater tendency for adverse effects. Uses : Treatment of NIDDM in conjuction with diet and exercise.
- 21. Glipizide N-2(4-(Cyclohexylcarbamoyl) amino) sulfonyl) Phenyl) ethyl)-5-methyl pyrazine -2- carboxamide. Metabolism : Hepatic metabolism Uses : Adjunct diet for the control of Hyperglycemia.
- 22. Metabolism Hydroxylation of non-terminal aliphatic carbon adjacent to aromatic ring Aliphatic hydroxylation of methyl carbon adjacent to aromatic ring AndFromCyProduct Hydroxylation of alicyclic secondary carbon Hydroxyla tion of alicyclic secondary carbon Hydroxylation of alicyclic secondary carbon
- 23. Glimepride Metabolism : Glimepride is metabolized in the liver. Primarily in Cytochrome P2 C9 to the active metabolite cyclohexyl hydroxy methyl derivative ( M-1) which is further metabolized to the inactive metabolite carboxyl derivative. Uses : Treatment of non- insulin dependent type diabetes mellitus.
- 24. Meglitinides Repaglinide 2-ethoxy -4 ( 1s – 3-Methyl -1- ( 2- Piperidyl) – Phenyl) Butyl) carbamoyl) methyl benzoic acid. Metabolism : Repalinidine is rapidly metabolised via oxidation and dealkylation cytochrome P4503 A4 and 2C9 to form the major dicarboxylic acid derivative (M2)
- 25. Hydroxylation of non-terminal aliphatic carbon adjacent to aromatic ring Aliphatic hydroxylation of methyl carbon adjacent to aromatic ring AndFromCyProduct Hydroxylation of alicyclic secondary carbon Hydroxylation of alicyclic secondary carbon
- 26. Uses : As an adjunct to diet and exercise to improve glycemic control Nateglinide 2- hydroxy -4(propan-2yl) cyclohexyl) methylidene) amino -3- phenyl propanoic acid. Uses : For the treatment of NIDDM in conjuction with diet and exercise
- 27. Metabolism O-Hydroxylation of monosubstituted benzene Hydroxylation of non- terminal aliphatic carbon adjacent to aromatic ring Hydroxylation of alicyclic secondary carbon Hydroxylation of alicyclic secondary carbon
- 28. Insulin sensitizers ( PPAR) agonists The thiazolidine diones are the classic examples of PPARg agonists and commonly referred to as “ glitazones”. Thiazolidine diones are ligands of the perioxisome proliferator – activayed receptor – gamma ( PPAR –γ) that is expressed in the nucleus of adipocytes, myocytes and hepatocytes. PPARγ that regulates the expression of genes involved in lipid and glucose metabolism, insulin signal transduction and adipocyte differentiation. MOA: PPARγ is expressed in multiple tissue types ( skeletal muscle, fat & liver). Activation of PPAR – Gammareceptors regulates the transcription of insulin- responsive genes involved in the control of glucose production, transport and utilization.
- 29. Thiazolidiene diones is an increased expression of the glucose GLUT4. The increased expression of GLUT4 in addition to mediators of insulin signal transduction increases the ability of cells ( Adipocytes) which take up the glucose when stimulated by the insulin.
- 30. Rosiglitazone 5-(4-(2-(N-methyl-N (2-pyridyl) amino) ethoxy) benxyl)Thiazolidine -2,4 dione. Rosiglitazone is an anti-diabetic drug in the thiazolidinedione class of drugs. It is marketed by the pharmaceutical company GlaxoSmithKline as a stand-alone drug (Avandia) and in combination with metformin (Avandamet) or with glimepiride (Avandaryl). Like other thiazolidinediones, the mechanism of action of rosiglitazone is by activation of the intracellular receptor class of the peroxisome proliferator-activated receptors (PPARs), specifically PPARγ. Rosiglitazone is a selective ligand of PPARγ, and has no PPARα-binding action. Apart from its effect on insulin resistance, it appears to have an anti- inflammatory effect: nuclear factor kappa-B (NFκB) levels fall and inhibitor (IκB) levels increase in patients on rosiglitazone. Recent research has suggested that rosiglitazone may also be of benefit to a subset of patients with Alzheimer's disease not expressing the ApoE4 allele
- 31. N-Dealkylation of mixed tertiary amine AndFromCyProduct Enzyme: Cytochrome P450 1A2 BioSystem: HUMAN
- 32. N-Dealkylation of mixed tertiary amine AndFromCyProduct 2,4-Thiazolidinedione ring opening Enzyme: Cytochrome P450 1A2 BioSystem: HUMAN Enzyme: Cytochrome P450 1A2 BioSystem: HUMAN Uses :Rosiglitazone is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type -2- diabates
- 33. Pioglitazone 5- (4-(2- (5-ethylpyridin – 2yl) ethoxy) Phenyl) methyl) -1,3 thiazolidine – 2,4 dione. Pioglitazone is a thiazolidinedione used adjunctively with diet and exercise to normalize glycemic levels in adults with type 2 diabetes mellitus. Pioglitazone is an antihyperglycemic used as an adjunct to diet, exercise, and other antidiabetic medications to manage type 2 diabetes mellitus.4,5,6,7 It is administered as a racemic mixture, though there is no pharmacologic difference between the enantiomers and they appear to interconvert in vivo with little consequence. The thiazolidinedione class of medications, which also includes rosiglitazone and troglitazone, exerts its pharmacological effect primarily by promoting insulin sensitivity and the improved uptake of blood glucose4 via agonism at the peroxisome proliferator-activated receptor-gamma (PPARγ).1 PPARs are ligand- activated transcription factors that are involved in the expression of more than 100 genes and affect numerous metabolic processes, most notably lipid and glucose homeostasis
- 34. Metabolism Pyridine N-oxidation Hydroxylation of non-terminal aliphatic carbon adjacent to aromatic ring AndFromCyProduct Hydroxylation of non-terminal aliphatic carbon adjacent to aromatic ring AndFromCyProduct Enzyme: Cytochrome P450 1A2 BioSystem: HUMAN
- 35. Uses : Pioglitazone is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. Adv.effects : Fluid retetntion, Congestive heart failure. Biguanindes: The biguaninides are chemically represented by the linkage of two guanidine group with difference in side chains. The biguanides include metformin, phen formin and buformin. Metformin 1- carbamimidamido – N,N – dimethyl methanimidamide.
- 37. Metformin is a widely-used drug that results in clear benefits in relation to glucose metabolism and diabetes-related complications. The mechanisms underlying these benefits are complex and still not fully understood. Physiologically, metformin has been shown to reduce hepatic glucose production, yet not all of its effects can be explained by this mechanism and there is increasing evidence of a key role for the gut. At the molecular level the findings vary depending on the doses of metformin used and duration of treatment, with clear differences between acute and chronic administration. Metformin has been shown to act via both AMP-activated protein kinase (AMPK)-dependent and AMPK- independent mechanisms; by inhibition of mitochondrial respiration but also perhaps by inhibition of mitochondrial glycerophosphate dehydrogenase, and a mechanism involving the lysosome. In the last 10 years, we have moved from a simple picture, that metformin improves glycaemia by acting on the liver via AMPK activation, to a much more complex picture reflecting its multiple modes of action. More work is required to truly understand how this drug works in its target population: individuals with type 2 diabetes.
- 38. MOA of metformin
- 39. Metabolism : Metformin is excereted in the urine via tubular excretion as un metabolized drug with a half –life of approx 3-5 hrs. Uses : For adjunct diet and exercise in adult patients. Adv.effects : Epigastric discomfort, flatulence and vomiting. Alpha –GLUCOSIDASE INHIBITORS Alpha –amylase and alpha glucosidases are key enzymes responsible for the metabolism of carbohydrates. Glucosidase enzymes catalyze hydrolysis of starch to simple sugars. In humans, these enzymes aid digestion of dietary carbohydrates and starches to produce glucose for intestinal absorption, which in turn, leads to increase in blood glucose levels. Inhibiting the function of these enzymes in patients with type-2 diabetes may reduce hyperglycemia.
- 40. Description : Oral anti-diabetic drug Target(s) ;Glucosidase Generic : Acarbose Commercial Name ; Precose (United States), Glucobay (United Kingdom), Prandase (Canada) Combination Drug(s) : Acarbose tablets may be combined with sulfonylureas, insulin or metformin in fixed doses (Drugs.com). Other Synonyms : acarbosa, acarbosum IUPAC Name ;(2S,3R,4R,5S,6R)-5-[(2R,3R,4R,5S,6R)-5-[(2R,3R,4S,5S,6R)-3,4-dihydroxy-6- methyl-5-[[(1S,4R,5S,6S)-4,5,6-trihydroxy-3-(hydroxymethyl)cyclohex-2-en-1-yl]amino]oxan- 2-yl]oxy-3,4-dihydroxy-6-(hydroxymethyl)oxan-2-yl]oxy-6-(hydroxymethyl)oxane-2,3,4-triol Ligand Code in PDB ;ACR
- 41. Drug-Target Complex: Each molecule of the maltase glucoamylase (MGAM) enzyme is made up of 1867 residues and contains two homologous catalytic subunits. The N-terminal domain (residues 1-868) is called NtMGAM and C-terminal domain (residues 955-1867) is called CtMGAM. Both subunits carry out the same catalytic reaction - hydrolysis of α-(1,4) linked glucose units in linear oligosaccharide substrates yeilding glucose monomers. However, they differ in their distinct specificity for varying lengths of malto-oligosaccharides Both the NtMGAM and CtMGAM domains are comprised of five major sub-domains: a trefoil Type-P domain an N-terminal β-sandwich domain a catalytic (β/α)8 barrel domain with two inserted loops a proximal C-terminal domain a distal C-terminal domain The tertiary structures of NtMGAM and CtMGAM reveal a similar fold ,however the latter has a 21-residue insert (shown in cyan, Figures 2b and 3b), and gives it a larger binding pocket to bind longer substrates than NtMGAM.
- 43. Metabolism Acarbose is only metabolized with in the GIT – Intestinal bacteria and also digestive enzymes. Glycoside hydrolysis Alkyl-OH-glucuronidation Alkyl-OH- glucuronidation
- 44. Uses : For thr treatment and management of diabetes -II Voglibose Voglibose is an alpha-glucosidase inhibitor indicated in the management of postprandial blood glucose in patients with type II diabetes. 1S,2S,3R,4S,5S – 5 –(1,3 – dihydroxy propan – 2yl) amino) -1-(hydroxymethyl) cyclohexane, 1,2,3,4 -terol
- 45. Mechanims of action : Alpha-glucosidase inhibitors are saccharides that act as competitive inhibitors of enzymes needed to digest carbohydrates: specifically alpha-glucosidase enzymes in the brush border of the small intestines. The membrane-bound intestinal alpha-glucosidases hydrolyze oligosaccharides, trisaccharides, and disaccharides to glucose and other monosaccharides in the small intestine. Acarbose also blocks pancreatic alpha-amylase in addition to inhibiting membrane-bound alpha-glucosidases. Pancreatic alpha-amylase hydrolyzes complex starches to oligosaccharides in the lumen of the small intestine. Inhibition of these enzyme systems reduces the rate of digestion of complex carbohydrates. Maltase-glucoamylase, intestinal
- 46. Uses : For the treatment of diabets, especially post – prandial blood glucose. Adv.effects : GI –Irritation, bloating, flatulence. GLP-1 Analogs(Glucagon Like peptide -1) Glucagon Glucagon (shown in red) is recognized by cells using a G-protein- coupled receptor (shown in blue). This receptor is a bit different than a typical GPCR, like the one that recognizes adrenaline. It has an extra domain on the outer side of the cell (shown at the top of the illustration here), which traps glucagon and delivers it to the membrane-spanning portion. When glucagon binds, it activates G- proteins inside the cell, starting off a cascade of responses that lead to release of glucose.
- 47. Incretineffect the phenomenon whereby oral glucose elicits higher insulin secretory responses than does intravenous glucose,
- 48. MOA of GLP-1 Agonists
- 49. GLP-1 is secreted from L- cells which is a part of glucose –induced insulin secretion from pancreatic Beta cells. Metabolism of glucose in the instestinal L –cells leads to closure of ATP- linked potassium channels resulting in the depolarization of the membrane and entry of Ca2+ which secrete the GLP-1. GLP-1 agonists – Exetanide, liraglutide, albiglutide. Exetanide GLP-I agonist
- 50. Amylin agonists Amylin is a hormone that consists of a single chain of 37 amino acids and is released from pancreatic –Beta cells, co secreted with insulin primarily involved in the controlling post prandial blood sugars. Pramlintide :Pramlintide is a relatively new adjunct treatment for diabetes (both type 1 and 2), MOA : Pramlintide is an amlyinomimetic, a functional analog of the naturally occurring pancreatic hormone amylin. Amylin has activity in a number of gastrointestinal and glucodynamic systems, and by mimicking its activity, pramlintide acts to improve glycemic control through modulation of the rate of gastric emptying, prevention of post-prandial rise in glucagon levels, and by increasing sensations of satiety, thereby reducing caloric intake and potentiating weight loss. There appears to be at least three distinct receptor complexes that bind with high affinity to amylin. All three complexes contain the calcitonin receptor at the core, plus one of three Receptor activity- modifying proteins, RAMP1, RAMP2, or RAMP3.