Characteristics and Outcomes of Pediatric Patients supported with Ventricular Assist Device - A multi institutional analysis

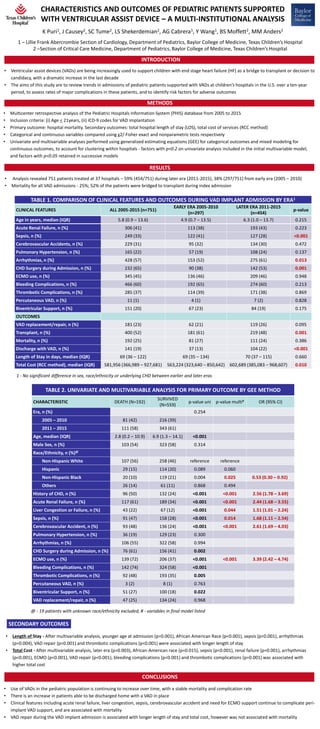
Ventricular assist devices (VADs) are being increasingly used to support children with end stage heart failure (HF) as a bridge to transplant or decision to candidacy, with a dramatic increase in the last decade The aims of this study are to review trends in admissions of pediatric patients supported with VADs at children’s hospitals in the U.S. over a ten-year period, to assess rates of major complications in these patients, and to identify risk factors for adverse outcomes Multicenter retrospective analysis of the Pediatric Hospitals Information System (PHIS) database from 2005 to 2015 Inclusion criteria: (i) Age < 21years, (ii) ICD-9 codes for VAD implantation Primary outcome: hospital mortality. Secondary outcomes: total hospital length of stay (LOS), total cost of services (RCC method) Categorical and continuous variables compared using χ2/ Fisher exact and nonparametric tests respectively Univariate and multivariable analyses performed using generalized estimating equations (GEE) for categorical outcomes and mixed modeling for continuous outcomes, to account for clustering within hospitals - factors with p<0.2 on univariate analysis included in the initial multivariable model, and factors with p<0.05 retained in successive models Use of VADs in the pediatric population is continuing to increase over time, with a stable mortality and complication rate There is an increase in patients able to be discharged home with a VAD in place Clinical features including acute renal failure, liver congestion, sepsis, cerebrovascular accident and need for ECMO support continue to complicate peri-implant VAD support, and are associated with mortality VAD repair during the VAD implant admission is associated with longer length of stay and total cost, however was not associated with mortality
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Characteristics and Outcomes of Pediatric Patients supported with Ventricular Assist Device - A multi institutional analysis
Similar to Characteristics and Outcomes of Pediatric Patients supported with Ventricular Assist Device - A multi institutional analysis (20)
More from Texas Children's Hospital
More from Texas Children's Hospital (16)
Recently uploaded
Recently uploaded (20)
Characteristics and Outcomes of Pediatric Patients supported with Ventricular Assist Device - A multi institutional analysis
- 1. CHARACTERISTICS AND OUTCOMES OF PEDIATRIC PATIENTS SUPPORTED WITH VENTRICULAR ASSIST DEVICE – A MULTI-INSTITUTIONAL ANALYSIS BACKGROUND • Ventricular assist devices (VADs) are being increasingly used to support children with end stage heart failure (HF) as a bridge to transplant or decision to candidacy, with a dramatic increase in the last decade • The aims of this study are to review trends in admissions of pediatric patients supported with VADs at children’s hospitals in the U.S. over a ten-year period, to assess rates of major complications in these patients, and to identify risk factors for adverse outcomes 1 – Lillie Frank Abercrombie Section of Cardiology, Department of Pediatrics, Baylor College of Medicine, Texas Children’s Hospital 2 –Section of Critical Care Medicine, Department of Pediatrics, Baylor College of Medicine, Texas Children’s Hospital CONCLUSIONS 1 - No significant difference in sex, race/ethnicity or underlying CHD between earlier and later eras METHODS • Multicenter retrospective analysis of the Pediatric Hospitals Information System (PHIS) database from 2005 to 2015 • Inclusion criteria: (i) Age < 21years, (ii) ICD-9 codes for VAD implantation • Primary outcome: hospital mortality. Secondary outcomes: total hospital length of stay (LOS), total cost of services (RCC method) • Categorical and continuous variables compared using χ2/ Fisher exact and nonparametric tests respectively • Univariate and multivariable analyses performed using generalized estimating equations (GEE) for categorical outcomes and mixed modeling for continuous outcomes, to account for clustering within hospitals - factors with p<0.2 on univariate analysis included in the initial multivariable model, and factors with p<0.05 retained in successive models @ - 19 patients with unknown race/ethnicity excluded, # - variables in final model listed RESULTS INTRODUCTION TABLE 1. COMPARISON OF CLINICAL FEATURES AND OUTCOMES DURING VAD IMPLANT ADMISSION BY ERA1 CLINICAL FEATURES ALL 2005-2015 (n=751) EARLY ERA 2005-2010 (n=297) LATER ERA 2011-2015 (n=454) p-value Age in years, median (IQR) 5.8 (0.9 – 13.6) 4.9 (0.7 – 13.5) 6.3 (1.0 – 13.7) 0.215 Acute Renal Failure, n (%) 306 (41) 113 (38) 193 (43) 0.223 Sepsis, n (%) 249 (33) 122 (41) 127 (28) <0.001 Cerebrovascular Accidents, n (%) 229 (31) 95 (32) 134 (30) 0.472 Pulmonary Hypertension, n (%) 165 (22) 57 (19) 108 (24) 0.137 Arrhythmias, n (%) 428 (57) 153 (52) 275 (61) 0.013 CHD Surgery during Admission, n (%) 232 (65) 90 (38) 142 (53) 0.001 ECMO use, n (%) 345 (45) 136 (46) 209 (46) 0.948 Bleeding Complications, n (%) 466 (60) 192 (65) 274 (60) 0.213 Thrombotic Complications, n (%) 285 (37) 114 (39) 171 (38) 0.869 Percutaneous VAD, n (%) 11 (1) 4 (1) 7 (2) 0.828 Biventricular Support, n (%) 151 (20) 67 (23) 84 (19) 0.175 OUTCOMES VAD replacement/repair, n (%) 181 (23) 62 (21) 119 (26) 0.095 Transplant, n (%) 400 (52) 181 (61) 219 (48) 0.001 Mortality, n (%) 192 (25) 81 (27) 111 (24) 0.386 Discharge with VAD, n (%) 141 (19) 37 (13) 104 (22) <0.001 Length of Stay in days, median (IQR) 69 (36 – 122) 69 (35 – 134) 70 (37 – 115) 0.660 Total Cost (RCC method), median (IQR) 581,956 (366,989 – 927,681) 563,224 (323,640 – 850,642) 602,689 (385,083 – 968,607) 0.010 TABLE 2. UNIVARIATE AND MULTIVARIABLE ANALYSIS FOR PRIMARY OUTCOME BY GEE METHOD CHARACTERISTIC DEATH (N=192) SURVIVED (N=559) p-value uni p-value multi# OR (95% CI) Era, n (%) 0.254 2005 – 2010 81 (42) 216 (39) 2011 – 2015 111 (58) 343 (61) Age, median (IQR) 2.8 (0.2 – 10.9) 6.9 (1.3 – 14.1) <0.001 Male Sex, n (%) 103 (54) 323 (58) 0.314 Race/Ethnicity, n (%)@ Non-Hispanic White 107 (56) 258 (46) reference reference Hispanic 29 (15) 114 (20) 0.089 0.060 Non-Hispanic Black 20 (10) 119 (21) 0.004 0.025 0.53 (0.30 – 0.92) Others 26 (14) 61 (11) 0.868 0.494 History of CHD, n (%) 96 (50) 132 (24) <0.001 <0.001 2.56 (1.78 – 3.69) Acute Renal Failure, n (%) 117 (61) 189 (34) <0.001 <0.001 2.44 (1.68 – 3.55) Liver Congestion or Failure, n (%) 43 (22) 67 (12) <0.001 0.044 1.51 (1.01 – 2.24) Sepsis, n (%) 91 (47) 158 (28) <0.001 0.014 1.68 (1.11 – 2.54) Cerebrovascular Accident, n (%) 93 (48) 136 (24) <0.001 <0.001 2.61 (1.69 – 4.03) Pulmonary Hypertension, n (%) 36 (19) 129 (23) 0.300 Arrhythmias, n (%) 106 (55) 322 (58) 0.994 CHD Surgery during Admission, n (%) 76 (61) 156 (41) 0.002 ECMO use, n (%) 139 (72) 206 (37) <0.001 <0.001 3.39 (2.42 – 4.74) Bleeding Complications, n (%) 142 (74) 324 (58) <0.001 Thrombotic Complications, n (%) 92 (48) 193 (35) 0.005 Percutaneous VAD, n (%) 3 (2) 8 (1) 0.763 Biventricular Support, n (%) 51 (27) 100 (18) 0.022 VAD replacement/repair, n (%) 47 (25) 134 (24) 0.968 • Use of VADs in the pediatric population is continuing to increase over time, with a stable mortality and complication rate • There is an increase in patients able to be discharged home with a VAD in place • Clinical features including acute renal failure, liver congestion, sepsis, cerebrovascular accident and need for ECMO support continue to complicate peri- implant VAD support, and are associated with mortality • VAD repair during the VAD implant admission is associated with longer length of stay and total cost, however was not associated with mortality K Puri1, J Causey2, SC Tume2, LS Shekerdemian2, AG Cabrera1, Y Wang1, BS Moffett2, MM Anders2 • Analysis revealed 751 patients treated at 37 hospitals – 59% (454/751) during later era (2011-2015), 38% (297/751) from early era (2005 – 2010) • Mortality for all VAD admissions - 25%; 52% of the patients were bridged to transplant during index admission • Length of Stay - After multivariable analysis, younger age at admission (p=0.001), African American Race (p<0.001), sepsis (p<0.001), arrhythmias (p=0.004), VAD repair (p<0.001) and thrombotic complications (p<0.001) were associated with longer length of stay • Total Cost - After multivariable analysis, later era (p=0.003), African-American race (p=0.015), sepsis (p<0.001), renal failure (p=0.001), arrhythmias (p<0.001), ECMO (p<0.001), VAD repair (p<0.001), bleeding complications (p<0.001) and thrombotic complications (p=0.001) was associated with higher total cost SECONDARY OUTCOMES