BLOOD TRANSFUSIONS ARE ASSOCIATED WITH MORTALITY IN PEDIATRIC PATIENTS WITH SYSTOLIC HEART FAILURE – A MULTI-INSTITUTIONAL ANALYSIS - PCICS 2018
•Download as PPT, PDF•
2 likes•87 views

Restrictive thresholds for red blood cell (RBC) transfusion have not been shown to be inferior to liberal transfusion thresholds after cardiac surgery in pediatric or adult patients.1,2 RBC transfusions are associated with readmission due to heart failure (HF) in adults after aortic valve replacements, and with increased risk of right ventricle-pulmonary artery conduit failure in pediatric patients.3,4 Data are limited about RBC transfusions in pediatric patients with HF.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to BLOOD TRANSFUSIONS ARE ASSOCIATED WITH MORTALITY IN PEDIATRIC PATIENTS WITH SYSTOLIC HEART FAILURE – A MULTI-INSTITUTIONAL ANALYSIS - PCICS 2018
Similar to BLOOD TRANSFUSIONS ARE ASSOCIATED WITH MORTALITY IN PEDIATRIC PATIENTS WITH SYSTOLIC HEART FAILURE – A MULTI-INSTITUTIONAL ANALYSIS - PCICS 2018 (20)
More from Texas Children's Hospital
More from Texas Children's Hospital (14)
Recently uploaded
Recently uploaded (20)
BLOOD TRANSFUSIONS ARE ASSOCIATED WITH MORTALITY IN PEDIATRIC PATIENTS WITH SYSTOLIC HEART FAILURE – A MULTI-INSTITUTIONAL ANALYSIS - PCICS 2018
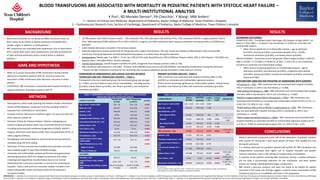
- 1. • Medical admissions comprised nearly half of the admissions of pediatric patients with systolic HF during the 5 year study period. Of these, 65% needed ICU care during the admission. • In a medical admission of a pediatric patient with systolic HF, RBC transfusion was independently associated with higher risk of hospital mortality and greater resource utilization, even in the setting of multiple other comorbidities. • A majority of the patients receiving RBC transfusion during a medical admission did not have a documented indication for the transfusion, and were neither anemic nor having a bleeding/hemorrhagic complication. • RBC remain a precious resource and were not found to be helpful for patient outcomes in this study. Our findings suggest a need for closer examination of RBC transfusion practice as a modifiable risk factor in this population. BLOOD TRANSFUSIONS ARE ASSOCIATED WITH MORTALITY IN PEDIATRIC PATIENTS WITH SYSTOLIC HEART FAILURE – A MULTI-INSTITUTIONAL ANALYSIS BACKGROUND K Puri1 , RD Morales Demori1 , PA Checchia1 , Y Wang2 , MM Anders1 1 – Section of Critical Care Medicine, Department of Pediatrics, Baylor College of Medicine, Texas Children’s Hospital; 2 – Cardiovascular Research Core, Section of Cardiology, Department of Pediatrics, Baylor College of Medicine, Texas Children’s Hospital CONCLUSIONS • Restrictive thresholds for red blood cell (RBC) transfusion have not been shown to be inferior to liberal transfusion thresholds after cardiac surgery in pediatric or adult patients.1,2 • RBC transfusions are associated with readmission due to heart failure (HF) in adults after aortic valve replacements, and with increased risk of right ventricle-pulmonary artery conduit failure in pediatric patients.3,4 • Data are limited about RBC transfusions in pediatric patients with HF. METHODS • Retrospective cohort study querying the Pediatric Health Information System (PHIS) database, comprised of 50 free-standing children’s hospitals from 01/01/2012 to 12/31/2017. • Inclusion Criteria: Admissions of patients aged < 21 years (yr) with ICD- 9/10 codes for systolic HF. • Exclusion Criteria for Primary Analysis: Patients undergoing any invasive surgical procedure which may necessitate blood transfusion, including extracorporeal membrane oxygenation (ECMO), RACHS-1 surgery, ventricular assist device (VAD), heart transplantation (HTx), or other surgeries (Others). • Demographic and clinical features and procedures during admission reviewed using ICD-9/10 coding. • Outcomes: Primary outcome was mortality and secondary outcomes were hospital length of stay (LOS) and billed charges. • Univariate and multivariable analyses performed using generalized estimating equations (GEE) for categorical outcomes and mixed modeling (with logarithmic transformation due to non-normal distribution) for continuous outcomes, to account for clustering by hospitals - factors with p<0.2 on univariate analysis included in the initial multivariable model, and factors with p<0.05 retained in successive models. RESULTS AIMS AND HYPOTHESIS • AIMS: (i) To assess the burden of RBC transfusions during medical admissions of pediatric patients with HF, and (ii) to assess the association of RBC transfusions with admission outcomes in these patients. • HYPOTHESIS: RBC transfusion is associated with hospital mortality in medical admissions of pediatric patients with HF. • 10,798 patients met initial inclusion criteria - 726 underwent HTx, 504 underwent VAD (without HTx), 1781 underwent RACHS-1 surgery (without VAD or HTx), 188 underwent ECMO (without HTx or VAD or RACHS-1 surgery), and 3036 underwent other surgical procedures (excluding cardiac or ECMO) were excluded • 4,563 medical admissions included in the primary analysis. • Separate exploratory analysis performed for the groups with surgical interventions. This was limited by inability to differentiate if they received RBC transfusion during perioperative period/cardiopulmonary bypass or at other times during the admission. • Demographics: Median age: 3 yr (IQR 0 – 13 yr), Sex: 54% (2,473) male; Race/Ethnicity: 45% (2,042)non-Hispanic white, 26% (1,162) Hispanic, 15% (683) non- Hispanic Black, 13% (585) Others, 2% (91) unknown. • Clinical Characteristics: overall hospital mortality 5% (244). Congenital heart disease present in 60% (2,756). • RBC transfusion administered in 11% (481). Of these, 41% (198/481) were anemic and 10% (49/481) had bleeding complications during the admission. • Reason for RBC transfusion uncertain for the remaining cases (surgical indications already excluded in initial selection criteria). TABLE 1. COMPARISON OF DEMOGRAPHIC AND CLINICAL FEATURES BETWEEN TRANSFUSED AND NON-TRANSFUSED GROUPS CLINICAL FEATURES TRANSFUSED (n=554) NON-TRANSFUSED (n=4417) p-value Age in years, median (IQR) 0 (0 – 8) 3 (0 – 13) <0.001 Male Sex, n (%) 260 (47) 2213 (50) 0.947 Anemia, n (%) 198 (36) 546 (12) <0.001 Bleeding, n (%) 49 (9) 435 (10) 0.752 Congenital Heart Disease, n (%) 303 (55) 2453 (56) 0.219 Concomitant Diastolic HF, n (%) 233 (42) 1829 (41) 0.130 Kidney Failure, n (%) 137 (25) 691 (16) <0.001 Liver Failure, n (%) 22 (4) 71 (2) <0.001 Mechanical Ventilation, n (%) 323 (58) 1025 (23) <0.001 ICU Admission, n (%) 427 (77) 2527 (57) <0.001 Length of Stay in ICU in days, median (IQR) 7 (2 – 14) 2 (0 – 6) <0.001 Risk of Mortality Score, n (%) <0.001 Major or Severe 423 (88) 2591 (66) Minor or Moderate 58 (12) 1491 (34) OUTCOMES Mortality, n (%) 68 (12) 176 (4) <0.001 Length of Stay in days, median (IQR) 16 (8 – 29) 7 (3 – 13) <0.001 Billed Charges (US Dollars), median (IQR) 358,215 (154,020 – 773,283) 90,857 (37,092 – 234,170) <0.001 TABLE 2. UNIVARIATE AND MULTIVARIABLE ANALYSIS FOR PRIMARY OUTCOME CHARACTERISTIC DEATH (N=244) SURVIVED (N=4319) p-value uni p-value multi# OR (95% CI) Age in years, median (IQR) 2 (0 – 13.0) 3 (0 – 13.0) 0.967 Male Sex, n (%) 124 (51) 2349 (54) 0.280 Race/Ethnicity, n (%)@ Non-Hispanic White 92 (38) 1950 (45) Ref Ref Hispanic 78 (32) 1084 (25) 0.008 0.010 1.57 (1.12 – 2.20) Non-Hispanic Black 33 (14) 650 (15) 0.726 0.219 Others 41 (17) 635 (15) 0.533 0.686 RBC transfusion, n (%) 68 (28) 413 (10) <0.001 0.014 1.55 (1.09 – 2.19) Anemia, n (%) 57 (23) 687 (16) 0.002 Bleeding Complications, n (%) 33 (14) 451 (10) 0.127 Congenital Heart Disease, n (%) 145 (59) 2611 (60) 0.749 Concomitant Diastolic HF, n (%) 112 (46) 1950 (45) 0.814 Kidney Failure, n (%) 118 (48) 710 (16) <0.001 <0.001 3.05 (2.28 – 4.07) Liver Failure, n (%) 22 (9) 71 (2) <0.001 <0.001 2.83 (1.67 – 4.80) Mechanical Ventilation, n (%) 199 (82) 1149 (27) <0.001 <0.001 10.68 (7.43 – 15.35) SECONDARY OUTCOMES: •LENGTH OF STAY - Transfused cohort had longer LOS (median 16 days (IQR 8 – 29 days) vs 7 days (IQR 3 – 13 days) in non-transfused, p < 0.001) on univariate and multivariable analysis. • Other factors significant on multivariable analysis – age at admission (p=0.027), anemia (p<0.001), concomitant diastolic HF (p = 0.039), mechanical ventilation (p<0.001), and kidney failure (p<0.001). •BILLED CHARGES - Transfused cohort had greater billed charges (median $ 358,215 (IQR $ 154,020 – $ 773,283) vs $ 90,857 ($ 37,092 – $ 234,170) in non-transfused, p<0.001) on univariate and multivariable analysis. • Other factors remaining significant on multivariable analysis – age at admission (p<0.001), race/ethnicity (p<0.001), congenital heart disease (p<0.001), anemia (p<0.001), mechanical ventilation (p<0.001), and kidney failure (p<0.001). PRIMARY OUTCOME ANALYSIS - TABLE 2: •RBC transfusion was associated with hospital mortality (28% vs 10%, p<0.001) on univariate and multivariable regression analysis. •Other factors remaining significant on multivariable analysis - kidney failure (p<0.001), liver failure (p<0.001) and mechanical ventilation (p<0.001). RESULTS REFERENCES: 1 – Shehata N et al. Restrictive compared with liberal red cell transfusion strategies in cardiac surgery: a meta-analysis. Eur Heart J. 2018 Aug 10; 2 - Cholette J et al. Recommendations on RBC Transfusion in Infants and Children With Acquired and Congenital Heart Disease From the Pediatric Critical Care Transfusion and Anemia Expertise Initiative. Pediatr Crit Care Med. 2018 Sep;19(9S Suppl 1):S137-S148; 3 - Durand E et al. Incidence, Prognostic Impact, and Predictive Factors of Readmission for Heart Failure After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2017 Dec 11;10(23):2426-2436; 4 - Therrien J et al. Repeated blood transfusions: Identification of a novel culprit of early graft failure in children. Int J Cardiol. 2018 Mar 1;254:90-95. Ref: reference Factors included in initial regression model – all with p<0.2; Factors in final regression model: race/ethnicity, kidney failure, liver failure, RBC transfusion, mechanical ventilation EXPLORATORY ANALYSIS FOR PEDIATRIC HF ADMISSIONS WITH SURGERY: •HTx group (n = 726) – RBC transfusion was not associated with hospital mortality (4% in transfused, vs 2.8% in non-transfused, p = 0.388). •VAD without HTx group (n = 188) – RBC transfusion was not associated with hospital mortality (38% in transfused vs 31% in non-transfused, p = 0.287). •RACHS-1 surgery without VAD or HTx group (n = 1781) – RBC transfusion was associated with mortality on univariate and multivariable analysis (6.2% vs 3.1%, p = 0.003, OR 2.33, 95% CI 1.34 – 4.06). •ECMO without VAD or HTx or RACHS-1 surgery group (n = 504) - RBC transfusion was not associated with hospital mortality (42% in transfused vs 39% in non- transfused, p = 0.569). •Other surgical procedures group (n = 3036) – RBC transfusion was associated with hospital mortality on univariate but NOT on multivariable regression analysis (6.2% vs 3.2%, p = 0.083 on multivariable analysis, OR 1.41, 95% CI 0.96 – 2.07). COMPARISON OF DEMOGRAPHIC AND CLINICAL FEATURES BETWEEN TRANSFUSED AND NOT-TRANSFUSED COHORTS – TABLE 1: •Compared to the non-transfused group, the transfused group was younger (p < 0.001), and more likely to have clinical comorbidities - including anemia (p<0.001), kidney failure (p<0.001), liver failure (p<0.001), and mechanical ventilation (p<0.001).
Editor's Notes
- LOS – age p =0.001, mech vent – p &lt;0.001, anemia p&lt;0.001, kidney failure p&lt;0.001, pRBC p&lt;0.001, OR 7.37, 95% CI 4.3 to 7.4