Downloaded 104 times

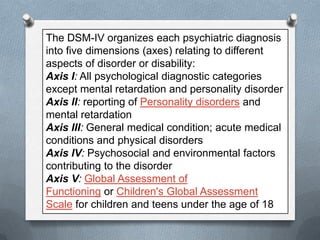
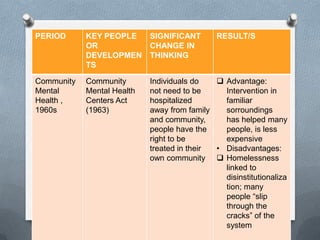
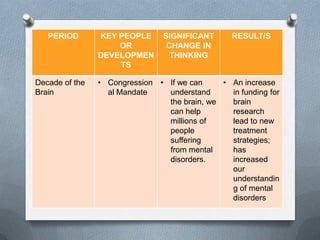
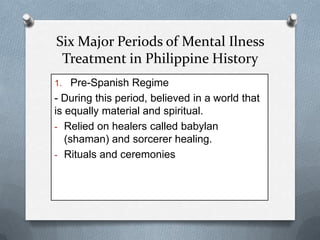
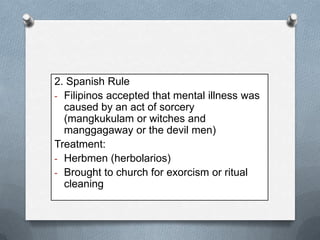

The document discusses the history and development of mental health and psychiatric nursing in the Philippines. It provides statistics on the distribution of mental health diagnoses across different facility types in the Philippines. It then covers topics such as the definition of mental health, factors influencing mental health, criteria for diagnosing mental disorders, the DSM-IV classification system, and the role of the psychiatric nurse. Finally, it discusses major periods in the history of mental illness treatment in the Philippines and benchmarks in the development of psychiatric nursing education.































![Stress & crisis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/stresscrisiscompatibilitymode-120712052718-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

















![mental_health_4[1]......... portreiz-1.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mentalhealth41portreiz-1-240426131223-b0451959-thumbnail.jpg?width=640&height=640&fit=bounds)
































