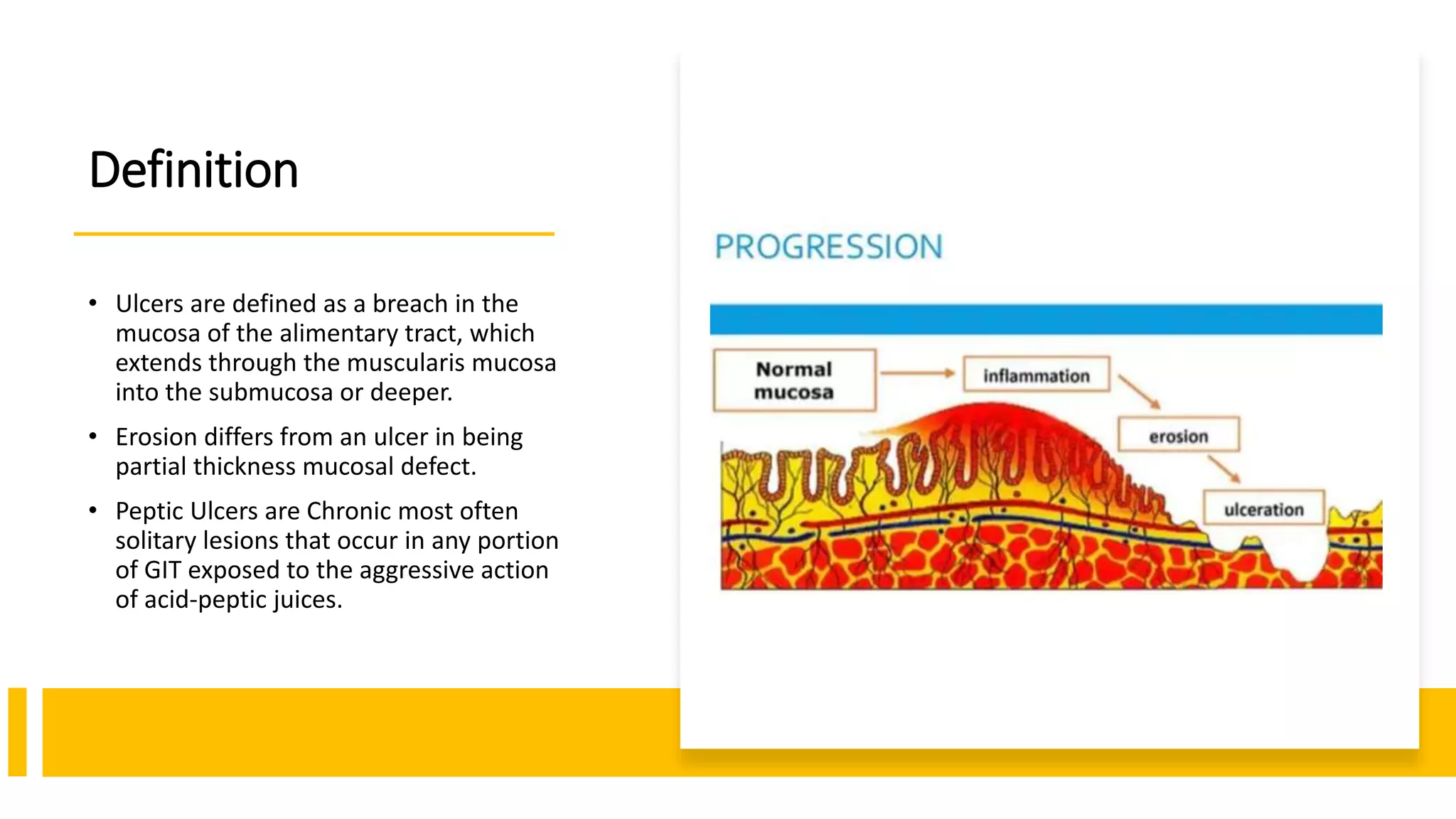
Peptic ulcer disease is defined as chronic ulcers that occur in portions of the gastrointestinal tract exposed to gastric acid and pepsin. Common causes include Helicobacter pylori infection and NSAID use.
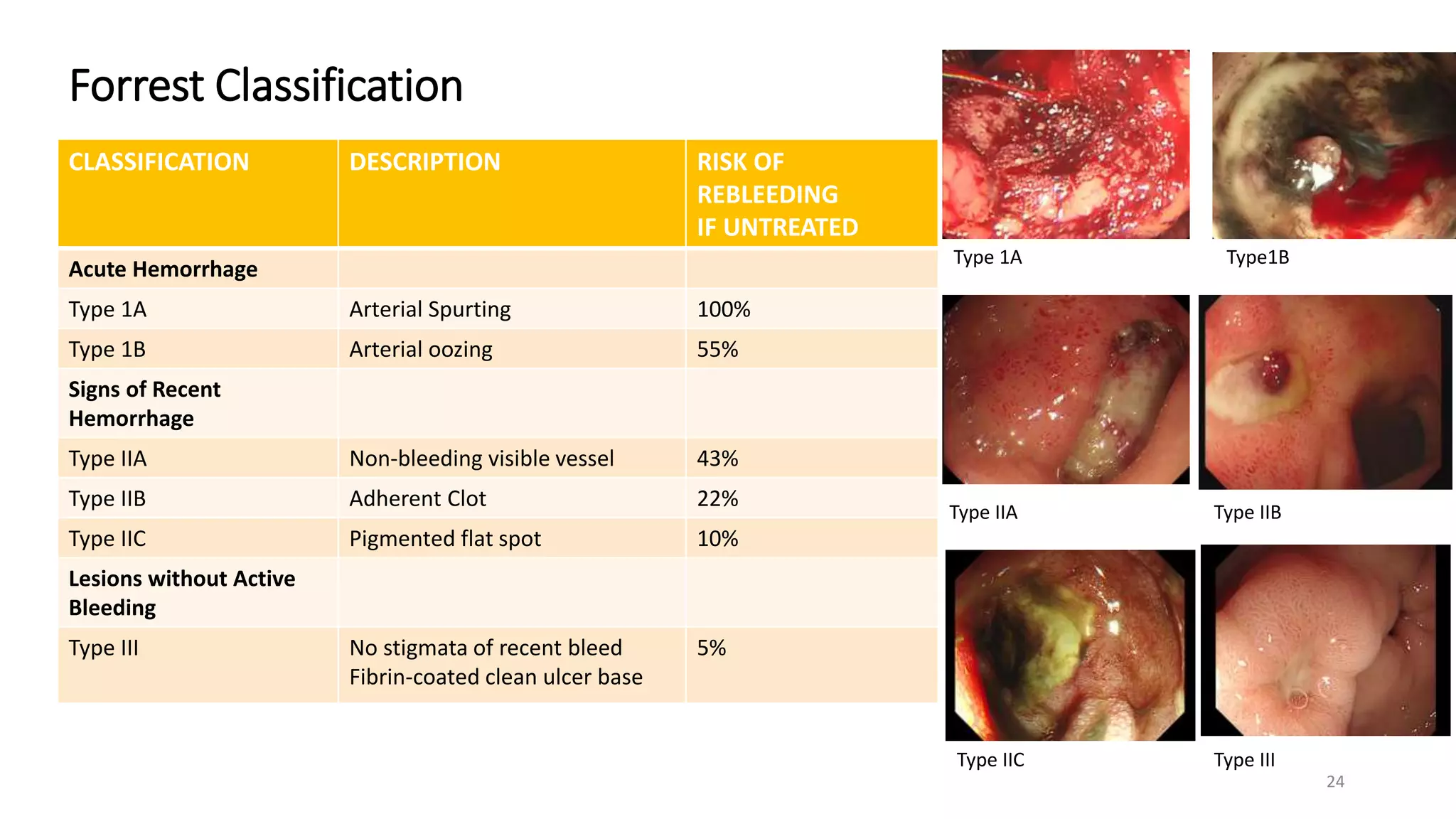
The document discusses gastric anatomy and physiology related to acid secretion. It also covers the pathogenesis of peptic ulcers involving an imbalance between aggressive and defensive factors. Diagnostics include endoscopy to visualize ulcers and test for H. pylori.
Management involves acid suppression with PPIs or H2 blockers as well as cytoprotective agents. H. pylori infection is treated with antibiotic combinations. NSAID-induced ulcers are prevented or treated with PPIs or misopro