The document discusses abnormal posture in respiratory conditions and outlines physiotherapy management strategies. It highlights common postures such as forward head posture, thoracic kyphosis, and scoliosis, along with their effects on respiratory function and treatment goals. Treatment interventions aim to improve postural alignment, strength, mobility, and patient education to enhance respiratory health.
![Abnormal Posture In Respiratory
Conditions And Its
Physiotherapy Management
Presenter:- Rekha Marbate [1ST MPT]
1](https://image.slidesharecdn.com/abnormalpostureinrs-180714161659/75/Abnormal-posture-in-rs-1-2048.jpg)


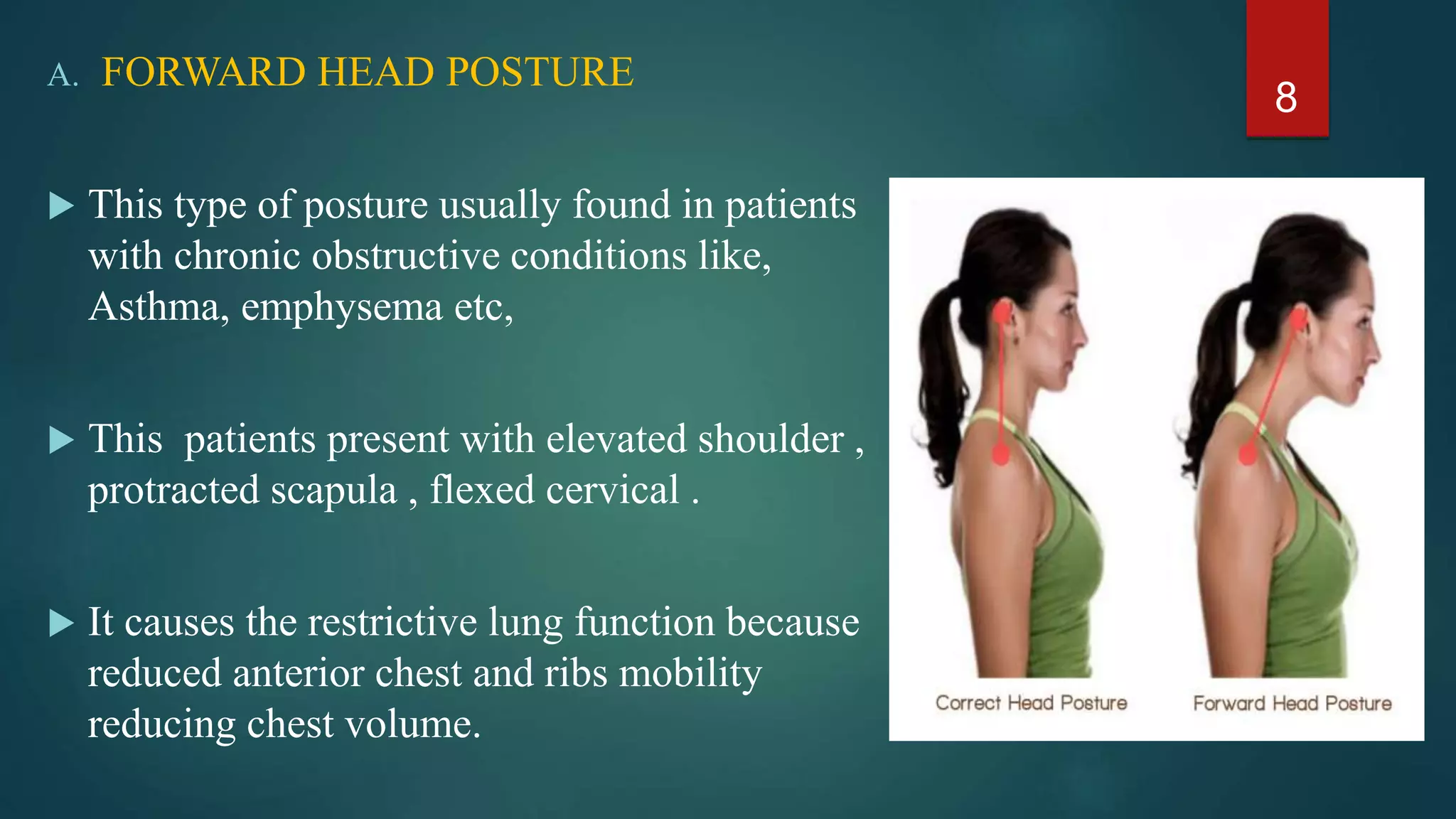
![Effect on respiratory function 7
Reduced anterior chest expansion
Rib approximation impaired pump handle mechanism.
Reduced chest volume
Reduced Total lung capacity
Jintae Han et al [2016]
Effects of poor head and thoracic posture on forced vital capacity and respiratory
muscles activity.
• FVC and FEV1 - in the forward head posture group than in the normal group.
• Accessory respiratory muscle activity was also lower .
• In particular, SCM and pectoralis major activity](https://image.slidesharecdn.com/abnormalpostureinrs-180714161659/75/Abnormal-posture-in-rs-7-2048.jpg)


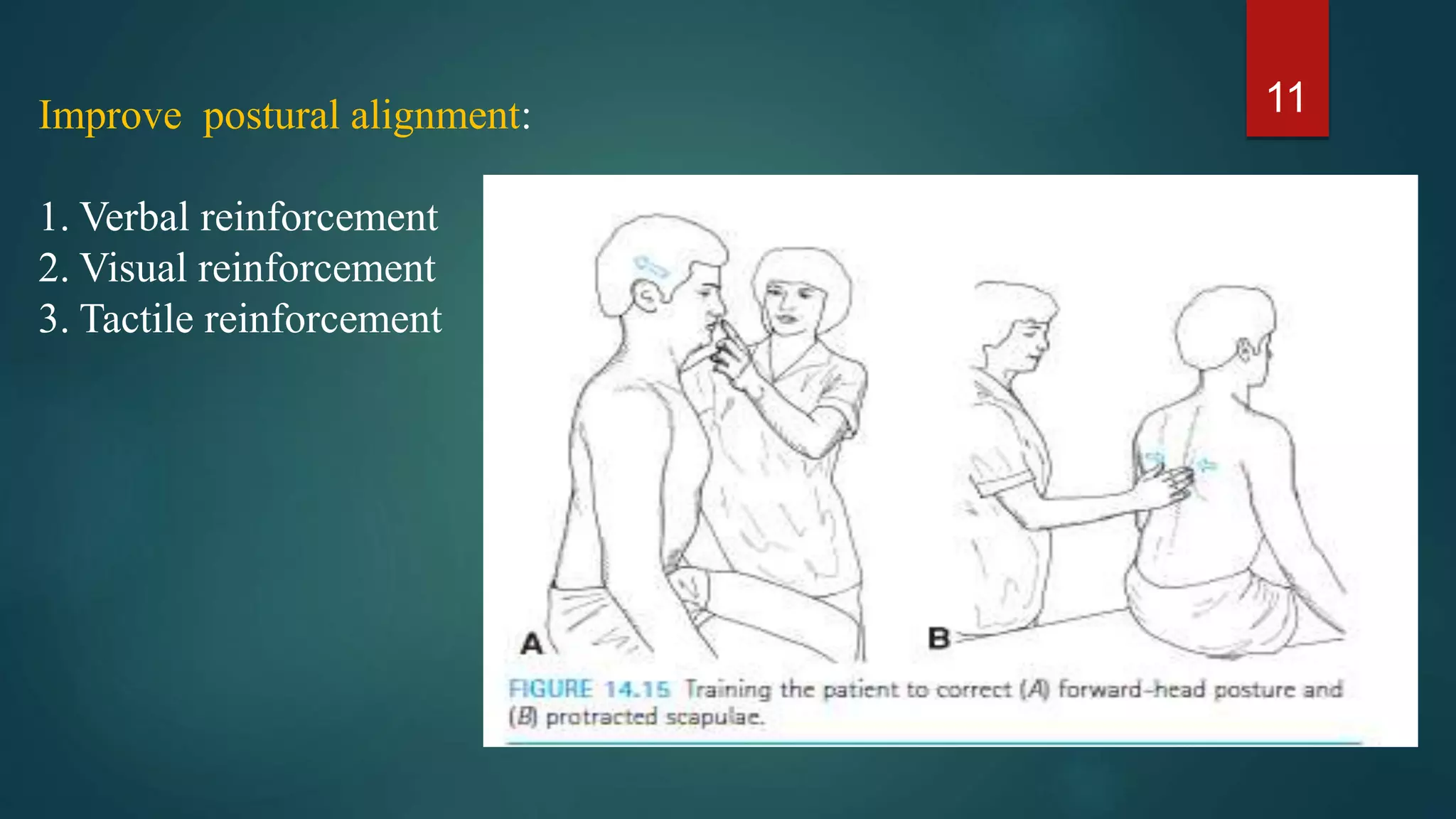

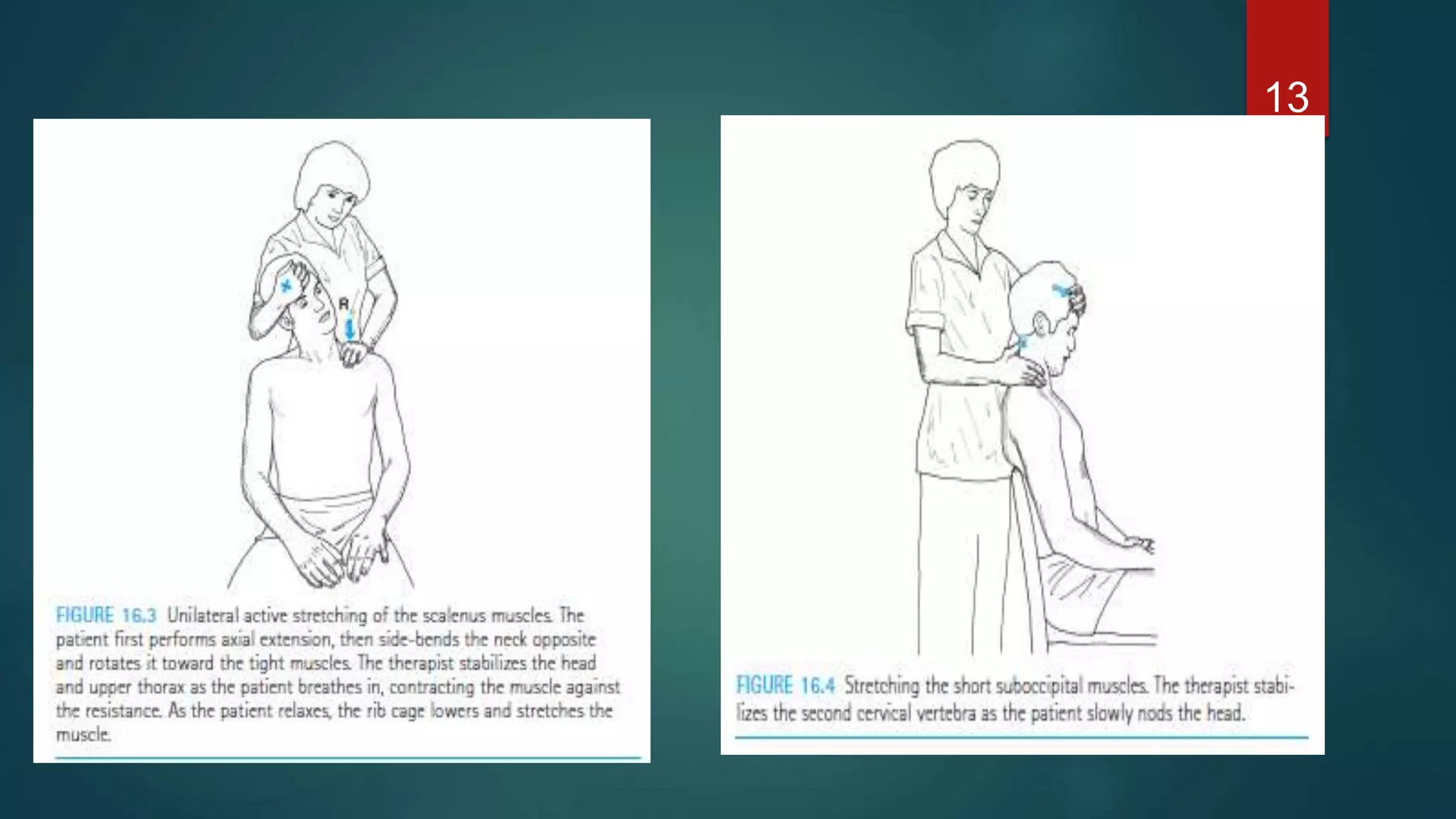


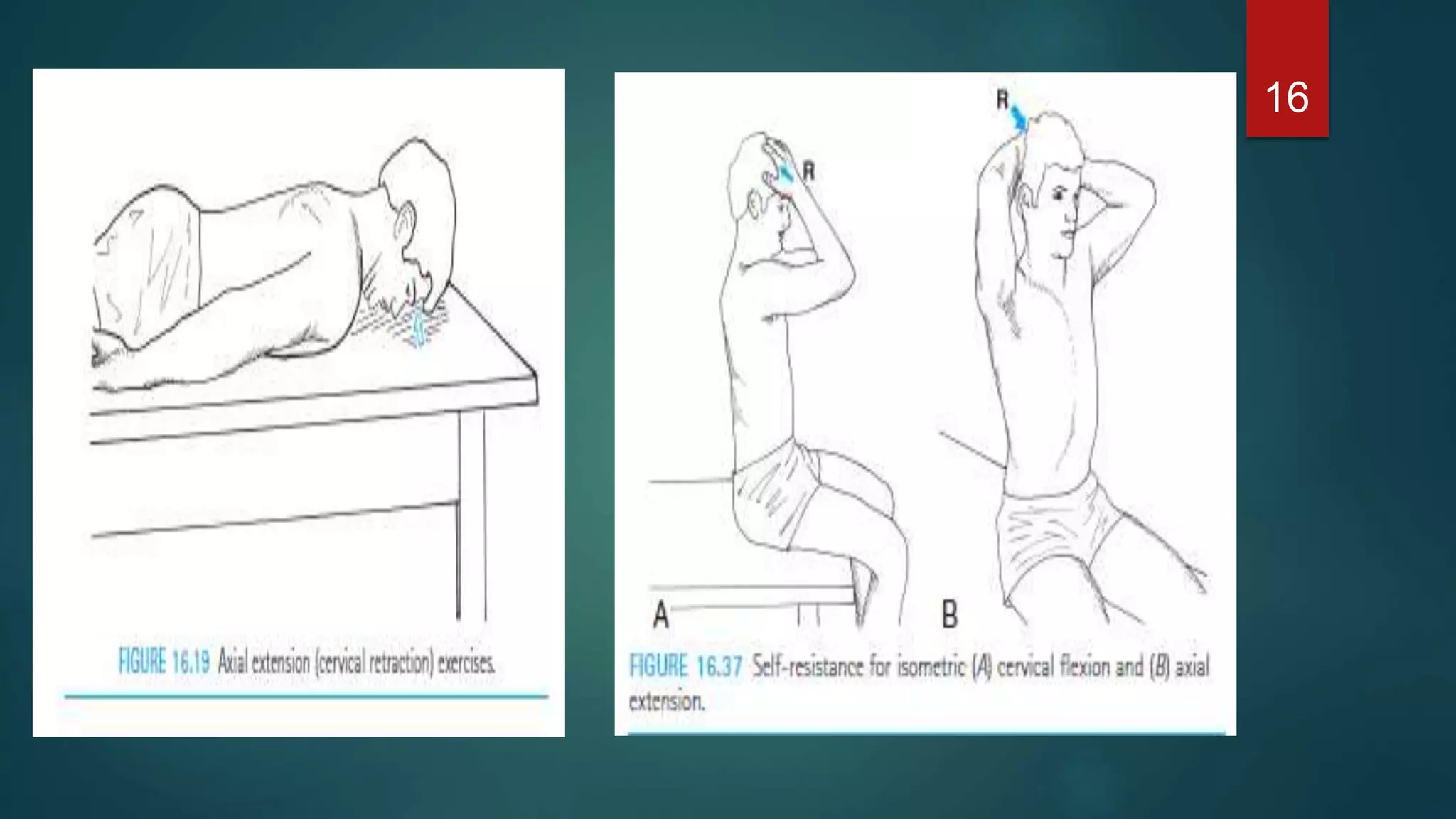






![Physiotherapy treatment
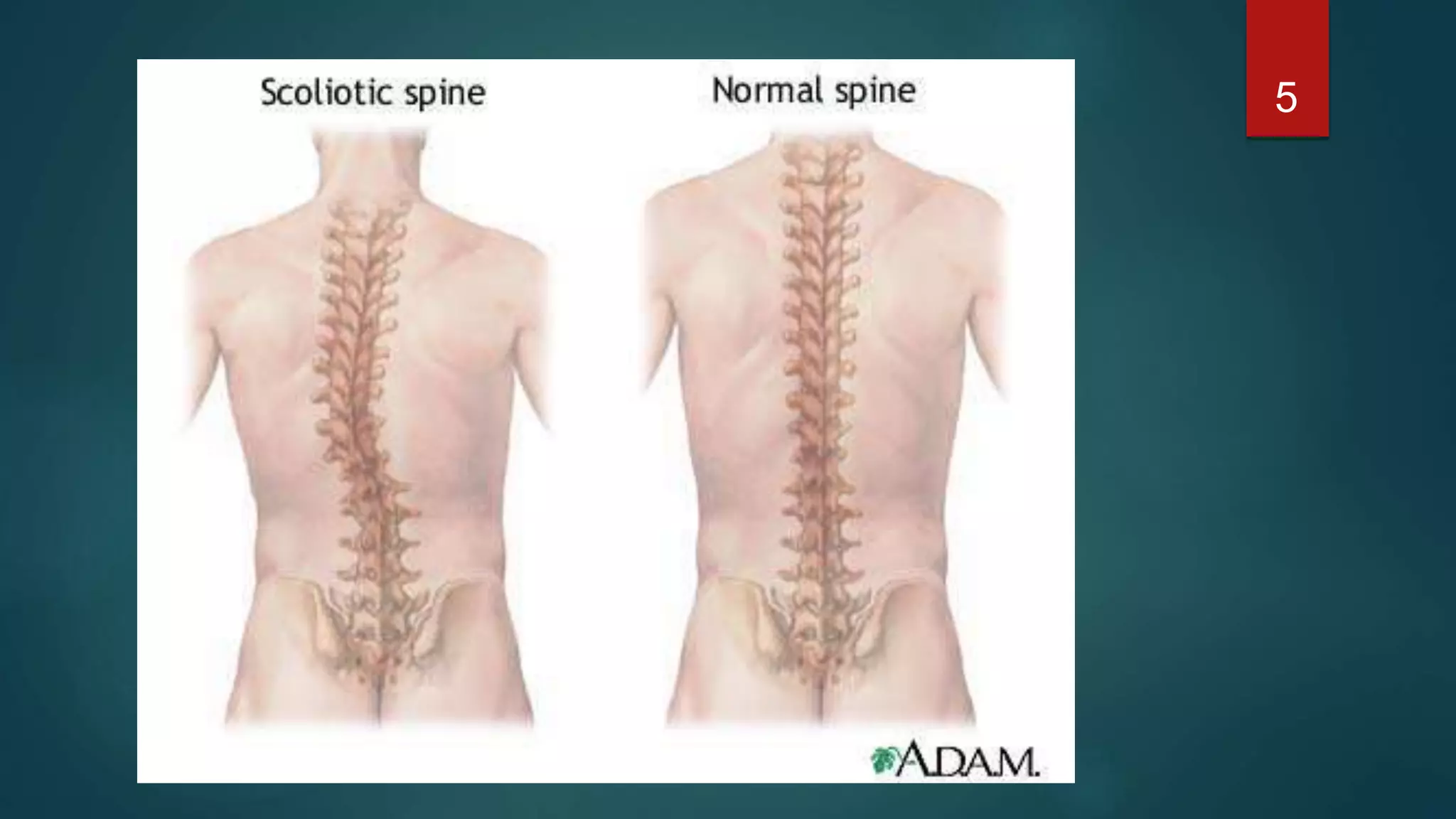
Physiotherapeutic Scoliosis Specific Exercises [ PSSE ]
Scoliosis is a complex three-dimensional (3D) spinal deformity.
Acquired scoliosis in early childhood may progress into
adulthood and pose an increased risk of health problems and
reduction in quality of life.
25](https://image.slidesharecdn.com/abnormalpostureinrs-180714161659/75/Abnormal-posture-in-rs-25-2048.jpg)















































![Waves Ultimate 15 v24.11.17 With Crack for MacOS [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409210017-8d703091-thumbnail.jpg?width=640&height=640&fit=bounds)


![CyberLink PhotoDirector Ultra Crack Free Download [Latest] 2025](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409211238-0f15f8fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![Freemake Video Converter Crack + Serial Key [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409205402-3ea828f6-thumbnail.jpg?width=640&height=640&fit=bounds)







![PT management in CKD [Renal Rehabilitation].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptmanagementinckdrenalrehabilitation-220727071020-ee721238-thumbnail.jpg?width=640&height=640&fit=bounds)



































