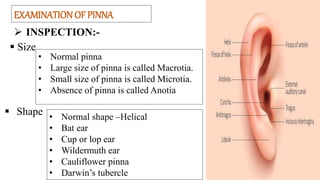
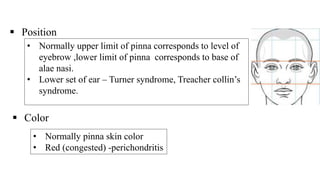
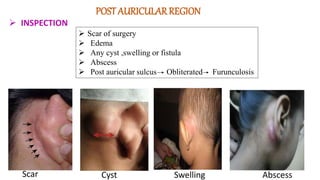
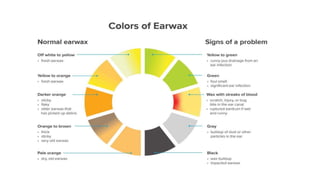
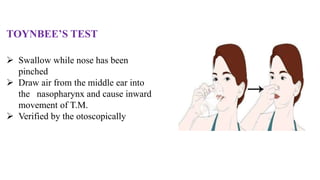
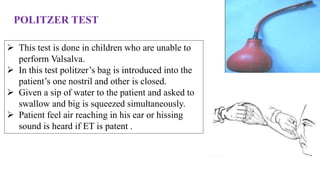
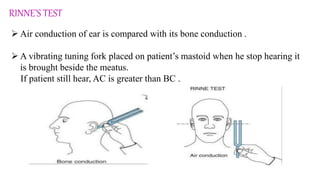
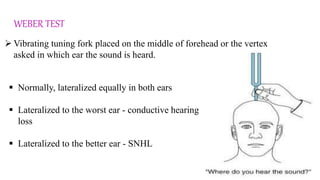
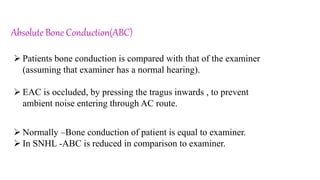
This document provides information on examining the ear. It discusses examining different parts of the ear including the pinna, external auditory canal, tympanic membrane, and eustachian tube. It outlines what to inspect and palpate for each area as well as common abnormalities. Functional examination of hearing is also described including voice testing, Rinne's test, Weber test, and bone conduction tests to evaluate air and bone conduction. The goal of examination is to evaluate for symptoms of pain, discharge, hearing loss and determine if any anatomical abnormalities or functional hearing issues exist.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






