2. MICTURITION
Def:- Micturition is a reflex process by which urine is voided from
urinary bladder through urethra. In grown up children and adults,it
can be controlled voluntarily to some extent.
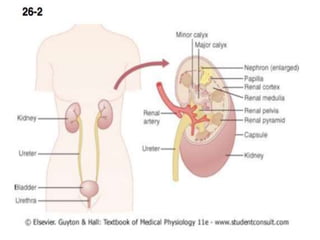
RENAL SYSTEM
Renal system includes:-
1. A pair of kidneys
2. A pair of ureters
3. One urinary bladder
4. One urethra
In male urethra is long but in female it is short.
3.
4. URINARY BLADDER
Urinary bladder consist of the
Body
neck
And internal urethral sphincter.
Smooth muscle forming the urinary bladder is called
detrusor muscle.
Detrusor muscle is formed by ill defined three layers of muscles fiber
Inner longitudinal layer
Middle circular layer
Outer longitudinal layer
Trigone:- At the posterior surface of bladder wall ,there is a triangular
area called Trigone.
Two ureters enter at the upper angle of Trigone.
Neck:- lower part of bladder is narrow and forms the neck of Bladder.
5. Internal urethral sphincter:- Distal end of
bladder is guarded by detrusor muscle called
internal sphincter.It opens towards urethra.
External urethral sphincter:- At the Distal end
of urethra , there is external urethral sphincter
made up of skeletal muscles fibers.
It is responsible for voluntary control of
micturition
6.
7. NERVE SUPPLY OF URINARY BLADDER
Urinary bladder and internal sphincter is
supplied by sympathetic and parasympathetic
divisions of Autonomic Nervous system
(ANS)
The external sphincter is supplied by the
somatic motor nerve fibers.
8.
9. SYMPATHETIC NERVE SUPPLY
Preganglionic fibers of sympathetic nerve arise from lumber segments
L1 , L2 of spinal cord.
Fibers pass through lateral sympathetic chain without any synapse
terminate in Hypogastic nerve , which supplies the detrusor muscles
and internal sphincter of urinary bladder.
FUNCTIONS OF SYMPATHETIC NERVE
Stimulation of sympathetic nerve causes relaxation of detrusor
muscles and constriction of internal sphincter
It causes filling of urinary bladder by urine and so called nerve
of filling.
10. PARASYMPATHETIC NERVE SUPPLY
Preganglionic fiber of parasympathetic nerve arise from second ,third and fourth
sacral segments(S2,S3,S4) of spinal cord form the pelvic nerve.
These fibers run through hypogastric ganglion and synapse with
postganglionic neurons situated close to urinary bladder
FUNCTIION PARASYMPATHETIC NERVE
Stimulation of pelvic (parasympathetic) nerve causes contraction of detruser
muscles and relaxation of the internal sphinctor leading to emptying of
urinary bladder. so, parasympatheric nerve is called the nerve of micturition
Pevlic nerve has also the sensary fibers which carry impulse from stretch
receptors present on the wall of urinary bladder and urethera to the C N S.
11. SOMATIC NERVE SUPPLY TO
EXTERNAL SPHINCTER
The external sphincter is skeletal muscle supplied by somatic nerve
called pudendal nerve. It arises from second ,third and fourth sacral
segments(S2,S3,S4) of spinal cord.
FUNCTION OF PUDENDAL NERVE
It maintains the tonic contraction of skeletal muscles fibers of
the external sphincter and keeps the external sphincter
constricted always.
During micturition this nerve is inhibited.
It causes relaxation of external sphincter leading to voiding of
urine(micturition).
So pudendal nerve is responsible for voluntary control of
micturition.
12. FILLING OF URINARY BLADDER
Urine is formed in the nephrons of kidneys continuosly and transported
by ureter to urinary bladder by peristallic movement in the ureter.
The direction of the ureter after leavling the kidney is downward and
outward and then horizontally before entering the bladder .
Due to adaptation of detruser muscle urine is collected in the bladder
without much increase in the intravesical pressure.
Relationship between the volume of urine and pressure in the urinary
bladder is studied by Cystometrogram.
13. CYSTOMETROGRAM
Def:- Cystometrogram is the graphical recordingof pressure changes in the
urinary bladder in relation to rise in the volume of urine collected in it.
METHOD OF RECORDING OF CYSTOMETROGRAM
A double lumen catheter is introduced in the urinary bladder.
One of the lumen is used to infuse fluid into the bladder and the other
one to record the pressure changes .
First the bladder is emptied completely then small known volume of
fluid is introduced into the bladder at regular intervals
The intravesical pressure is recorded.
A graph is obtained by plotting all the values of volume and the
pressure .
This graph is called Cystometrogram
15. CYSTOMETROGRAM SHOWS THREE SEGMENTS
SEGMENT I
When urinary bladder is empty the intravesical pressure is zero.
When about 100ml fluid collected the pressure rises sharply to about 10cm H2O
SEGMENT II
It shows plateau the intravesical pressure remains more or less 10cm H2O without any change
even introducing 300-400ml of fluid.
It is accordance with law of Laplace.
SEGMENT III
When collection of 300-400ml of fluid the contraction of detrusor muscle is intense and
increase in urge of micturation
Still voluntary control is possible upto 600-700ml the pressure rises to 35-40cm H2O.
When intravesicular pressure is above 40cm H2O.the constriction of detrusor muscles
become more intense and voluntary control is not possible.
16. LAW OF LAPLACE
Pressure in spherical organ is inversly proportional to its radius, the
tone remaining constant.
P=T/R
P= presure ,
T= tension
R= Radius
If radius is more pressure is less and if radius is less pressure is more
provided tone remains constant.
Urinary bladder obeys Laplace law.
When urine collected beyond 400ml ,the pressure rises sharply and urge
of micturition starts.
Still voluntary control of micturition is possible.
Beyond 600-700ml of urine collected then control starts failing.
18. MICTURATIONREFLEX
FILLING OF URINARY BLADDER
|
STIMULATION OF STRETCH RECEPTORS
|
AFFRENT IMPULSES PASS VIA PELVIC NERVE
|
SACRAL SEGMENTS OF SPINAL CORD
|
EFFERENT IMPULSE VIA PELVIC NERVE
|
CONTRACTION OF DETRUSER MUSCLE AND
RELAXATION OF INTERNAL SPHINCTOR
|
FLOW OF URINE IN URETHRAAND
STIMULATION OF STRETCH RECEPTORS
|
AFFERENT IMPULSES VIA PELVIC NERVE
|
INHIBITION OF PUDENDAL NERVE
|
RELAXATION OF EXTERNAL SPHINCTER,
|
VOIDING OF URINE
19. The Micturition Reflex
Components of the
reflex arc that
stimulates smooth
muscle contractions in
the urinary bladder.
Micturition occurs
after voluntary
relaxation of the
external urethral
sphincter.
20. MICTURITION
It is the reflex by which micturition occurs.
It is elicited by stimulation of stetch receptors on the wall of urinary
bladder and urethra.
When urine is collected 300-400ml the intervesicular pressure increases
and the stretch receptors are stimulated and generation of sensory
impulse.
The sensory impulse from the receptors reach the sacral segments of
spinal cord via sensory fibers of pelvic nerve(parasympathetic nerve)
Motor impulses from spinal cord travel through motor fiber of pelvic
nerve to bladder and internal sphincter
Causes contraction of detrusor muscles of bladder and relaxation of
internal sphincter urine enters urethra from bladder.
21. Stretch receptors in urethra stimlated send
afferent impulses to spinal cord via pelvic nerve
fibres.
These impulse inhibit pudendal nerve ,external
sphinder relaxes and micturition occurs.
Once micturition reflex begins it is self
regenerative further sensory impulse cycle
continues and urine is voided completely.
During micturation the flow of urine is facilitated
by the increase in the abdominal pressure due to
voluntary contraction of abdominal muscles.
22. HIGHER CENTERS OF
MICTURITION
Spinal centers are present in lumber segments (L1, L2), sacral segments
(S2, S3, S4) of spinal chord but regulated by higher centers which
control micturition
(1) INHIBITARY CENTER OF MICTURITION
Inhibitary center in midbrain and cerebral cortex inhibit the micturition
by supressing mictonitim center.
(2) FACILITATORY CENTER OF MICTURICTION
Facilitatory center are in Pons facilitates micturition via spinal center
24. 1. Atonic bladder
Due to distruction of sensary pelvic nerve fibers of urinary bladder
A. spinal injury ( first stage of spinal shock.)
B. Syphilis – destruction of dorsal sensary nerve roots.
In atonic bladder loss of tone in the urinary bladder due to
destruction of sensary nerve fibers. The bladder is filled up without
any stretch becomes flacid. No micturition contraction.
Bladder filled completely and overflow in drops.
It is called overflow incontenence or overflow dribling.
25. 2. Automatic bladder
This occurs during second stage of spinal shock after complete trans-
section of spinal cord above sacral segments.
It is due to hyperactive micturation reflex.
Voluntary control of micturation is lost.
Even small amount of urine collected in bladder micturation reflex
occurs.
Resulting in empting of bladder.
26. 3. Uninhibited neurogenic
bladder
Due to lesion in midbrain continuous excitation of spinal micturation
centers.
Resulting in frequent and uncontrollable micturation even small
quantity of urine collected in bladder will elicit micturation reflex.
It is also called spastic neurogenic bladder or hyperactive neurogenic
bladder.
27. 4. Nocturnal micturition Or Enuresis Or
Bed wetting
Involuntary voiding of urine during night is called Enuresis.
It is due to absences of voluntary control of micturition.
It is common and normal process in inafants and children before 3 yrs. Due
to under developments of voluntary control of micturition because of
incomplete myelilation of motor nerve fobers of urinary bladder.
When myelination is complete voluntary control of micturition develops and
enuresis in children stops.
In adult and grown up children due to psyclogical factors.
It may also occurs during inpairment of motor area of cerebral cortex.
28. Abnormalities of micturition
1. Atonic bladder
This is due to destruction of sensory nerve fibers from urinary
from the bladder. When the dorsal sacral roots are interrupted by
diseases of the dorsal roots such as tabes dorsalis or when there is
crush injury to sacral segments of spinal cord, person looses
bladder control (abolition of reflex contractions of the bladder).
Bladder muscle looses the tone (hypotonic) and becomes flaccid).
Bladder fills to the capacity and overflows few drops at a time
through the urethra (overflow incontinence or overflow dribbling).
29. 2. Automatic bladder (Spastic
neurogenic bladder)
During spinal shock after complete transection of
spinal cord above sacral centres of micturition, the
urinary bladder looses its tone and becomes flaccid
and unresponsive. So, the bladder is completely
filled, and later urine overflows by dribbling. After
the spinal shock has passed, the voiding reflex
returns although there is no voluntary and higher
centre control.
Whenever, the bladder is filled with some amount
of urine, there is automatic evacuation of the
bladder.
30. 3. Uninhibited neurogenic bladder
Due to a lesion in some parts of brain stem
(interrupting most
of the inhibitory signals), there is continuous
excitation of
spinal micturation centre by the higher centre.
There is
uncontrollable micturation. Even a small
quantity of urine
collected in bladder will elicit the micturation
reflex increasing
the frequency of micturation.
31. Nocturnal micturition (Bed wetting)
This is normal in infants and children below 3 years. It occurs due to
incomplete myelination of motor nerve fibers of the bladder
resulting loss of voluntary control of micturition .
33. URINALYSIS
A analysis of the volume and physical chemical and microscopic
properties of urine is called urinalysis.
Characteristics of normal urine
1. Volume – 1 to 2 Liters/day normal.
2. Color – yellow or amber.
3. Turbidity – Transparent freshly.
But cloudy (Turbid) after standing.
4. Odor – Mildly aromatic but becomes ammonia like upon standing.
In diabetic – fruity due to presence of ketone bodies .
5. PH – Ranges from 4.6 to 8.0, average 6.0 .
Depends on diet – Vegetarian alkality
Non Vegetarian acidity.
6. Specific gravity 1.001 to 1.035.33
34. Abnormal Constituent of Urine
1. Albumin – excessive in urine called
• Albuminuria.
2. Glucose present - * In diabetes Mellitus
* Excessive stress
* Excessive epinephrine
3. RBC – Hematuria pathological condition Irritation
from kidney stone.
4. Ketone Bodies – High level of ketone
Called ketonuria
Indication – diabetes mellitus,
– Anorexia
– starvation.
34
35. 5. Bitirubin – when RGC destroyed by macrophages
Bilirrubin liberated.
Above normal level in urine called
Bilrubinia.
6. Casts – Casts are tiny mass
white blood cell casts
Red blood cell casts
Epithelial casts.
6. Microbes – E. Coli
Fungus
35
36. Dialysis
If a person’s kidneys are so impaired by disease - kidney
failure, injury
Then blood must be cleaned artificially by Dialysis.
Dialyo = to separate.
The separation of large solutes from smaller ones by
diffusion through selectively permeable membrane.
Method of Dialysis
1) Hemodialysis
2) Peritoneal Dialysis
36
37. 1) Hemodialysis
(Hemo = blood)
It directly filters the patient blood by removing
wastes and excess electrolytes and fluid.
Then returning the cleansed blood to the patient.
Blood removed from the body is delivered to
Hemodialyzer (Artificial kidney)
A special solution dialysate is pumped into the
Hemodialyzer
37
38. Remove wastes from the blood for example –
urea
creatinine
uric acid
Excess phosphate
potassium
sulphate ions
Add needed substances glucose and Bicarbonate ions
An Anticoagulant Heparin is added to prevent blood from
clotting in The Hemodialyzer.
Most people require 6-12 hrs a week
38
39. 2) Peritoneal dialysis
In this peritoneum of abdominal cavity is used as dialysis
membrane to filter the blood.
The peritoneum has large surface area, and numerous
blood vessels and so it is very effective filter.
A catheter is inserted into peritoneal cavity and connected
to a bag of dialysate.
The fluid flows into peritoneal cavity by gravity and left
their for sufficient time to permit washes and excess
electrolytes and fluid to diffuse into dialysate.
Then the dialysate is drained into a bag, discarded and
replaced by fresh dialysate.
39