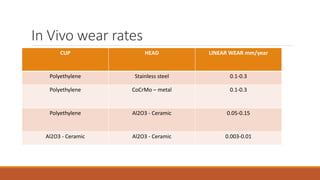
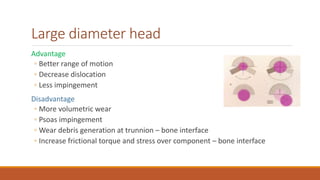
This document discusses the tribology of total hip replacements (THRs). It covers topics like wear, lubrication, friction, bearing materials, and concerns with different bearings. Regarding bearings, it describes hard-on-soft bearings like metal-on-polyethylene, and hard-on-hard bearings like ceramic-on-ceramic and metal-on-metal. It also discusses factors like head size, noting that large heads can decrease dislocation but increase wear.