2. relationships with adults help children gain the benefits of
instructional experiences and resources. Children who
see themselves as highly valued are more likely to feel secure,
thrive physically, get along with others, learn well,
and feel part of a community.
2. Curriculum
Program Standard: The program implements a curriculum that is
consistent with its goals for children and that
promotes learning and development in each of the following
areas: social, emotional, physical, language, and
cognitive.
Rationale: A curriculum that draws on research assists teachers
in identifying important concepts and skills as well
as effective methods for fostering children’s learning and
development. When informed by teachers’ knowledge of
individual children, a well-articulated curriculum guides
teachers so they can plan learning experiences that promote
children’s growth across a broad range of developmental and
content areas. A curriculum also helps ensure that the
teacher is intentional in planning a daily schedule that (a)
maximizes children’s acquisition of desired knowledge
and skills through the effective use of time and materials and
3. (b) offers opportunities for children to learn through
play and through structured activities, individually and in
groups, according to their developmental needs and
interests.
3. Teaching
Program Standard: The program uses a variety of
developmentally, culturally, and linguistically appropriate and
effective teaching approaches that enhance each child’s learning
and development in the context of the program’s
curriculum goals.
Rationale: Teaching staff who purposefully use multiple
instructional approaches optimize children’s opportunities
for learning. These approaches include strategies that range
from structured to unstructured and from adult directed
to child directed. Children bring to learning environments
different backgrounds, interests, experiences, learning
styles, needs, and capacities.
When selecting and implementing instructional approaches,
teachers’ consideration of these differences helps all
children learn. Instructional approaches differ in their
effectiveness for teaching different elements of curriculum and
5. teaching practices, and to drive program improvement.
Rationale: Teachers’ knowledge of each child helps them to
plan an appropriately challenging curriculum and to
tailor instruction that responds to each child’s strengths and
needs. Further, systematic assessment is essential for
identifying children who may benefit from more intensive
instruction or intervention or who may need additional
developmental evaluation. This information ensures that the
program meets its goals for children’s learning and
developmental progress as well as informs program
improvement efforts.
5. Health
Program Standard: The program promotes the nutrition and
health of children and protects children and staff from
illness.
Rationale: To benefit from education and optimize quality of
life, children need to be as healthy as possible. Health
is a state of complete physical, oral, mental, and social well -
being and not merely the absence of disease or
infirmity (World Health Organization 1948). Children depend
on adults (who also are as healthy as possible) to
6. make healthy choices for them and to teach them to make
healthy choices for themselves. Although some degree
of risk taking is desirable for learning, a quality program
prevents hazardous practices and environments that are
likely to result in adverse consequences for children, staff,
families, or communities.
6. Staff Competencies, Preparation, and Support
Program Standard: The program employs and supports a
teaching and administrative staff that have the
qualifications, knowledge, and professional commitment
necessary to promote children’s learning and development
and to support families’ diverse needs and interests.
Rationale: Children in early learning programs benefit most
when teaching and administrative staff have high levels
of formal education and specialized professional preparation.
Staff who have specific preparation, knowledge, and
skills in child development and early childhood education are
more likely to engage in warm, positive interactions
with children, offer richer language experiences, and create
higher quality learning environments. Opportunities for
teaching and administrative staff to receive supportive
supervision and to participate in ongoing professional
8. 8. Community Relationships
Program Standard: The program establishes relationships with
and uses the resources of the children’s
communities to support the achievement of program goals.
Rationale: As part of the fabric of children’s communities, an
effective program establishes and maintains
reciprocal relationships with agencies and institutions that can
support it in achieving its goals for the curriculum,
health promotion, children’s transitions, inclusion, and
diversity. By helping to connect families with needed
resources, the program furthers children’s health, development,
and learning.
9. Physical Environment
Program Standard: The program has a safe and healthful
environment that provides appropriate and well-
maintained indoor and outdoor physical environments. The
environment includes facilities, equipment, and
materials to facilitate child and staff learning and development.
Rationale: The program’s design and maintenance of its
physical environment support high-quality program
activities and services and allow for optimal use and operation.
9. Well-organized, equipped, and maintained
environments support program quality by facilitating the
learning, comfort, health, and safety of those who use the
program. Program quality is enhanced by also creating a
welcoming and accessible setting for children, families,
and staff.
10. Leadership and Management
Program Standard: The program effectively implements
policies, procedures, and systems that support stable staff
and strong personnel, fiscal, and program management so all
children, families, and staff have high-quality
experiences.
Rationale: Excellent programming requires effective leadership
and governance structures and comprehensive,
well-functioning administrative policies, procedures, and
systems. Effective leadership and management create the
environment for high-quality care and education by (a) ensuring
compliance with relevant regulations and
guidelines; (b) promoting fiscal soundness, program
accountability, effective communication, helpful consultative
services, and positive community relations; (c) maintaining
stable staff; and (d) instituting ongoing program planning
10. as well as continuous program improvement.
1Rev Bras Enferm. 2020;73(Suppl 4):
SUPPLEMENTARY EDITION 4
WOMEN'S AND CHILDREN'S HEALTH
e20190143http://dx.doi.org/10.1590/0034-7167-2019-0143 7of
ABSTRACT
Objectives: to investigate the presumption of sexual abuse
through the records of live births
with mothers up to 13 years of age. Methods: this is a
quantitative study, with an ecological
design, carried out in Maceió, with data from the Brazilian Live
Birth Information System from
2009 to 2017, based on Law 12,015/2009, on sexual crimes
against the vulnerable, applying the
presumption of violence in children under 14 years old. Results:
nine hundred fifty-three births
of children with mothers aged 10 to 13 years were recorded;
1.3% were reported as victims
of sexual abuse; 20.3% declared to be married or living in a
stable relationship. Records were
concentrated in 04 neighborhoods, Guaxuma, Benedito Bentes,
Tabuleiro do Martins, and
Jacintinho. Conclusions: there was a prevalence of pregnancy
and marriage in girls under 14
years of age and scarcity of reporting presumed sexual abuse by
11. health professionals.
Descriptors: Vulnerable Populations; Pregnancy; Nursing;
Adolescent; Child Abuse, Sexual.
RESUMO
Objetivos: investigar a presunção da violência sexual através
dos registros de nascidos
vivos com mães até 13 anos de idade. Métodos: trata-se de um
estudo quantitativo com
delineamento ecológico realizado em Maceió, com dados do
Sistema de Informação sobre
Nascidos Vivos no período de 2009 a 2017, fundamentando-se
na Lei nº 12.015/2009, sobre
crimes sexuais contra vulnerável. Aplicou-se a presunção da
violência em menor de 14 anos.
Resultados: foram registrados 953 nascimentos de crianças com
mães em idades de 10 a 13
anos; 1,3% foram notificadas como vítimas de abuso sexual;
20,3% declaram ser casadas ou
viver em união estável. Os registros concentraram-se em 04
bairros, Guaxuma, Benedito Bentes,
Tabuleiro do Martins e Jacintinho. Conclusões: constatou-se
prevalência de gestação e de
casamento em meninas com menos de 14 anos e a escassez de
notificações de abuso sexual
por presunção por parte dos profissionais de saúde.
Descritores: Populações Vulneráveis; Gravidez; Enfermagem;
Adolescente; Abuso Sexual
na Infância.
RESUMEN
Objetivos: investigar la presunción de violencia sexual a través
de los registros de nacimientos
vivos con madres de hasta 13 años. Métodos: este es un estudio
cuantitativo con un diseño
ecológico realizado en Maceió, con datos del Sistema de
12. Información sobre Nacimientos Vivos
en el período de 2009 a 2017, basado en la Ley 12.015/2009,
sobre delitos sexuales contra
personas vulnerables. Se aplican a presunción de violencia en
menores de 14 años. Resultados:
se registraron 953 nacimientos de niños con madres de entre 10
y 13 años; 1.3% se informó
como víctimas de abuso sexual; 20.3% se declaró casado o
viviendo en una relación estable.
Los registros se concentraron en 04 barrios, Guaxuma, Benedito
Bentes, Tabuleiro do Martins y
Jacintinho. Conclusiones: hubo una prevalencia de embarazo y
matrimonio en niñas menores
de 14 años y la falta de informes de abuso sexual debido a la
presunción de profesionales de
la salud.
Descriptores: Poblaciones Vulnerables; Embarazo; Enfermería;
Adolescente; Abuso Sexual
Infantil.
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Presunção do abuso sexual em crianças e adolescentes:
vulnerabilidade da gravidez antes dos 14 anos
Presunción de abuso sexual en niños y adolescentes:
vulnerabilidad del embarazo antes de 14 años
ORIGINAL ARTICLE
Ana Jéssica Cassimiro da SilvaI
ORCID: 0000-0002-0608-6015
Ruth França Cizino da TrindadeI
13. ORCID: 0000-0001-9932-6905
Larissa Lages Ferrer de OliveiraI
ORCID: 0000-0002-4071-2438
IUniversidade Federal de Alagoas. Maceió, Alagoas, Brazil.
How to cite this article:
Silva AJC, Trindade RFC, Oliveira LLF.
Presumption of sexual abuse in children and
adolescents: vulnerability of pregnancy before 14 years.
Rev Bras Enferm. 2020;73(Suppl 4):e20190143.
doi: http://dx.doi.org/10.1590/0034-7167-2019-0143
Corresponding author:
Ana Jéssica Cassimiro da Silva
E-mail: [email protected]
EDITOR IN CHIEF: Antonio José de Almeida Filho
ASSOCIATE EDITOR: Mitzy Reichembach
Submission: 05-05-2019 Approval: 02-29-2020
2Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Silva AJC, Trindade RFC, Oliveira LLF.
14. INTRODUCTION
Care for children and adolescents is based on the idea that they
are vulnerable individuals, individually and collectively,
consider-
ing that vulnerability is intrinsic to human beings, especially in
its initial phase. Their biopsychic development is under
construc-
tion, amid to a period of innocence, discovery and dependence,
which naturally make them more susceptible to situations and
contexts in which the dominance of the strongest over the weak-
est is present. Therefore, it demands comprehensive attention
for
the prevention of situations that possibly have consequences,
whether by negligence, discrimination, exploitation, violence,
cruelty or oppression(1-3).
Adolescent pregnancy is an expressive phenomenon in Brazil,
being a product of this vulnerability. It generates risks to
biological
(maternal-fetal risks), psychological (insecurity, fear) and
social
(socioeconomic compromise, family breakdown, school
dropout)
development as a result of early sexual initiation, which makes
the growing increase in the representation of children and ado-
lescents aged 10 to 14 years, in these pregnancies. Biological
and
psychological immaturity during this phase of transition
between
childhood and adulthood increase exposure to these risks(4-6).
The Brazilian judicial system recognizes children and
adolescents
under the age of 14 as a public that demands legitimate criminal
protection against any and all types of early sexual initiation to
15. which they are subjected by an adult, in view of the unpredict-
able risks to the future development of their personality and the
inability to measure the physical and psychological scars
resulting
from a decision that an adolescent or child is not yet able to
make(7).
Law 12,015/2009, which provides for heinous crimes and
includes sexual crimes against the vulnerable in this category,
establishes that performing sexual acts or performing any libidi -
nous act with or in the presence of a child under 14 is a sexual
crime against the vulnerable, regardless of consent, obeying the
legal justification that the vulnerable does not have the
necessary
discernment to practice the act, or that, for some reason, cannot
offer resistance(7).
The Brazilian legislator’s definition of the age of less than 14
years was established based on the principle “Qui velle non
potuit,
ergo noluit” (translation, “Who cannot want, does not want, who
cannot consent, dissent”). Moreover, health and human sciences
professionals define this age group as the stage in which
psycho-
physiological changes linked to sexual maturation occur.
Countries
like Germany and Italy also adopt the same age, differently
from
other countries like Argentina and Paraguay, which establ ish the
limit of 12 years as a vulnerable minor(8).
According to the Brazilian Penal Code, the vulnerability of
children under 14 does not allow relativization, regardless of
the
victim’s consent, past sexual experiences (even in cases of child
prostitution) or romantic relationship between author and
16. victim.
They are people still in cognitive, hormonal and psychological
development with regard to sexuality(2,7).
This study becomes relevant due to the need for visibility of
the vulnerability factors surrounding the under-14s, through
investigation, reception, and reporting of confirmed or
presumed
cases of sexual violence by health professionals. They will
favor
discussion between legal and assistance aspects, expand the
implantation of prevention and recovery interventions aimed at
reducing these factors, whether from social or biological
aspects.
Therefore, children and adolescent well-being is one of the
goals
of caring by these professionals(9).
OBJECTIVES
To investigate the presumption of sexual violence through
the records of live births with mothers up to 13 years old in the
city of Maceió, State of Alagoas.
METHODS
Ethical aspects
The study was submitted to the Universidade Federal do
Alagoas’s
Ethics Committee, being approved on 02/02/2018. As it
involved
the use of secondary nominal data of non-public domain, the
Research Ethics Committee (REC) was asked to waive the
Informed
17. Consent Term (ICT), committing to comply with the
information
confidentiality term. Nominal data use was necessary so that
there
was no duplication of subjects during the analysis and to make
it possible to cross-check the information with the bank of the
Brazilian Notifiable Diseases Information System.
Study design, place and period
This is an epidemiological study with a quantitative, observa-
tional approach, with an ecological design. The main advantages
of being an ecological study is the possible union of several
epi-
demiological data from different sources, which favors a broad
view of the association between the possible determining and
conditioning factors of the group exposed to the studied aspect.
In this case, under 14 years old victims of sexual abuse enable a
wide study area with savings in time and resources and make it
possible to measure the effect of an injury on the health condi -
tions of a given population(10-11).
The city of Maceió, currently composed of 50 neighborhoods,
was chosen as the study site, because in 2015 it had 26.8% of
the
total population of children under 14 years old in the State of
Alagoas and represented 51% of the records of live births dur -
ing the period analyzed in this study(12). Moreover, it had a
large
part of the reference units for dealing with sexual violence in
the
sector, composing the protection network for victims.
The research was carried out with data from SINASC involving
records of live births from 2009 to 2017. This period was
defined
18. based on the date of publication of Law 12,015/2009(7), which,
through changes in the penal code for heinous crimes, included
sexual crimes against the vulnerable in this category, applying
the possibility of presumption of violence in cases of children
and adolescents under 14 years old.
Population
This study included children and adolescents between zero
(0) and 13 years, 11 months and 29 days of age classified as
vul-
nerable according to Law 12,015/2009, who were registered at
SINASC as mothers of live births in the city of Maceió.
3Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Silva AJC, Trindade RFC, Oliveira LLF.
Exclusion criteria
Records with information on live births from the same preg-
nancy (twin) and duplicate records from the same birth were not
considered for data treatment.
Study protocol
Among the study variables, they include the newborn birth
date, registration year, mother age, parturient name, Live Birth
Declaration number, declared marital status, father age, neigh-
borhood of residence, number of prenatal care appointments,
number of previous pregnancies and gestational weeks at
19. delivery.
As the data available at SINASC refer to the age group
including
the age of 14 years, which was not of interest in that study, all
records
with mothers aged 14 years were removed, which represented
74.9% (3,146) of the records. Subsequently, for the exclusion
criteria
screening, the following variables were analyzed: parturient
name,
parturient birth date, Declaration of Live Births number, date of
birth
of the newborn and number of fetuses during pregnancy. The
need
to check the variable “number of fetuses during pregnancy”
occurred
so that in twin pregnancy situations, it was not counted twice.
Analysis of results and statistics
After being collected in digital media, the data were subjected
to
review and screening for duplicate records. Statistical analysis
was
performed using the Statistical Package for Social Sciences
software
(SPSS). In the geoprocessing of the results, the Brazilian
National
Institute for Space Research (Instituto Nacional de Pesquisas
Espaciais,
abbreviated INPE) - TerraView program was used, because it is
an ap-
plication for visualization and analysis of geographic data,
enabling
the visualization of the distribution of cases by the city studied.
20. For analysis of descriptive statistics, measures of position and
central tendency, variability and regression were used. For the
applied tests, the level of significance was 5%.
RESULTS
Nine hundred fifty-three live births were registered with
mothers under 14 years old, ranging from 10 to 13 years, with
the age of 13 and 12 years being the most representative, 86.6%
and 11.5%, respectively. The results revealed that the average
age
was 12.8 with a minimum of 10 years (± 0.439), thus showing a
considerably low age range.
When performing the nominal crossing between the database
of the Live Birth Information System (Sistema de Informação
sobre
Nascidos Vivos, abbreviated SINASC) with the Notified
Diseases
Information System (Sistema de Informação de Agravos
Notificados,
abbreviated SINAN). In relation to the victim of sexual abuse
from
0 to 13 years old, it was possible to highlight that among the
number of girls who entered the Brazilian Unified Health
System
(Sistema Único de Saúde) due to childbirth under the age of 14,
only 14 (1.3%) were reported as victims of sexual abuse at
SINAN.
Table 1 shows that 78.3% of mothers of live births declared to
be single, while 20.3% consist of married or in a stable
relationship.
A percentage of 0.1 declared to be separated or widowed. When
21. analyzing the father’s age variable, n reduced considerably to
127
cases, which represents 86.6% of this information not recorded
in the declaration of live births. Among those registered, it was
found that 50% of the children’s parents were over 20 years old.
Another important aspect is related to the obstetric history of
these girls. Table 1 also shows that 5.6% of the girls have
already
experienced another pregnancy under the age of 14, 15.9% had
a premature birth and that 74% of the mothers had at least one
prenatal care appointment before of delivery, showing a
distribution
of the number of the same symmetricals in relation to their
aver-
age. On average, girls have 5.6 prenatal care appointments
during
pregnancy, but 50% of them had fewer than six appointments.
Table 1 - Distribution of mothers under 14 years old registered
in SINASC,
Maceió, Alagoas, Brazil, 2009 to 2017
Characteristics of mothers under 14 years old N %
Declared marital status
Single 746 78.3
Married 11 1.2
Widow 1 0.1
Separated 1 0.1
Common-law marriage 185 19.4
Ignored 9 0.9
Previous pregnances
None 688 72.2
1 or more 53 5.6
22. Ignored 212 22.3
Number of prenatal care appointments
None 6 0.6
1 to 6 476 49.9
<6 230 24.1
Ignored 241 25.3
Gestational weeks at the time of childbirth
Up to 36 weeks 152 15.9
>36 weeks 801 84.1
Source: SINASC (Sistema de Informação sobre Nascidos
Vivos).
The analysis of this variable allowed to reveal that 74% of the
girls under 14 years old who had children born alive between
2009 and 2017 had at least one contact with health profession-
als, and even so sexual violence reporting was present in only
1.3% of cases.
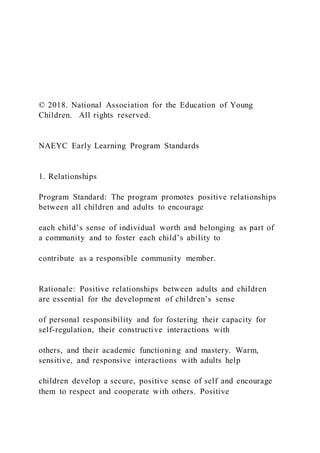
When analyzing the records of live births from 2009 to 2017,
in order to assess the presumed violence in these girls, it was
identified through linear regression that, despite the occurrence
of a 4.9% reduction in the growth rate regarding the number of
live births with mothers under 14 years old between the years
analyzed, a weak linear correlation was identified.
6.00
5.00
4.00
3.00
2.00
1.00
0.00
23. 2009 2010 2011 2012 2013 2014 2015 2016 2017
P
o
r
1
,0
0
0
li
v
e
b
ir
th
s
Birth year
4.34
5.14
4.36
5.14 5.04
4.73
3.08
3.79
24. 4.12
y = -0.1319x + 5.075
R² = 0.2728
Figure 1- Linear regression by the proportion of live births to
mothers
under 14 years old by the total number of live births according
to the years
of birth, Maceió, Alagoas, Brazil, 2009 to 2017
4Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Silva AJC, Trindade RFC, Oliveira LLF.
Regarding the distribution of live births to mothers under 14
years old, according to the neighborhood of residence, it is ob-
served through the map that represents the geographic space of
the city of Maceió, that 20% (10) of the neighborhoods of
Maceió
did not present records at SINASC. There is also a
concentration
in nine neighborhoods (18%) of residence of these mothers in
which the number of births varied from 11 to 55. It is shown on
the map that four neighborhoods concentrate a distribution be-
tween 44 and 55 live births, they are Guaxuma, Benedito
Bentes,
Tabuleiro do Martins, and Jacintinho.
the visibility of the problem and the training for a consistent
and
25. committed service. There is harm when the professional does
not
know and underreport the situation.
There are studies that reveal that this type of underreporting is
common when victims of violence belong to vulnerable groups,
such as children and adolescents under 14 years old, in addition
to women, homosexuals, the elderly and homeless people. The
absence of filling in data is another factor that reveals the lack
of knowledge of the professionals responsible for welcoming
these victims, which weakens the policy and makes qualified
care difficult(9,16-18), identified by means of ignored or
unfilled data.
It is possible to affirm that the situation of vulnerability is pres-
ent in the entire group of adolescents, however the age range
carried out in this study, involving 10 to 13 years old, may
include
the public most susceptible to lack of information and more ex-
posed to sexual abuse, both for the lack of autonomy to consent
to sexual relations and for the fragility in suffering
coercion(19).
Viewing children and adolescents as a vulnerable group al -
lows them to know and understand the particularities of these
subjects, both individually and as a social group, to articulate
network actions and to seek to strengthen citizenship rights and
the duty of assistance, which favors coping with situations as
they
are. the case of sexual abuse, which contributes to the compro-
mise of autonomy as a subject, to the inability to elaborate and
incorporate information aimed at your own care, compromising
the protection and prevention of your health(3,20).
It should be noted that the system adopted by the Code of
Ethics for professions is based on responsibility towards du-
26. ties and obligations. It is noteworthy that the Codes of Ethics
in medicine and nursing, professionals working in the care of
these audiences, including prenatal care, expressly condemn the
omission or collusion of the professional in the face of
situations
of violence of any nature, imposing penalties that may result in
forfeiture of the right to exercise the profession. Thus, violence
reporting omission can be configured as an ethical infraction by
these professionals(21-22).
Some authors define the importance of reporting when
welcoming victims. A study that made it possible to analyze
the protection network flows against violence against children
through reporting, carried out in 2018(23), defines reporting as
one
of the pillars of the fight against child violence and highlights
its potential to define measures of preventing recurrence and
establishing a line of care for victims. Another study(16), which
analyzed health professionals’ Codes of Ethics, regarding the
responsibility to report cases of violence against children and
adolescents, stated that reporting should work and be viewed as
an instrument for the construction of public policies,
contributing
to their dimensioning and ensuring the implantation of public
policies for surveillance and assistance to victims.
Both of the aforementioned studies(16,23) argue that the pre-
vention of sexual abuse is highly relevant, as they act directly
in
reducing the incidence, in combating recurrences, in manipu-
lating the quality of life, in the high costs of care services and
incidence of early pregnancy and contamination by Sexually
Transmitted Infections.
It is necessary to provide guidance to health professionals
inserted in the network of attention to this public, that reporting
27. DISCUSSION
Based on the results, it can be seen that 953 live births were
from pregnancies involving girls under 14 years old, among
them
a portion of 74% had at least one prenatal care appointment and
24.1% did not reach the minimum amount recommended by
the Ministry of Health, which corresponds to a minimum of six
appointments. Among them, only 1.3% were reported at SINAN
as sexual abuse violence.
It is pointed out with this that girls, during her pregnancy,
had contacts with health professionals. However, sexual
violence
report was minimal, thus observing a setting of underreporting
of
cases by health network professionals who provided assistance
to
these minors, considering that, in the age group studied, sexual
violence is seen as suspected and/or presumed.
In Brazil, through Ministerial Decree(13), it is mandatory for
health
professionals to report the Municipal Office of sexual violence
cases
they witness during their professional practice. As an example,
we have prenatal care appointments to pregnant girls assisted
by nurses in primary care. This is a service that when performed
together with qualified listening allows the identification of risk
situations, reporting, and individualized assistance. Studies
dem-
onstrate(14-15) that the increase in the number of reports favors
Meters
28. 0 6000 12000 18000
Number_Residence_Mothers_SINASC
-0.1 ~ 11.0
11.0 ~ 22.0
22.0 ~ 33.0
33.0 ~ 44.0
44.0 ~ 55.1
Missing Data
Figure 2 - Map of the distribution of presumed sexual abuse
according to
SINASC’s records by the place of residence of mothers under
14 with children
born alive between 2009 and 2017, Maceió, Alagoas, Brazil
5Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Silva AJC, Trindade RFC, Oliveira LLF.
is not synonymous with denunciation. In the case of children
and
adolescents who are victims of sexual abuse, only suspicion is
sufficient to carry out the reporting(9). In this phase, sexual
inter-
course is not always a conscious decision, in which the risks
and
consequences involved were evaluated, even though relation-
ships said to be consented or accepted, often the adolescent has
little control over the sexual initiation event, existing a power
29. relationship between the oppressing adult and the oppressed
child or adolescent(24).
It is possible to discuss this when we observe that the data
revealed that among mothers under 14 years old, 20.6% declare
that they are married or in some type of stable union, which
brings up a discussion about the acceptance of marital/sexual
relationship and the prevalence of pregnancy involving girls
under 14 in Maceió.
According to UNICEF (United Nations Children’s Fund), for-
mal or informal union before the age of 18 is defined as child
marriage, although studies show that marriage before the age
of 18 is a violation of the fundamental rights of children and
adolescents, affecting the educational, socioeconomic and
physi-
ological development, in a more disproportionate way in girls
than boys(19,25-26). It is possible to see that child marriage is
still
very present in developing countries, where 1/3 of the girls are
married before the age of 18 and, for every nine girls, a “house”
before the age of 15(26).
According to the Brazilian Civil Code, the nubile age, that is,
the minimum legal age for marriage, corresponds to 16 years,
for both men and women, and Bill 56/2018, which prohibits
marriage with under 16, regardless of the circumstances,
without
relativization, even in situations involving pregnancy(27).
However, between 16 and 18 years old, as they are considered
relatively incapable, these adolescents need to be assi sted by
their
parents or guardians. Therefore, because they are seen before
the Brazilian judiciary as a vulnerable group due to numerous
factors, among them the progression of sexual maturation, mi -
30. nors under 14, according to the majority doctrine, are prevented
from marrying. Furthermore, a sexual relationship is only
morally
legitimate when both parties have the ability to consent, which
the child under 14 does not have(7,19,28-29).
Taking into account legal issues, pregnancy underreporting
in children under 14 contacted in this study reveals that health
professionals naturalize pregnancy and marriage in this group,
ignoring their particularities and treating them as adults, not
viewing the imbalance of discernment in this context and the
consequences they have entailed.
Adolescent pregnancy, unfortunately, is an expressive phe-
nomenon in Brazil, with growing concern due to the number
of records of live births involving mothers between 10 and 14
years old, a group of greatest gestational vulnerability, for both
mother and baby. Among the analysis, this was seen when it
was
identified that 15.9% of births were premature, similar to other
studies, which may be associated with lack of support in the
monitoring of pregnancy, biological immaturity, fragility in the
family structure, enhanced when associated with socioeconomic
and geographic factors(4,30-31).
Although the literature is broader about teenage pregnancy
involving the 15 to 19 year old age group, studies indicate that
recently the inclusion of the 10 to 14 year old population
segment
as a growing reproductive age, associated with the social
vulner-
ability in which they are inserted and in consequent
repercussions,
has been demonstrated in several parts of the country, with the
northeast standing out among the regions(19,24,32-34).
31. Georeferencing, present in that work, made possible the pre-
sumption of sexual violence according to the neighborhood of
residence. It was revealed that among the neighborhoods with
the most reports, two of them are among the five neighborhoods
considered the most violent in the capital, Benedito Bentes and
Tabuleiro do Martins. There is the need for preventive actions
in
the region with a focus on children and adolescents in the com-
munity, planning and implanting policies structured according
to
the particularities of the public that will benefit and the
locations
in which they are located(35).
Specialized care is required from professionals involved in as -
sisting to these victims, allowing compulsory reporting to work
as an instrument to favor protection, prevention, identification
and monitoring by health, social assistance and justice profes -
sionals, in order to strengthen identifying vulnerabilities and
adopting measures to care for these victims. Therefore,
reporting
implies sharing and sharing with different branches of society
the
responsibility to protect our children and adolescents.
Study limitations
As with all types of studies, ecological studies have limitations,
among those present in this study we find the unavailability of
total information on all variables analyzed, due to the lack of
data and the impossibility of an association between exposure
and the individual health status of the subjects, which limits
the conclusions about the cause of the disease. This limitation
is called the ecological fallacy(10-11).
32. Contributions to nursing
It is believed that nurses need to have scientific knowledge
about the problem of violence in order to fulfill their responsi-
bility in relation to professional assistance, taking over the role
of caregiver, that of educator, showing the family, at any time,
the ideology of protection of rights children and adolescents,
emphasizing the prevention of the event and recurrence.
Thus, the study reveals that it is necessary to deepen the
dissemination and understanding of the discussions involving
the issue of violence against children and adolescents, whether
reported or presumed, so that nurses use the scientific
knowledge
built to urgently face the challenge of detecting, reporting,
caring
for, minimizing, and preventing situations of violence against
children and adolescents.
CONCLUSIONS
The results obtained in this study showed that 953 children
were born to mothers aged 10 to 13 years, with only 1.3% of
these
mothers being reported as victims of sexual abuse. Associated
with this fact, it was possible to verify that child marriage is
still
a very present reality in the city of Maceió (20.6%), which
reveals
6Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
33. Silva AJC, Trindade RFC, Oliveira LLF.
that pregnancy in girls up to 13 years old is not identified by
health
professionals as a result of sexual abuse, regardless of whether
the pregnancy is due to a relationship said to be consensual or
not, which accentuates issue underreporting and (in) visibility.
Therefore, it is necessary to debate the issues of sexuality and
gender involved in sexual initiation of pre-teenagers.
FUNDING
The research carried out to build the aforementioned manu-
script received funding from Research Support Foundation of
the State of Alagoas (FAPEAL - Fundação de Amparo à
Pesquisa
do Estado de Alagoas).
REFERENCES
1. Presidência da República (BR). Decreto nº 7.958, de 13 de
Março de 2013. Estabelece diretrizes para o atendimento às
vítimas de violência
sexual pelos profissionais de segurança pública e da rede de
atendimento do Sistema Único de Saúde. Brasília [Internet].
2013 [cited 2018
Nov 13]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2011-
2014/2013/decreto/d7958.htm
2. Faria AAM, Vianna T. Maioridade Sexual: por uma idade de
consentimento sexual pautada na tutela de bens jurídicos. Rev
Bras Ciênc
Crim[Internet]. 2016 [cited 2018 Feb 10];118:15-54. Available
from: http://bdjur.stj.jus.br/jspui/handle/2011/99346
34. 3. Carmo ME, Guizardi FL. O conceito de vulnerabilidade e
seus sentidos para as políticas públicas de saúde e assistência
social. Cad Saúd Púb.
2018;34(3):e00101417. doi: 10.1590/0102-311x00101417
4. Farias R, Moré COO. Impact of pregnancy on at-risk, 10-14
year-old adolescents. Rev Psicol: Reflex Crít[Internet]. 2012
[cited 2018 Jan
28];25(3):596-604. doi: 10.1590/S0102-79722012000300020
5. World Health Organization (WHO). Health for the world’s
adolescents: a second chance in the second decade [Internet].
2014 [cited 2017
Nov 01]. Available from:
http://www.who.int/maternal_child_adolesce nt/documents/secon
d-decade/en/
6. Santos MJ, Mascarenhas MDM, Rodrigues MTP, Monteiro
RA. Caracterização da violência sexual contra crianças e
adolescentes na escola-
Brasil, 2010-2014. Rev Epidemiol Serv Saúde [Internet].
2018;27(2):e2017059. doi: 10.5123/S1679-49742018000200010
7. Presidência da República (BR). Lei Federal n. 12.015, de 7
de agosto de 2009. Altera o Título VI da Parte Especial do
Decreto-Lei no 2.848,
de 7 de dezembro de 1940 - Código Penal, e o art. 1o da Lei no
8.072, de 25 de julho de 1990, que dispõe sobre os crimes
hediondos, nos
termos do inciso XLIII do art. 5o da Constituição Federal e
revoga a Lei no 2.252, de 1o de julho de 1954, que trata de
corrupção de menores
[Internet]. Brasília 2009 [cited 2017 May 03]. Available from:
http://www.planalto.gov.br/ccivil_03/_Ato20072010/2009/Lei/L
12015.htm
35. 8. Carvalho ACBO. Violência sexual presumida. Curitiba:
Juruá, 2005. 23 p.
9. Garbin CAS, Dias IA, Rodovia TAS, Garbin AJI. Desafios do
profissional de saúde na notificação da violência:
Obrigatoriedade, efetivação e
encaminhamento. Ciênc Saúde Colet [Internet].
2015;20(6):1879-1890. doi: 10.1590/1413-
81232015206.13442014
10. Medronho RA. Estudos ecológicos. In: Medronho RA, et al.
Epidemiologia. São Paulo: Atheneu; 2009. 265-74 p.
11. Hulley SB, Cummings SR, Browner W, Grady DG, Newman
TB. Delineando a pesquisa clínica: Uma abordagem
epidemiológica. Porto Alegre:
Artmed, 2015. 47-80 p.
12. Ministério da Saúde (BR). Departamento de Informática do
SUS. Sistema de Informação de saúde. [Internet]. Datasus. 2018
[cited 2018 jan
20]. Available from: http://datasus.saude.gov.br/informacoes -
de-saude/tabnet.
13. Ministério da Saúde (BR). Portaria nº204, de 17 de
fevereiro de 2016. Define a Lista Nacional de Notificação
Compulsória de doenças, agravos
e eventos de saúde pública nos serviços de saúde públicos e
privados em todo o território nacional, nos termos do anexo, e
dá outras
providências[Internet]. 2016 [cited 2019 Feb 01]. Available
from:
http://bvsms.saude.gov.br/bvs/saudelegis/gm/2016/prt0204_17_
02_2016.html
36. 14. Alves JM, Vidal ECF, Fonseca FLA, Vidal ECF, Silva MJ,
Pinto AGA, et al. Notificação da violência contra criança e
adolescentes por
profissionais de saúde. Rev Fac Ciênc Méd. 2017;19(1):26-32.
doi: 10.5327/Z1984-4840201726596
15. Ministério da Saúde (BR). Secretaria de Atenção à Saúde.
Departamento de Atenção Básica. Atenção ao pré-natal de baixo
risco [Internet].
2013 [cited 2018 Dec 03]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_
32.pdf
16. Almeida AHV, Silva MLCA, Musse JO, Marques JAM. A
responsabilidade dos profissionais de saúde na notificação dos
casos de violência
contra crianças e adolescentes de acordo com seus códigos de
ética. Arq Odontol [Internet]. 2012 [cited 2018 Jun
16];48(2):102-15.
Available from:
http://revodonto.bvsalud.org/pdf/aodo/v48n2/a08v48n2.pdf
17. Mascarenhas MDM, Andrade SSCA, Neves ACM, Pedrosa
AAG, Silva MMA, Malta DC. Violência contra pessoa idosa:
análise das notificações
realizadas no setor de saúde. Ciênc Saúde Colet [Internet].
2012;17(9):2331-2341. doi: 10.1590/S1413-
81232012000900014
18. Meneghel SN, Bairros F, Mueller B, Monteiro D, Oliveira
LP, Collaziol ME. Rotas críticas de mulheres em situação de
violência:
depoimentos de mulheres e operadores em Porto Alegre, Rio
Grande do Sul, Brasil. Cad Saúde Púb. 2011;27(4):743-52. doi:
10.1590/
S0102-311X2011000400013
37. 19. Cavasin S, (Org.). Gravidez entre adolescentes de 10 a 14
anos: estudo exploratório em cinco capitais brasileiras e
vulnerabilidade social:
relatório de pesquisa. São Paulo: ECOS; 2004. p. 13-35.
20. Egry EY, Apostólico MR, Morais TCP, Lisboa CCR. Coping
with child violence in primary care: how do professionals
perceive it? Rev Bras
Enferm. 2017;70(1):113-9. doi: 10.1590/0034-7167-2016-0009
7Rev Bras Enferm. 2020;73(Suppl 4): e20190143 7of
Presumption of sexual abuse in children and adolescents:
vulnerability of pregnancy before 14 years
Silva AJC, Trindade RFC, Oliveira LLF.
21. Conselho Federal de Enfermagem. Resolução COFEN nº
564, de 06 de novembro de 2017. Reformulação do Código de
Ética
dos Profissionais de Enfermagem[Internet]. 2017 [cited 2018
Dec 06]. Available from: http://www.cofen.gov.br/resolucao-
cofen-
no-5642017_59145.html
22. Conselho Federal de Medicina. Resolução CFM nº 2.217, de
01 de novembro de 2018. Aprova o Código de Ética
Médica[Internet]. 2018
[cited 2018 Dec 06]. Available from:
http://portal.cfm.org.br/images/PDF/cem2019.pdf
23. Egry EY, Apostolico MR, Morais TCP. Notificação da
violência infantil, fluxos de atenção e processo de trabalho dos
38. profissionais da Atenção
Primária em Saúde. Ciênc. Saúde Colet. [Internet]. 2018;
23(1):83-92. doi: 10.1590/1413-81232018231.22062017.
24. Rede Nacional da Primeira Infância (RNPI). Primeira
Infância e gravidez na Adolescência. Centro de Estudos
integrados: infância,
adolescência e Saúde [Internet]. 2015 [cited 2019 Feb 02].
Available from: http://primeirainfancia.org.br/wp-
content/uploads/2015/01/
Cartilha-Gravidez-Adol-FINAL-HD.pdf
25. UNICEF. State of the World's Children. New York: UNICEF
[Internet]. 2013 [cited 2018 Dec 12]. Available from:
https://www.unicef.org/
sowc2013/
26. Tascón LAM, Benítez DIC, Tascón LIM, Ospina CBP,
Guatibonza MDA, Bejarano JHC, et al. Matrimonio infantil: un
problema social, económico
y de salud pública. Rev Child Obstet Ginecol. 2016;81(3):254-
61. doi: 10.4067/S0717-75262016000300013
27. Brasil. Projeto de Lei nº 56/2018. Confere nova redação ao
art. 1.520 da Lei nº 10.406, de 10 de janeiro de 2002 (Código
Civil), para suprimir
as exceções legais permissivas do casamento infantil. Brasília
[Internet]. 2018 [cited 2019 Feb 15]. Available from:
https://www25.senado.
leg.br/web/atividade/materias/-/materia/133561.
28. Câmara dos Deputados (BR). Código Penal Brasileiro. Lei
11.106/2005: Altera os arts. 148, 215, 216, 226, 227, 231 e
acrescenta o art. 231-A
ao Decreto-Lei no 2.848, de 7 de dezembro de 1940 – Código
Penal e dá outras providências. Brasília [Internet]. 2005 [cited
39. 2019 Feb 10].
Available from:
http://www.planalto.gov.br/ccivil_03/_Ato2004-
2006/2005/Lei/L11106.htm.
29. Nogueira RM. A evolução da sociedade patriarcal e sua
influência sobre a identidade feminina e a violência de gênero.
Rev Jus Navigandi
[Internet]. 2016 [cited 2018 Oct 11]; 23(5377). Available from:
https://jus.com.br/artigos/48718
30. Costa EL, Sena MCF, Dias A. Gravidez na adolescência:
determinante para prematuridade e baixo peso. Comun Ciênc
Saúde [Internet]. 2011
[cited 2018 Sep 20];22(Sup-1):183-8. Available from:
http://bvsms.saude.gov.br/bvs/artigos/gravidez_adolescencia.pdf
31. Souto RMCV, Porto DL, Pinto IV, Vidotti CCF, Barufaldi
LA, Freitas MG, et al. Estupro e gravidez de meninas de até 13
anos no
Brasil: características e implicações na saúde gestacional, parto
e nascimento. Ciênc Saúde Colet. 2017;22(9):2909-18. doi:
10.1590/1413-81232017229.13312017
32. Costa RP. Gilberto Freyre e a infância no Brasil patriarcal.
Angelus novus [Internet]. 2015 [cited 2018 Sep 22];6(10):41-
60. Available from:
http://www.revistas.usp.br/ran/article/view/123940/120178
33. Pedro Filho F, Sigrist RMS, Souza LB, Mateus DC, Rassam
E. Perfil epidemiológico da grávida adolescente no município
de Jundiaí e sua
evolução em trinta anos. Adolesc Saúde [Internet]. 2011 [cited
1019 Jan 10];8(1):21-27. Available from:
http://www.adolescenciaesaude.
com/detalhe_artigo.asp?id=261
41. *Applies to all accreditation site visits
beginning July 2019 until otherwise informed.
NAEYC Early Learning Program Accreditation
Standards and Assessment Items Copyright
2019 National Association for the Education of
Young Children. All rights reserved.
NAEYC Accreditation
Chief Strategy and
Innovation Officer,
Michelle Kang
Senior Director, NAEYC
Accreditation of
Early Learning Programs
Kristen Johnson
Director, Quality
Assessment and Assurance
Susan Hedges
Senior Reliability Specialist
Amanda Batts
Director, Quality Improvement
and Program Support
April D. Kimble
Senior Creative Design Manager
Henrique J. Siblesz
44. and Harmonious Classroom ................ 13
1.E—Addressing Challenging
Behaviors .............................................. 14
1.F—Promoting Self-Regulation ........... 15
Accreditation Assessment Items for
Standard 1—Relationships ...................16
2 Curriculum ............................... 19
Definition of Standard 2—Curriculum 19
Rationale ............................................. 20
Topic Areas ......................................... 20
2.A—Essential Characteristics ............ 20
2.B—Social and Emotional
Development....................................... 22
2.C—Physical Development ................ 23
2.D—Language Development ............. 23
2.E—Early Literacy............................... 24
2.F—Early Mathematics ...................... 26
2.G—Science ........................................27
2.H—Technology ................................. 28
2.J—Creative Expression and
Appreciation for the Arts .................... 29
45. 2.K—Health and Safety ....................... 30
2.L—Social Studies ............................. 30
Accreditation Assessment Items for
Standard 2—Curriculum ..................... 32
3 Teaching ..................................39
Definition of Standard 3—Teaching ... 39
Rationale ............................................. 40
Topic Areas ......................................... 40
3.A—Designing Enriched Learning
Environments ...................................... 40
3.B—Creating Caring Communities for
Learning ............................................... 41
3.C—Supervising Children ................. 42
3.D—Using Time, Grouping, and
Routines to Achieve Learning Goals .. 44
3.E—Responding to Children’s Interests
and Needs ........................................... 44
3.F—Making Learning Meaningful for All
Children ............................................... 45
3.G—Using Instruction to Deepen
Children’s Understanding and Build
Their Skills and Knowledge ................ 46
46. Accreditation Assessment Items for
Standard 3—Teaching ........................ 48
4 Assessment of Child Progress 53
Definition of Standard 4—Assessment of
Child Progress ..................................... 53
Rationale ............................................. 54
Topic Areas ......................................... 54
4.A—Creating an Assessment Plan .... 54
4.B—Using Appropriate Assessment
Methods .............................................. 55
4.C—Identifying Children’s Interests
and Needs and Describing Children’s
Progress .............................................. 56
4.D—Adapting Curriculum,
Individualizing Teaching, and Informing
Program Development ........................57
4.E—Communicating With Families and
Involving Families in the Assessment
Process .................................................57
Accreditation Assessment Items
for Standard 4—Assessment of
Child Progress ..................................... 59
5 Health ...................................... 61
Definition of Standard 5—Health ......61
47. Rationale ............................................. 62
Topic Areas ......................................... 62
5.A—Promoting and Protecting
Children’s Health and Controlling
Infectious Disease ............................... 62
Health records ................................. 62
Health consultants ........................... 63
Staff training and program practices
in the event of illness ....................... 63
Outdoor activities ............................ 64
Diapering .......................................... 65
Hand washing .................................. 66
Children’s medications .................... 66
Water play ........................................ 67
Sudden infant death syndrome....... 67
Feeding ............................................ 68
5.B—Ensuring Children’s Nutritional
Well-Being ........................................... 69
5.C—Maintaining a Healthful
Environment ......................................... 71
48. Accreditation Assessment Items for
Standard 5—Health ............................. 73
6 Staff Competencies,
Preparation, and Support ........... 77
Definition of Standard 6—
Staff Competencies,
Preparation, and Support ....................77
Rationale ............................................. 78
Topic Areas ......................................... 78
6.A—Supportive Work Environment ... 78
6.B—Professional Identity and
Recognition ......................................... 80
6.C—Qualifications of Teaching and
Administrative Staff ............................. 81
6.D—Ongoing Professional
Development....................................... 82
Accreditation Assessment Items for
Standard 6—Staff Competencies,
Preparation, and Support ................... 85
7 Families ................................... 90
Definition of Standard 7—Families .....90
Rationale ..............................................91
Topic Areas ..........................................91
49. 7.A—Knowing and Understanding the
Program’s Families ...............................91
7.B—Sharing Information Between Staff
and Families ........................................ 93
7.C—Nurturing Families as Advocates
for Their Children ................................ 95
Accreditation Assessment Items for
Standard 7—Families ...................... 96
8 Community Relationships ....... 97
Definition of Standard 8—Community
Relationships ....................................... 97
Rationale ............................................. 98
Topic Areas ......................................... 98
8.A—Linking With the Community ..... 98
8.B—Accessing Community
Resources ............................................ 99
8.C—Acting as a Citizen in the
Neighborhood and the Early Childhood
Community ....................................... 100
Accreditation Assessment Items
for Standard 8—Community
Relationships ......................................102
9 Physical Environment ............ 103
50. Definition of Standard 9—Physical
Environment ...................................... 103
Rationale ........................................... 104
Topic Areas ....................................... 104
9.A—Indoor and Outdoor Equipment,
Materials, and Furnishings................ 104
Basic furnishings ............................ 104
Curriculum-related materials and
equipment .......................................105
Design of indoor environments ..... 106
9.B—Outdoor Environmental Design 107
9.C—Building and Physical Design ... 109
9.D—Environmental Health ................ 111
Accreditation Assessment Items for
Standard 9—Physical Environment ... 113
10 Leadership and
Management ............................ 115
Definition of Standard 10—Leadership
and Management ................................115
Rationale ............................................ 116
Topic Areas ........................................ 116
51. 10.A—Leadership ............................... 116
10.B—Management Policies and
Procedures ..........................................117
10.C—Fiscal Accountability Policies and
Procedures ......................................... 118
10.D—Health, Nutrition, and Safety
Policies and Procedures .................... 119
10.E—Personnel Policies ....................120
10.F—Program Evaluation,
Accountability, and
Continuous Improvement ..................121
Accreditation Assessment Items
for Standard 10—Leadership and
Management ...................................... 122
NAEYC Accreditation
Glossary of Terms .......................127
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
6
Introduction
Since 1926, the National Association for the Education of
Young Children
(NAEYC) has strived to improve the quality of early learning
programs for
52. young children by defining a vision for high quality and
providing tools and
resources to achieve that vision. For more than 30 years,
NAEYC Accreditation
of Early Learning Programs has been one of the Association’s
most powerful
mechanism in this regard. The NAEYC accreditation system
sets the standard
for excellence—for families, the early childhood education
profession as well as
the public—and offers support to programs to meet the
standards.
The comprehensive nature of the NAEYC Early Learning
Program Accreditation
Standards and Assessment Items outlined in this document—
with its combined
focus on children, staff, partnerships, and administration —
promotes program
accountability and makes it possible for programs to
consistently provide high
quality learning experiences for each child and maintain the
infrastructure
needed to sustain this high level of quality over time. The
NAEYC Early Learning
Program Accreditation Standards and Assessment Items provide
guidance to
all programs about making improvements regardless of whether
they intend to
seek accreditation.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
53. 7
Each of the 10 standards is a broad statement that describes an
essential
element that together with the other nine standards provide a
definition
of quality for early learning programs serving young children
birth
through kindergarten.
Mirroring the value of continuous improvement, the NAEYC
Accreditation of
Early Learning Programs process and standards are constantly
reviewed under
the auspices of the Council on the Accreditation of Early
Learning Programs to
ensure that they are informed by current research and reflect the
ever-evolving
early childhood landscape.
NAEYC gratefully acknowledges early childhood educators,
program
administrators, accreditation assessors, accreditation faci litation
specialists,
coaches, families, policy makers, researchers, NAEYC
governance bodies, and
NAEYC staff for their continued guidance and support.
Limitations of Use
This document outlines the NAEYC Early Learning Program
Accreditation
Standards and Assessment Items. However, it does not include
the
complementary tools and guidance that are needed to gain a
deeper
understanding of how these standards and assessment items
54. drive accreditation
decisions. Use of complementary tools and guidance is highly
recommended.
Basic Structure
Standard
› Definition
› Rationale
› Topic Areas
• Description
• Recommended Best Practices
› Accreditation Assessment Items (measured
to determine the accreditation decision)
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
8
Overview
STANDARD 1
Relationships
The program promotes positive relationships between all
children and adults
to encourage each child’s sense of individual worth and
belonging as part of
a community and to foster each child’s ability to contribute as a
55. responsible
community member.
STANDARD 2
Curriculum
The program implements a curriculum that is consistent with its
goals for
children and that promotes learning and development in each of
the following
areas: social, emotional, physical, language, and cognitive.
STANDARD 3
Teaching
The program uses a variety of developmentally, culturally, and
linguistically
appropriate and effective teaching approaches that enhance each
child’s
learning and development in the context of the program’s
curriculum goals.
STANDARD 4
Assessment of Child Progress
The program uses a variety of formal and informal assessment
approaches
to provide information on children’s learning and development.
These
assessments occur in the context of reciprocal communications
between
teachers and families, and with sensitivity to the cultural
contexts in which
children are developing. The program uses assessment results to
inform
decisions about the children in their care, to improve teaching
56. practices, and
to drive program improvement.
STANDARD 5
Health
The program promotes the nutrition and health of children and
protects
children and staff from illness.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
9
STANDARD 6
Staff Competencies,
Preparation, and Support
The program employs and supports a teaching and
administrative staff that
have the qualifications, knowledge, and professional
commitment necessary
to promote children’s learning and development and to support
families’
diverse needs and interests.
STANDARD 7
Families
The program establishes and maintains collaborative
relationships with
each child’s family to foster children’s development in all
settings. These
57. relationships are sensitive to family composition, language, and
culture.
STANDARD 8
Community Relationships
The program establishes relationships with and uses the
resources of the
children’s communities to support the achievement of program
goals.
STANDARD 9
Physical Environment
The program has a safe and healthful environment that provides
appropriate
and well-maintained indoor and outdoor physical environments.
The
environment includes facilities, equipment, and materials to
facilitate child and
staff learning and development.
STANDARD 10
Leadership and Management
The program effectively implements policies, procedures, and
systems that
support stable staff and strong personnel, fiscal, and program
management so
all children, families, and staff have high-quality experiences.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
58. 10
STANDARD 1
Relationships
Definition of Standard 1—Relationships
The program promotes positive relationships between all
children and adults
to encourage each child’s sense of individual worth and
belonging as part of
a community and to foster each child’s ability to contribute as a
responsible
community member.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
11
Rationale
Positive relationships between adults and children are essential
for the development
of children’s sense of personal responsibility and for fostering
their capacity for self-
regulation, their constructive interactions with others, and their
academic functioning
and mastery. Warm, sensitive, and responsive interactions with
adults help children
develop a secure, positive sense of self and encourage them to
respect and cooperate
with others. Positive relationships with adults help children
gain the benefits of
instructional experiences and resources. Children who see
themselves as highly valued
59. are more likely to feel secure, thrive physically, get along with
others, learn well, and
feel part of a community.
The Relationships Standard includes six topic areas (1.A, 1.B,
1.C, 1.D, 1.E, and 1.F).
Topic Areas
› 1.A—Building Positive Relationships Between Teachers and
Families
› 1.B—Building Positive Relationships Between Teachers and
Children
› 1.C—Helping Children Make Friends
› 1.D—Creating a Predictable, Consistent, and Harmonious
Classroom
› 1.E—Addressing Challenging Behaviors
› 1.F—Promoting Self-Regulation
1.A—Building Positive Relationships Between Teachers and
Families
Topic 1.A addresses the development and maintenance of
positive, reciprocal
relationships between teachers and families, emphasizing the
need for ongoing
communication and sensitivity to family diversity.
Recommended Best Practices
We cannot overstate the importance of the relationship between
teacher and family.
At the start, teachers need to be sensitive to the fact that some
60. families are uneasy
about having their children in child care. Trust building takes
time and attention,
but is essential. Parents need to feel trust in their child’s
teachers, and teachers need
to know and understand the family in order to fully understand
the child. Teachers
should solicit input from families about their child’s needs and
how the family defines
their race, culture, religion, home language, and family
structure (e.g., nuclear, single
parent, childless, multi-generational, same-sex, blended
families). Regular two-
way communication is an essential element for maintaining
positive relationships
with families. Teachers keep families informed about their
child’s progress at the
program, and parents share information about what’s going on
in the child’s home
life. Teachers also give families practical information about
classroom routines, rules,
and expectations. Nurturing a strong partnership with families
helps to ensure that
children’s needs are met, families’ concerns are addressed, and
transitions between
program and home are smooth.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
12
1.B—Building Positive Relationships
Between Teachers and Children
61. Topic 1.B addresses the development of positive, individualized
relationships
between teachers and children, emphasizing the need for
consistent, predictable
care; frequent social interactions; acceptance of a wide range of
emotions; and
support and acknowledgement of all children as capable and
resourceful.
Recommended Best Practices
Children learn best when they feel respected and valued.
Teachers can create a positive
emotional climate in their classroom through their warm,
affectionate verbal and
physical interactions and consistent, predictable care. All
teaching staff must also
demonstrate the ability to interact appropriately with young
children: communicate
at their level, protect them from harm, provide activities,
encourage socialization, and
manage them gently. Smiles, eye contact, and calm tones of
voice all contribute to
positive relationships. Physical punishment such as shaking,
slapping, pulling limbs,
pinching, or requiring a child to remain inactive for a long
period of time is never
permitted. It is important that teachers appreciate each child’s
unique personality,
abilities, activity level, and pace of development and that they
respond to children’s
individual needs. For toddlers and older children, teachers show
respect for children
by listening to them, answering their questions, and engaging
them in meaningful
conversations. Children feel more secure when teachers
62. encourage children’s self-
reliance in the classroom and acknowledge their
accomplishments.
As children learn to express and manage their emotions,
teachers are important as
guides and models. They provide comfort and support when
children experience
hurt, fear, and anger, and they encourage children to express
both positive and
negative emotions in appropriate ways. Teachers must
themselves model good
emotional expression and management. To avoid creating a
negative emotional
climate, teachers do not engage in psychological abuse such as
verbal abuse,
threats, harsh remarks, ridicule, or stand by when other adults
or children do these
things. Coercive tactics such as rough handling, forcing a child
to sit or lie down, or
physically forcing a child to perform an action are also never
used.
With infants and young toddlers, relationship building begins
when teachers learn to
read a baby’s nonverbal signals and to sense mood and level of
attention, and adjust
their interactions accordingly. Social interactions include
singing, narrating, and
responding to a baby’s coos and sounds. Making eye contact
and giving one-on-one
attention during caregiving routines (e.g., diapering, changing
clothes, cleaning) also
help teachers create a positive, individual relationship with each
little one.
63. NAEYC Early Learning Program Accreditation Standards and
Assessment Item
13
1.C—Helping Children Make Friends
Topic I.C addresses the role teachers play in the development of
friendships
between children: they design opportunities that promote peer
engagement, help
children sustain and enhance play, and help children resolve
conflict.
Recommended Best Practices
Children need help navigating the complexities of forming
positive social
relationships with peers. For infants, this begins with creating
opportunities to
interact with other babies. As children grow, teachers have to
supervise children’s
interactions and engage with them during play to help them
build friendships.
While allowing children to take the lead, teachers’ participation
in children’s play
can help make it more complex and cooperative. Teaching staff
should encourage
children to resolve their own conflicts and support them in
identifying their feelings
and working together to develop and try a variety of solutions.
To help all children
feel included, teachers may need to ensure that socially reserved
children are
invited into other children’s play and helped to practice positive
64. peer interaction
skills such as sharing materials, exchanging thoughts or ideas,
saying nice things
and being helpful to others. Children who hurt or bully others
are helped to follow
classroom rules.
1.D—Creating a Predictable, Consistent,
and Harmonious Classroom
Topic 1.D addresses the creation of classroom environments in
which limits are
clear, bias is countered, and prosocial behavior is promoted.
Recommended Best Practices
Teachers create harmonious classrooms when they model
consideration and
respect for all the children, intentionally address issues of bias,
and value
differences. For example, children’s environments should
display images of
children and their families and include materials that reflect the
cultures of the
children in the class. Staff should review and remove older
books, posters, music,
and other materials that might promote stereotypes. Teachers
are aware of
caricatures of gender, racial or ethnic groups, age, and class. To
support prosocial
behaviors in children, teachers model sharing and caring by
encouraging children
to listen to each other and by helping them negotiate their
interactions as they play.
Teachers identify and label children’s prosocial behaviors when
they see them and
foster positive self-identity by encouraging children to name
65. and embody affirming
personal attributes such as “I am good at doing puzzles”, “I am
a good big brother”,
“I can run fast”. Teachers also intentionally teach social skills
such as playing
cooperatively, turn taking, expressing emotion in non-harmful
ways, and learning
about self and others. They follow up with guidance and
prompts to help children
learn to take turns and listen to others. To encourage a sense of
community,
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
14
teachers have children participate often in decision making
about classroom
rules, plans, and activities and expect children to help care for
their classroom.
To proactively maintain a harmonious environment, teachers
learn to anticipate
potential behavior problems and take steps to prevent them.
Teachers promote emotional competence by helping children
talk about emotions
in themselves and others. They help children identify different
feelings and the way
feelings can be expressed. Children are encouraged to comfort
their friends who are
sad or distressed.
1.E—Addressing Challenging Behaviors
66. Topic 1.E addresses the skills teachers need to protect children
from harm and the
support teachers must provide to help children develop new and
more adaptable
ways to relate to peers and adults. Sharing information between
staff and
families, helping families advocate for their children, and
linking families and the
program with community resources help ensure that children
and families receive
necessary support. Proactive ways to address challenging
behaviors include
carefully designing the learning environment.
Recommended Best Practices
Staff understand and recognize that challenging behaviors are
children’s attempts
to communicate a message, such as, “I am scared,” “I am hurt,”
or “I want to play
with you.” To that end, they use multiple strategies to prevent
and address these
behaviors and to build children’s positive social and emotional
regulation and
their communication skills. Common examples of challenging
behaviors in the
early learning setting include physical aggression such as
hitting, biting, shoving,
whacking with toys, relational aggression (“You can’t play with
us.”), verbal
bullying, tantrums, whining, testing limits, or refusal to follow
directions or observe
classroom rules.
To help minimize challenging behaviors, teachers should
routinely observe their
67. group in action to identify events, activities, interactions, and
other contextual
factors that may be predictive of challenging behavior. When
they identify
environmental factors that might be contributing to behavior
problems, they make
environmental modifications and implement targeted teaching
strategies designed
to support appropriate behaviors.
When responding to challenging behaviors, teachers avoid using
negative responses
(e.g., “stop pushing!”, “No running!”). Teachers help children
learn appropriate
social, communication, and emotional regulation skills such as
taking turns,
moderating voice, and expressing emotions in non-harmful
ways, persisting
when frustrated, and gaining control of physical impulses.
Teachers are respectful
and calm, and they ensure the emotional and physical safety of
the child and
others in the classroom. They provide support and guidance to
help children
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
15
develop alternative behaviors. These include setting realistic
and age-appropriate
expectations for behavior, establishing clear and consistent
routines, and engaging
68. children in cooperative activities and group projects.
For children with persistent or serious challenging behaviors,
individualized plans
designed to support inclusion and success are developed jointly
with families and
other support service staff (e.g., psychologists, social workers,
therapists).
The program establishes a written policy related to suspension,
expulsion and
other exclusionary measures. The goal of this policy is to
severely limit or eliminate
exclusionary measures. The policy clearly states the
circumstances under which
various types of exclusion may occur, and is communicated to
families, staff, and
other relevant stakeholders. Exclusionary measures are not
considered until all
other possible interventions have been exhausted, and unless
there is agreement
that another placement is in the best interest of the child. If
exclusionary measures
must be taken, the program assists the family in accessing
services and identifying
an alternative placement. The policy complies with federal and
state civil rights
laws.
1.F—Promoting Self-Regulation
Topic 1.F addresses the teacher’s role in determining and
providing necessary
support for children to regulate their emotions and manage their
own behavior.
Recommended Best Practices
69. When children learn to manage their behavior, thoughts, and
feelings, they are
developing self-regulation. Children need self-regulation to
successfully and
actively participate in learning. To develop self-regulation,
children need many
opportunities to experience and practice skills with adults and
peers. With toddlers
and older children, teachers actively teach social,
communication, and emotional
regulation skills including helping children to use language to
communicate their
needs, appropriately expressing their emotions, and taking turns
when speaking
with each other. They continually look for opportunities to
provide supports and
guidance to help children build these skills. Further, they
support self-regulation
by helping children to problem solve and persist when they are
frustrated or
challenged, take turns and play cooperatively with others,
control physical
impulses, use language to communicate needs, express emotions
in ways that do
not harm others, and use problem-solving techniques.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
16
Item Number Accreditation Assessment Item
Source of
70. Evidence
1B.1
Teachers respond to children's negative emotions (hurt, fear,
anger) by
offering developmentally appropriate comfort, support, and
assistance.
CO
1B.2
Teachers take into account children's differing
temperaments when relating to each child.
CO
1B.3
Teachers take into account children's differing
activity levels when relating to each child.
CO
1B.4
Required; Must Be Met
to Earn and Maintain
Accreditation
Staff never use physical punishment and do not
engage in psychological abuse or coercion.
CO
1B.5 Infant teachers talk, coo, and sing to infants and repeat
infants' sounds. CO
71. 1B.6
Teachers are aware of infants', toddlers', and twos'
individual levels of arousal and moderate their own
voice level and physical interaction accordingly.
CO
1B.7
Teachers can distinguish the meaning of infants’, toddlers',
and twos’ various cries and other signs of distress.
CO
1B.8
Show that your guidance/discipline policy states that staff may
never use
physical punishment, psychological abuse, or coercion when
disciplining
a child. The policy must include examples of prohibited staff
practices.
PP
1B.9 Show how your guidance/discipline policy is
communicated to all staff. PP
1B.10
Required; Must Be Met
to Earn and Maintain
Accreditation
Show that your guidance/discipline policy does not include any
circumstances when it is permissible for staff to use any form of
72. physical
punishment, psychological abuse, or coercion when disciplining
a
child. Appropriate use of restraint for safety reasons is
permissible.
PP
Accreditation Assessment Items for Standard 1—Relationships
Sources of Evidence
CO Class Observation
CP Class Portfolio
PO Program Observation
PP Program Portfolio
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
17
Item Number Accreditation Assessment Item
Source of
Evidence
1C.1
Teachers facilitate infants' interest in looking at,
touching, or vocalizing to other people.
CO
73. 1C.2
Teachers give children a chance to resolve their own
conflicts without immediate teacher intervention.
CO
1C.3 When children are in conflict, teachers help them identify
their feelings. CO
1C.4
When children are in conflict, teachers help them
identify and describe the problem.
CO
1C.5
When children are in conflict, teachers help
them think of alternative solutions.
CO
1C.6
Show or describe two examples of how you help
make children's play more complex.
CP
1D.1
Classroom materials show persons with differing abilities
engaged
in activities that counteract stereotypical limitations.
CO
1D.2
74. Classroom materials show persons of different
ethnic or cultural backgrounds engaged in activities
that counteract stereotypical limitations.
CO
1D.3
Teachers offer children the chance to choose activities,
materials, and areas in which to play.
CO
1D.4 Teachers anticipate problematic behavior and take steps to
prevent it. CO
1D.5
Teachers use narration and description of ongoing
interactions to identify prosocial behaviors.
CO
1D.6
Show two objects, materials or visual images in your classroom
that
depict men and/or women in work, family, and/or personal
roles.
CP
1D.7
Show or describe one example of how children have
opportunities
to participate in decision making about class plans.
CP
75. 1D.8
Show or describe one example of how you have anticipated
problematic behavior and taken steps to prevent it.
CP
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
18
Item Number Accreditation Assessment Item
Source of
Evidence
1E.1
Show that your program’s written guidance and discipline
policy
addresses the use of suspension, expulsion and other
exclusionary
measures, and includes ALL of the features listed below.
› Policy is communicated to families and staff.
› Stated goal of policy is to limit or eliminate the use of
suspension, expulsion and other exclusionary measures.
› Policy states the circumstances under which
types of exclusion may occur.
› Policy states what steps are taken before a
decision to exclude is considered.
76. › Exclusionary measures are not considered until all other
possible interventions have been exhausted, and there is
agreement that exclusion is in the best interest of the child.
› If exclusionary measures must be taken, the program offers
assistance
to the family in accessing services and an alternative placement.
› Policy acknowledges that it complies with
federal and state civil rights laws.
PP
1F.1 Teachers help children learn emotional regulation skills.
CO
1F.2
Teachers guide and support children to use
language to communicate needs.
CO
1F.3 Teachers guide and support children to gain control of
physical impulses. CO
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
19
STANDARD 2
Curriculum
Definition of Standard 2—Curriculum
77. The program implements a curriculum that is consistent with its
goals for children
and that promotes learning and development in each of the
following areas: social,
emotional, physical, language, and cognitive.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
20
Rationale
A curriculum that draws on research assists teachers in
identifying important
concepts and skills as well as effective methods for fostering
children’s learning
and development. When informed by teachers’ knowledge of
individual children, a
well-articulated curriculum guides teachers so they can plan
learning experiences
that promote children’s growth across a broad range of
developmental and content
areas. A curriculum also helps ensure that the teacher is
intentional in planning a
daily schedule that (a) maximizes children’s acquisition of
desired knowledge and
skills through the effective use of time and materials and (b)
offers opportunities for
children to learn through play and through structured activities,
individually and in
groups, according to their developmental needs and interests.
The Curriculum Standard includes 11 topic areas (2.A, 2.B, 2.C,
2.D, 2.E, 2.F, 2.G,
78. 2.H, 2.J, 2.K, and 2.L).
Topic Areas
› 2.A—Essential Characteristics
› 2.B—Social and Emotional Development
› 2.C—Physical Development
› 2.D—Language Development
› 2.E—Early Literacy
› 2.F—Early Mathematics
› 2.G—Science
› 2.H—Technology
› 2.J—Creative Expression Appreciation for the Arts
› 2.K —Health and Safety
› 2.L —Social Studies
2.A—Essential Characteristics
Topic 2.A addresses the necessity for a clear, coherent
philosophy and explicit
educational goals for meeting the learning and developmental
needs of all children
in an early childhood program. It emphasizes effective use of
groupings, settings,
and schedules and the importance of materials that reflect not
only the lives of the
children and families in the program but also the diversity
found in society.
79. Recommended Best Practices
All programs should have a written statement of philosophy
guiding their educational
goals. A comprehensive, age-appropriate curriculum guides
teachers’ development
and intentional implementation of learning opportunities that
are consistent with
the program’s goals and objectives for children of all ages. The
written curriculum
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
21
framework should provide a coherent focus for planning
children’s experiences. It
should also allow for adaptations and modifications to ensure
access to the curriculum
for all children. For preschoolers and kindergartners, the
curriculum allows teachers
to intentionally plan opportunities for play, including dramatic
play and blocks,
that relates specifically to the classroom topics of study (e.g.,
seasons, farm animals,
transportation, and insects).
A comprehensive curriculum includes content, concepts, and
activities that foster
social, emotional, physical, language, and cognitive
development. Curriculum for
cognitive development includes key areas: literacy,
80. mathematics, science, technology,
social studies, health and safety, creative expression, and
appreciation of the arts.
It is important that curriculum be implemented in a way that
reflects the family
values, beliefs, experiences, cultures, and languages of all
enrolled children.
Teachers rely on the curriculum goals and objectives to inform
their ongoing
assessment of children’s progress. The curriculum should
provide guidance to
teachers about how to integrate assessment information with
curriculum goals in
order to create individualized learning experiences in the
classroom.
The curriculum should allow for the development of a daily
schedule that is
predictable, yet flexible and responsive to the individual
children’s needs. The
daily schedule must include both indoor and outdoor
experiences, sufficient time
and support for transitions, and periods of rest, active play, and
planned learning
experiences including experiments, recitals, performances,
conversations and
fieldtrips. For toddlers, twos, preschoolers, and kindergartners,
the schedule should
provide time for creative expression, large and small group
activities, and child-
initiated activities. Some learning opportunities, experiences, or
projects should extend
over the course of several days.
81. The classroom materials and equipment used to implement the
curriculum (books,
music, dolls, puzzles, toys, dramatic play props) should be
representative of the lives
of the enrolled children and their families. Curriculum materials
should also represent
the diverse cultures, languages, ages, abilities, and genders
found in society as a whole.
Include materials and equipment that accommodate children’s
individual needs
and special needs. Examples of individual needs include
culturally relevant dietary
or clothing practices, and family circumstances such as poverty,
homelessness, and
parental military deployment.
Each class environment should contain a rich variety of things
to engage young
learners. All classroom materials and equipment should provide
for children’s safety
while also being appropriately challenging. Look for toys and
other materials that are
interactive and encourage exploration, experimentation, and
discovery. To encourage
and support independent use, classroom materials and
equipment must be readily
accessible to children. To support children’s developing
interests and skill levels,
materials and equipment can change over time to reflect current
curriculum concepts
and content.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
82. 22
The materials and equipment used to implement the curriculum
in infants’, toddlers’,
and twos’ classrooms should encourage exploration,
experimentation, and discovery
and promote physical development through self-initiated
movement.
2.B—Social and Emotional Development
Topic 2.B addresses formal and informal plans as well as
opportunities for
fostering children’s healthy social and emotional growth
through the development
of friendships, self-regulation skills, empathy, and the ability to
resolve conflict in
positive ways.
Recommended Best Practices
All children have varied opportunities to engage throughout the
day with teaching
staff who are attentive and responsive to them and who
facilitate their social
competence and their ability to learn through interacting with
others. Children
have varied opportunities to recognize and name their feelings
and the feelings of
others. Children have varied opportunities to learn the skills
needed to regulate their
emotions, behavior, and attention. Children have varied
opportunities to develop
a sense of competence and positive attitudes toward learning,
such as persistence,
engagement, curiosity, and mastery.
83. Toddlers and older children have varied opportunities to
develop skills for entering
into social groups, developing friendships, learning to help, and
using other prosocial
behaviors. Children have varied opportunities to interact
positively, respectfully, and
cooperatively with others; learn from and with one another; and
resolve conflicts
in constructive ways. Children have varied opportunities to
learn to understand,
empathize with, and take into account other people’s
perspectives.
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
23
2.C—Physical Development
Topic 2.C addresses program plans, materials, and equipment
for the support of
children’s large motor development.
Recommended Best Practices
Young children achieve mastery of their bodies through self-
initiated movement.
For infants, toddlers, and twos, gross motor development is
promoted by providing
an environment that allows them to move freely. Babies and
toddlers need to have
many different kinds of opportunities to practice emerging
skills in coordination,
84. movement and balance, and sensory–motor integration through
activities such
as stacking blocks or rings, crawling through tunnels, copying
visual cues, or
completing simple puzzles.
Preschoolers and kindergartners should be given equipment they
can use to
engage in large motor experiences that stimulate a variety of
skills. Their physical
development goals are to develop balance, strength, and
coordination and to enhance
sensory–motor integration. These older children need physical
experiences ranging
from familiar to new and challenging such as traffic cone bike
courses, impromptu
obstacle courses, and sprinklers. It is time for them to learn
physical games that have
rules and structure (such as hokey pokey, Simon says, red
light/green light). Children
with varying abilities must be able to have large motor
experiences similar to those of
their peers.
Fine motor development (e.g., controlled twisting or turning of
the wrists, pouring
liquids, fastening clothing, writing) proceeds when young
children have many
different developmentally appropriate opportunities to use their
hands and fingers to
act on their environment.
2.D—Language Development
Topic 2.D addresses program plans and materials for supporting
children’s
language development. The goals and objectives for language
85. acquisition address
both verbal and nonverbal communication and are rooted in
ethnic and other
community traditions.
Recommended Best Practices
The curriculum must provide all children with opportunities for
language acquisition
that align with the program’s philosophy of education and
include consideration
of family and community perspectives. For example, children
should be able to
experience oral and written communication in a language their
family uses or
understands. Children should also have opportunities to hear
their families’ preferred
terminology (e.g., pronouns, body parts or functions, or familial
relationships)
included in classroom use. Additionally, experiences featuring
local or regional
terminology for geographic or architectural features, community
specific industry, and
NAEYC Early Learning Program Accreditation Standards and
Assessment Item
24
other specific ethnic or cultural terminologies in their
community is sometimes used
in relevant learning opportunities. Children need a variety of
opportunities to develop
competence in verbal and nonverbal communication by
86. responding to questions;
communicating needs, thoughts, and experiences; and
describing things and events.
Toddlers and older children should have experiences that
develop vocabulary, such
as participating in conversations and field trips and hearing and
reading books. The
curriculum and learning environment should create
opportunities for children to have
discussions with teachers or with each other. For instance, these
can be discussions
about solving interpersonal problems or solving problems
related to the physical world
(e.g., how to retrieve a ball that has gone over a fence, using
ramps to make cars go
faster or further, putting puzzles together).
If toddlers and older children are nonverbal, staff should know
how to use alternative
communication strategies with these children.
2.E—Early Literacy
Topic 2.E addresses program plans and materials for supporting
early literacy
through reading, learning letters and sounds, writing, and
immersion in a print-
rich environment.
Recommended Best Practices
Literacy development needs to be an element of all early
curricula, including those
of infants and toddlers. Literacy starts when infants, toddlers,
and 2-year-olds have
chances to experience talk, songs, rhymes, routine games (e.g.,
Patty-Cake, peek-
87. a-boo, Itsy bitsy Spider), and books. Staff convey language to
individual young
ones using simple rhymes, songs, and interactive games (e.g.,
peek-a-boo), some
of which include sequences of gestures (e.g., where is
Thumbkin). Every day, little
ones should get to hear and respond to various types of books,
including picture
books, wordless books, and books with rhymes. They need to
have regular access to
durable books they can explore on their own. Toddlers and twos
should start to have
experiences that help them understand that pictures can
represent real things in
their environment.
Toddlers and older children need to be given many
opportunities to become familiar
with print. Help them become actively involved in making sense
of print by having
print throughout the classroom. Items belonging to a child
should be labeled with
his or her name. Materials are labeled, and print is used to
describe some rules
and routines. Teaching staff should help children recognize
print and connect it to
spoken words.
Preschool and kindergarten children should have books read to
them at least twice
a day in full-day programs, and at least once daily in half-day
programs. Children
must be able to explore books on their own and have places that
are conducive to the
quiet enjoyment of books. The book selection should include
various types of books,
88. NAEYC Early Learning Program Accreditation Standards and
Assessment Item
25
including storybooks, factual books, books with rhymes,
alphabet books, number/
counting books, and wordless books. Teachers should read in an
engaging manner,
sometimes to individual children, sometimes to small groups
(two to six children),
and sometimes to large groups. They should help children
identify the various parts
of books such as the cover, title page, spine, beginning and
ending and differentiate
print from pictures. Some books should be read on repeated
occasions, and children
should have chances to retell and reenact events in storybooks.
The curriculum
should link books to other topics in the curriculum.
Preschool and kindergarten children should have multiple and
varied opportunities
to write. For instance, a variety of materials and experiences in
the classroom must be
provided to help them recognize and write letters of the
alphabet. Letters and words
can be posted at eye level or put on laminated cards (or both).
Books and writing
materials and activities should be readily available in art,
dramatic play, and other
learning centers. Various types of writing are supported,
including scribbling, letter-