
Recommended
Recommended
More Related Content
Similar to Primary Care Integration in Rural AreasA Community-Focused .docx
Similar to Primary Care Integration in Rural AreasA Community-Focused .docx (20)
More from LacieKlineeb
More from LacieKlineeb (20)
Recently uploaded
Recently uploaded (20)
Primary Care Integration in Rural AreasA Community-Focused .docx
- 1. Primary Care Integration in Rural Areas: A Community-Focused Approach Emily M. Selby-Nelson, PsyD Cabin Creek Health Systems, Charleston, West Virginia Joshua M. Bradley, PsyD Tri-Area Community Health, Laurel Fork, Virginia Rebekah A. Schiefer, MSW Oregon Health & Science University Alysia Hoover-Thompson, PsyD Stone Mountain Health Services, Jonesville, Virginia Current and developing models of integrated behavioral health service delivery have proven successful for the general population; however, these approaches may not sufficiently address the unique needs of individuals living in rural and remote areas. For all communities to benefit from the opportunities that the current trend toward inte- gration has provided, it is imperative that cultural and contextual factors be considered determining features in care delivery. Rural integrated primary care practice requires specific training, expertise, and adjustments to service delivery
- 2. and intervention to best meet the needs of rural and underserved communities. In this commentary, the authors present trends in integrated behavioral health service delivery in rural integrated primary care settings. Flexible and creative strategies are proposed to promote in- creased access to integrated behavioral health services, while simultaneously address- ing patient care needs that arise as a result of the barriers to treatment that are prevalent in rural communities. Keywords: integrated behavioral health, integrated primary care, rural, rural health The need for integrated health care is well documented. Nearly 70% of primary care ap- pointments include issues associated with psy- chosocial factors (Gatchel & Oordt, 2003). Many patients would prefer to receive behav- ioral health services in their primary care pro- vider’s office, as opposed to a specialty mental health setting (Lang, 2005). Patients in primary care offices are also more likely to follow through with a behavioral health referral when that service is provided in the same office (Slay & McCleod, 1997). Overall, integrated behav- ioral health services have been shown to suc- cessfully enhance health care services and yield improvements in medical and behavioral health conditions (Kwan & Nease, 2013). Integrated care models may be especially im- pactful in areas where access to specialty care is
- 3. limited, such as rural communities. However, a discussion of the adjustments warranted when developing integrated behavioral health ser- vices in rural practice settings is all but absent in the literature. Significant treatment needs in ru- ral areas, combined with poor availability of referral-based services in rural communities, re- quire effective integrated primary care (IPC) to be provided in a flexible, patient-tailored, and community-focused manner. In this paper, we aim to outline the special considerations neces- sary for conducting IPC in rural communities wherein behavioral health providers (BHPs) may struggle to balance individual- and popu- This article was published Online First August 2, 2018. Emily M. Selby-Nelson, PsyD, Cabin Creek Health Sys- tems, Charleston, West Virginia; Joshua M. Bradley, PsyD, Tri-Area Community Health, Laurel Fork, Virginia; Re- bekah A. Schiefer, MSW, Department of Family Medicine, Oregon Health & Science University; Alysia Hoover- Thompson, PsyD, Stone Mountain Health Services, Jones- ville, Virginia. Correspondence concerning this article should be ad- dressed to Emily M. Selby-Nelson, PsyD, Cabin Creek Health Systems, Sissonville Health Center, 1635 Sissonville Drive, Charleston, WV 25312. E-mail: [email protected] .com T hi s do
- 8. y. Families, Systems, & Health © 2018 American Psychological Association 2018, Vol. 36, No. 4, 528–534 1091-7527/18/$12.00 http://dx.doi.org/10.1037/fsh0000352 528 mailto:[email protected] mailto:[email protected] http://dx.doi.org/10.1037/fsh0000352 lation-based demands. As a diverse group of BHPs working in four different rural primary care clinics, we plan to provide insights and guidance into the nuances of rural IPC. Rural Communities Vulnerabilities Significant mental health disparities exist be- tween rural residents and urban dwellers in the United States. Rural residents remain dispropor- tionately at risk for suicide (Hirsch & Cukrow- icz, 2014), substance abuse, and chronic illness (Wagenfeld, 2003). Rates of mood and anxiety disorders, trauma, and developmental and psy- chotic disorders are at least as high as the rates in urban areas (Roberts, Battaglia, & Epstein, 1999). Further, high rates of mental health co- morbidities exist in this population (Smalley et al., 2010). The impact of these disparities on the
- 9. daily functioning of rural residents is magnified by barriers to availability, accessibility, and ac- ceptability of mental health treatment (Human & Wasem, 1991; U.S. Department of Health & Human Services, 2005). Availability Many rural areas have few, if any, mental health providers (Helbok, Marinelli, & Walls, 2006; Schank & Skovholt, 2006), with 60% of rural Americans living in mental health profes- sional shortage areas (U.S. Department of Health and Human Services, 2012). Rural com- munity health centers often are smaller because of dispersed population and therefore may have fewer medical providers (Rosenblatt & Hart, 2000; U.S. Department of Health and Human Services, Health Resources and Services Ad- ministration, 2012). Accessibility Residents of rural communities may face a multitude of social and environmental chal- lenges which include limited access to employ- ment, scarce resources, high poverty rates, less formal education, and higher illiteracy rates (Campbell, Kearns, & Patchin, 2006; Wagen- feld, 2003). These challenges have the potential to limit awareness of when services are needed, what is available, and how to use those services (Smalley et al., 2010). Mental health services may be difficult to access because of a dearth of public transportation, financial burden associ-
- 10. ated with maintaining a personal vehicle, and transportation complications related to chal- lenging geographic terrain and seasonal weather further exacerbating existing access issues. Acceptability Factors contributing to lower acceptability of mental health services among rural populations include increased stigma and decreased ano- nymity in using mental health services (U.S. Department of Health & Human Services, 2005). These perceptions represent risk factors that may influence participation in health care and mental health services (Bradley, Werth, Hastings, & Pierce, 2012; Schank & Skovholt, 2006). Rural individuals may possess strong kinship ties with family residing in the same community, a tendency toward family based support, hesitancy to share personal information with strangers or professionals (Bradley et al., 2012), and a strong sense of self-reliance that can be a potential barrier preventing outsiders from gaining the trust of community members (Schank & Skovholt, 2006). As a result of these barriers to mental health care, rural Americans use primary care providers (physicians and other medical providers) for behavioral and mental health services more than their urban counterparts (Crosby, Wendel, Vanderpool, & Casey, 2012). Rural Integrated Primary Care Existing and emerging models of integrated behavioral health, although effective for many
- 11. primary care patients, may insufficiently ad- dress the needs of individuals living in rural and underserved areas where mental health treat- ment availability, accessibility, and acceptabil- ity are low. Rural integrated primary care re- mains true to the philosophy of behavioral health integration, while adjusting service de- livery to suit the unique needs of rural commu- nities through population-based care in the con- text of underserved settings. Similar to BHPs in urban settings, rural BHPs tend to have various roles and responsibilities, including behavioral health consultant, psychotherapist, educator or trainer, scholar, administrator, and leader. To complicate matters, rural BHPs often practice 529PRIMARY CARE INTEGRATION IN RURAL AREAS T hi s do cu m en t is co py ri
- 15. an d is no t to be di ss em in at ed br oa dl y. these roles across multiple clinics throughout their rural health care system, with each clinic striving to meet distinct needs in different com- munities. BHPs practicing in multiple clinics may have practices that vary by site, requiring flexibility and heterogeneity in practice style. Because of the typical absence of specialty mental health treatment options, rural integra-
- 16. tion warrants the inclusion of resources beyond in-person treatment such as distance access ap- proaches to adequately address the depth, breadth, and magnitude of mental health needs of rural residents. Rural integrated primary care leads BHPs to strike a balance between answering the consul- tation needs of a primary care clinic and the greater community’s need for continued longer term services. This task is challenging as BHPs risk overbooking their schedule with follow-up care, adversely affecting their open access availability. Current integrated primary care models are based strongly on the expectation of, and reliance on, referrals to specialty mental health services. However, such referrals are typ- ically impractical, if not impossible, because of the dearth of accessible mental health services in rural areas. As a result of the underserved nature of rural areas, individuals seeking care in these regions may present with mental health problems that have gone untreated for some time, leading an integrated BHP to treat patients who have sig- nificant mental health needs with either limited access or no access to mental health referral options. BHPs face the decision to provide more traditional mental health care with evidence- based interventions in the primary care setting, or to refer when options are available and hope the patient completes the referral despite treat- ment barriers.
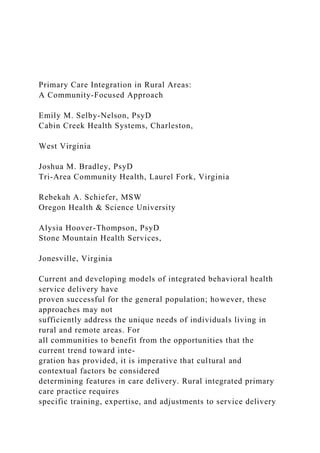
- 17. Community-Focused Practice Implications In their June 2016 commentary Mauksch and Fogarty discussed their vision for a “perennial philosophy” to guide the field of integrated be- havioral care as it moves forward. Their philos- ophy highlights the central value of maintaining flexibility in delivering services to meet the unique needs of a variety of primary care pa- tients (Mauksch & Fogarty, 2016). We similarly believe that flexibility in service delivery is a central component to providing integrated be- havioral health services in rural settings, as each rural community may have specific needs and differing cultural and accessibility consider- ations. A flexible and community-focused ap- proach to IPC requires awareness of the follow- ing practice domains and adjustments: provider ratio, sustainability of billing practices, gener- alist practice and ethical considerations, and flexible structure of behavioral health service delivery (see Figure 1). Ratio of BHP to Medical Provider in Rural Practice The balance of the number of medical and behavioral health providers is pertinent to the Features of Urban-based Integrated Behavioral Health Features of Rural Community-Focused Integrated Behavioral Health
- 18. • Model based (fixed) • Population based • Appointments are 30 minutes or less • Clinic patients only • High severity referred to specialty mental health • Collaboration primarily within clinic • 1 BHP to 3-4 PCPs • Treatment duration typically 1-6 visits • Bill Health and Behavior codes • Focus on health issues, health behavior change and mental health • Need based (flexible) • Population and community based • Appointments determined by patient need and provider availability • May accept outside referrals • High severity may be treated by BHP • Collaboration within clinic and community • No standard ratio of BHPs and PCPs • Treatment duration based on patient need • Bill Health and Behavior and Psychotherapy codes • Focus on health issues, health behavior change, mental health, advocacy, disaster relief, crisis work and some case management Figure 1. Summary of contrasting features of urban and rural integrated behavioral health services. 530 SELBY-NELSON ET AL.
- 23. ed br oa dl y. success and sustainability of an IPC practice. In brief, IPC models the ratio of BHPs to medical providers is 1:3–4 (Robinson & Reiter, 2015). It is alleged that this ratio allows a BHP to remain productive with both warm-handoff in- troductions and follow-up appointments with existing clinic patients. Although some rural clinics may be able to sustain a relatively large number of medical providers, many rural clinics are staffed with fewer than 3–4 PCPs. This staffing scenario may result in a lower provider ratio between BHP and PCP, therefore the role and scope of the BHP is broadened to compen- sate for the smaller amount of referrals expected from a sole practitioner. A rural BHP concerned about sustainability should consider augmenting their productivity by taking self-referred clients from the commu- nity who are only seeking mental health ser- vices and make a reverse referral to their med- ical provider colleague when that patient does not have an existing PCP. In this instance, a patient may initially establish care with a clinic for behavioral health service only, later becom-
- 24. ing a primary care patient to access medical care. It is additionally recommended that rural BHPs consider adding more scheduled patients throughout their day to offset downtime when they are not consulting with the medical pro- vider. Sustainability of Integration Sustainability remains a barrier for some pri- mary care practices who wish to integrate be- havioral health services but struggle with how to develop payment and reimbursement systems that cover the cost of nonmedical staff (Kathol, Butler, McAlpine, & Kane, 2010). This situa- tion can be especially challenging for smaller practices with smaller budgets, where a BHP’s salary significantly impacts the practice budget. We are familiar with some integrated practices who have chosen to primarily use health and behavior billing codes that provide reimburse- ment for behavioral health services under the medical portion of a patient’s insurance plan. However, these codes yield relatively small re- imbursements and are not uniformly reimbursed (Kessler, 2008), especially in small rural prac- tices where the BHP may only see a few pa- tients whose primary issues are appropriately represented by a health and behavior code. Psy- chotherapy codes reimburse at a higher rate comparatively. These codes may be considered for rural integrated practices where the demand for psychotherapy is present, where there are limited mental health services available, or when underutilization is a problem (Rost, Fort-
- 25. ney, Fischer, & Smith, 2002). Consideration of the payer mix for behavioral health reimbursement is important, as reim- bursement varies state by state. A BHP may find that there are extra steps to access Medicaid reimbursement for psychotherapy, requiring billing consultation. Rural BHPs may expect more consistent reimbursement from Medicare and private insurances, and additionally, may need to consider negotiating a sliding scale for uninsured individuals in the community, or for patients who do not have mental health cover- age. In our experience, BHPs can achieve sus- tainability with a community-focused approach by using a combination of strategic scheduling, using both types of billing codes, negotiating individual contracts of enhanced payment for integrated services through Medicaid, and serv- ing as a training site for psychology, counseling, and social work students and interns. Rural IPC clinics may be able to expand access to address some behavioral health needs through the inclusion of other helping profes- sionals or trainees like medical family therapists and bachelors level health and wellness coaches (Jordan & Livingstone, 2013). However, psy- chologists and licensed clinical social workers are the only behavioral health providers ap- proved for Medicare reimbursement, an insur- ance type held by many rural health care con- sumers. This population may go untreated if accessing services at sites struggling to hire those particular BHP types.
- 26. Generalist Practice and Ethical Considerations The wide variety of behavioral health con- cerns treated in primary care requires that any successful BHP have solid generalist training, paralleling the generalist demands of PCP prac- tice. Because of the diverse needs of under- served rural populations, we believe that BHPs in rural settings need to be able to provide generalist services, while also being capable of effectively delivering specialty mental health care in children, adults, and elderly populations 531PRIMARY CARE INTEGRATION IN RURAL AREAS T hi s do cu m en t is co py ri gh te
- 30. is no t to be di ss em in at ed br oa dl y. with conditions ranging from mild to severe. Although the rural and urban BHP may ap- proach consultation and brief interventions sim- ilarly, the rural BHP may need to provide addi- tional longer term services for a variety of populations who are unable to access more in- tensive care. Along with treating a wide variety of patients with varying clinical presentations, BHPs in
- 31. rural settings encounter unique ethical issues. Dual relationships, conflicting roles, and prac- ticing at the limits of one’s scope of competence are all issues commonly experienced by rural mental health providers (Roberts et al., 1999). According to Schank (1998), rural community expectations and standards may contribute to ethical dilemmas that conflict with professional codes and guidelines. Whereas urban BHPs can more readily consult specialists and refer tradi- tional or intensive mental health cases to spe- cialty mental health, rural BHPs may be faced with consulting and treating conditions with which they have limited experience, or face turning the patient away. Because of the closeness of rural community members and the potential for dual relationships that occurs when community members are also clinic staff, navigating issues related to confi- dentiality and dual roles can lead to unique ethical conflicts in rural IPC. We believe that BHPs preparing for, or currently in, rural prac- tice may not see their ethical issues adequately reflected in much of the literature about inte- grated care or in the general application of their professional ethics code. The American Psycho- logical Association’s Committee on Ethics and Committee on Rural Health are working toward more practice-based guidance for ethical deci- sion making across practice settings and popu- lation diversity (including geographic location) that will ideally resolve this area of growth in our field. Rural BHPs are advised to routinely consult colleagues with expertise in ethics and rural practice to remain prepared to face the
- 32. ethical issues regularly experienced in rural practice. Technological Bridges to Specialty Care Innovations in consultation and education in- cluding telehealth, Extension for Community Health Care Outcomes (Project ECHO), and the hub-and-spoke model have provided additional support and training to rural practitioners who may otherwise face professional and educa- tional isolation. These programs can offer con- tinued guidance to support PCPs and BHPs when treating cases that challenge their compe- tency limits and generalist model. Tele- psychiatry provides the opportunity to integrate specialty psychiatric treatment. The AIMS cen- ter at the University of Washington provides excellent examples of how telehealth can be used to provide effective and evidenced based treatments for chronic conditions, like the pro- tocol driven Collaborative Care Model (Gil- body, Bower, Fletcher, Richards, & Sutton, 2006). The Collaborative Care Model has demon- strated meaningful outcomes for the treatment of depression and anxiety (Archer et al., 2012) and should be considered along with other tele- health services in rural communities where ac- cess to psychiatry is often very limited (Hilty et al., 2006). BHPs may consult, facilitate, and engage in co-management during psychiatry telehealth, bridging the access gap to psychiat- ric treatment typically found in rural areas. Al-
- 33. though the function of the BHP differs within a collaborative care model as opposed to a con- sultant model, both can be used in combination and tailored to meet the needs of a clinic pop- ulation. Frequency and Structure of Behavioral Health Services BHPs in rural practice may consistently need to balance their range of services within the context of their community population, which includes special attention to session frequency. Some models of integration provide firm guide- lines for the frequency of behavioral health vis- its (Robinson & Reiter, 2015). In our experi- ence, flexibility in the length and range of behavioral health visits is congruent with the needs of rural communities and does not nec- essarily negatively influence the BHP’s avail- ability to provide integrated services and con- sultation to the primary care team. For example, recent data from one of our practice sites in rural Virginia demonstrated an average of 4.5 behavioral health visits among referred patients during 2015, with single visits removed from the data. However, the session range extended to 42 visits, demonstrating the BHP flexibility 532 SELBY-NELSON ET AL. T hi s do
- 38. y. for a small amount of patients requiring more intensive care. Another of our practice sites in rural Oregon produced similar data in 2016, with an average of 4 visits for each person seen in behavioral health. The behavioral health team in this clinic was able to see nearly 10% of the total clinic population, while not restricting the number of visits for patients needing longer term mental health services. Just as BHPs in all practices must achieve a balance of consultation and direct patient care, each practice may employ differing strategies to increase BHP availability. Based on our collec- tive experience, we have observed success in achieving behavioral health access by setting an intentional culture of flexibility for behavioral health services with both patients and primary care team colleagues. For example, BHPs work- ing alone and who are dedicating some of their practice to psychotherapy may prepare their pa- tients for the possibility of interruptions for urgent consultation needs. The BHP may carry a pager or use a messaging system based in the electronic health record to ensure easy and ac- cessible communication with other providers. Each practice and individual BHP may adapt the range of services they provide to their com- munity based upon need. For example, some patients may need advocacy around legal prob- lems or help with case management and navi-
- 39. gating social services systems. Some primary care psychologists may offer psychological test- ing when patients cannot receive those services in their community. In our experience, achiev- ing and maintaining this level of flexibility in service delivery and structure requires inten- tional and ongoing evaluation of processes to monitor for needed changes and improvement, as well as constant communication with mem- bers of the primary care team. Conclusion The integration of behavioral health services into primary care settings promotes access to quality care for people of all communities and minimizes barriers to treatment. Cultural and contextual factors are necessary considerations in the design and implementation of integrated primary care delivery in rural settings. Mauksch and Fogarty (2016) described the importance of flexibility in meeting the needs of the range of patients that may present in primary care, which is amplified when considering patients living in rural communities. As a result of the unique practice implications inherent in rural health care settings, adjustments in the IPC model de- sign are necessary to best meet the needs of these underserved communities. Literature offering guidance on the imple- mentation of alternative models or adjusting behavioral health care service in primary care models has been limited to date. It is recom- mended that IPC education and research initia-
- 40. tives further investigate and disseminate infor- mation and best practices in this area to promote competence in rural IPC practice. Such ad- vancement in knowledge may promote recruit- ment and retention of behavioral health provid- ers in rural IPC settings, minimize the risk of burnout, and lead to increased access to behav- ioral health services. References Archer, J., Bower, P., Gilbody, S., Lovell, K., Rich- ards, D., Gask, L., . . . Coventry, P. (2012). Col- laborative care for depression and anxiety prob- lems. Cochrane Database of Systematic Reviews, 10, CD006525. Bradley, J. M., Werth, J. L., Jr., Hastings, S. L., & Pierce, T. (2012). A qualitative study of rural men- tal health practitioners regarding the potential pro- fessional consequences of social justice advocacy. Professional Psychology: Research and Practice, 43, 356–363. http://dx.doi.org/10.1037/a0027744 Campbell, C. D., Kearns, L. A., & Patchin, S. (2006). Psychological needs and resources as perceived by rural and urban psychologists. Professional Psy- chology: Research and Practice, 37, 45–50. http:// dx.doi.org/10.1037/0735-7028.37.1.45 Crosby, R. A., Wendel, M. L., Vanderpool, R. C., & Casey, B. R. (2012). Rural populations and health. San Francisco, CA: John Wiley & Sons Inc. Gatchel, R. J., & Oordt, M. S. (2003). Clinical health psychology and primary care: Practical advice
- 41. and clinical guidance for successful collaboration. Washington, DC: APA Books, American Psycho- logical Association. http://dx.doi.org/10.1037/ 10592-000 Gilbody, S., Bower, P., Fletcher, J., Richards, D., & Sutton, A. J. (2006). Collaborative care for depres- sion: A cumulative meta-analysis and review of longer-term outcomes. Archives of Internal Medi- cine, 166, 2314–2321. http://dx.doi.org/10.1001/ archinte.166.21.2314 Helbok, C. M., Marinelli, R. P., & Walls, R. T. (2006). National survey of ethical practices across rural and urban communities. Professional Psy- 533PRIMARY CARE INTEGRATION IN RURAL AREAS T hi s do cu m en t is co py ri
- 46. dx.doi.org/10.1037/0735-7028.37.1.36 Hilty, D. M., Yellowlees, P. M., Cobb, H. C., Bour- geois, J. A., Neufeld, J. D., & Nesbitt, T. S. (2006). Models of telepsychiatric consultation—Liaison service to rural primary care. Psychosomatics: Journal of Consultation and Liaison Psychiatry, 47, 152–157. http://dx.doi.org/10.1176/appi.psy .47.2.152 Hirsch, J. K., & Cukrowicz, K. C. (2014). Suicide in rural areas: An updated review of the literature. Journal of Rural Mental Health, 38, 65–78. http:// dx.doi.org/10.1037/rmh0000018 Human, J., & Wasem, C. (1991). Rural mental health in America. American Psychologist, 46, 232–239. http://dx.doi.org/10.1037/0003-066X.46.3.232 Jordan, M., & Livingstone, J. B. (2013). Coaching vs psychotherapy in health and wellness: Overlap, dissimilarities, and the potential for collaboration. Global Advances in Health and Medicine, 2, 20– 27. http://dx.doi.org/10.7453/gahmj.2013.036 Kathol, R. G., Butler, M., McAlpine, D. D., & Kane, R. L. (2010). Barriers to physical and mental con- dition integrated service delivery. Psychosomatic Medicine, 72, 511–518. http://dx.doi.org/10.1097/ PSY.0b013e3181e2c4a0 Kessler, R. (2008). Integration of care is about money too: The health and behavior codes an element of a new financial paradigm. Families, Systems, & Health, 26, 207–216. http://dx.doi.org/10.1037/ a0011918
- 47. Kwan, B. M., & Nease, D. E. (2013). The state of the evidence for integrated behavioral health in pri- mary care. In M. R. Talen & A. B. Valeras (Eds.), Integrated behavioral health in primary care: Evaluating the evidence, identifying the essentials. New York, NY: Springer. http://dx.doi.org/10 .1007/978-1-4614-6889-9_5 Lang, A. J. (2005). Mental health treatment prefer- ences of primary care patients. Journal of Behav- ioral Medicine, 28, 581–586. http://dx.doi.org/10 .1007/s10865-005-9019-2 Mauksch, L. B., & Fogarty, C. T. (2016). In search of a perennial philosophy for behavioral health inte- gration in primary care. Families, Systems, & Health, 34, 79– 82. http://dx.doi.org/10.1037/ fsh0000196 Roberts, L. W., Battaglia, J., & Epstein, R. S. (1999). Frontier ethics: Mental health care needs and eth- ical dilemmas in rural communities. Psychiatric Services, 50, 497–503. http://dx.doi.org/10.1176/ ps.50.4.497 Robinson, P., & Reiter, J. T. (2015). Behavioral consultation and primary care: A guide to inte- grating services (2nd ed.). Cham, Switzerland: Springer International Publishing. Rosenblatt, R. A., & Hart, L. G. (2000). Physicians and rural America. The Western Journal of Medi- cine, 173, 348–351. http://dx.doi.org/10.1136/ ewjm.173.5.348
- 48. Rost, K., Fortney, J., Fischer, E., & Smith, J. (2002). Use, quality, and outcomes of care for mental health: The rural perspective. Medical Care Re- search and Review, 59, 231–265. http://dx.doi.org/ 10.1177/1077558702059003001 Schank, J. A. (1998). Ethical issues in rural counsel- ing practice. Canadian Journal of Counselling, 32, 270–283. Schank, J. A., & Skovholt, T. M. (2006). Ethical practice in small communities: Challenges and rewards for psychologists. Washington, DC: American Psychological Association. http://dx.doi .org/10.1037/11379-000 Slay, J. D., & McCleod, C. (1997). Evolving an integration model: The Healthcare partners expe- rience. In N. A. Cummings, J. L. Cummings, & J. N. Johnson (Eds.), Behavioral health in primary care: A guide for clinical integration (pp. 103– 120). Madison, CT: Psychological Press. Smalley, K. B., Yancey, C. T., Warren, J. C., Naufel, K., Ryan, R., & Pugh, J. L. (2010). Rural mental health and psychological treatment: A review for practitioners. Journal of Clinical Psychology, 66, 479–489. U.S. Department of Health and Human Services. (2005). Mental health and rural America: 1994– 2005. Rockville, MD: Office of Rural Health Pol- icy, Health Resources and Services Administra- tion. U.S. Department of Health and Human Services,
- 49. Health Resources and Services Administration. (2012). Designated health professional shortage areas (HPSA) Statistics. Rockville, MD: Health Resources and Services Administration, Office of Shortage Designation. Wagenfeld, M. O. (2003). A snapshot of rural and frontier America. In R. L. Stamm (Ed.), Rural behavioral health care: An interdisciplinary guide (pp. 33–40). Washington, DC: American Psycho- logical Association. http://dx.doi.org/10.1037/ 10489-002 Received October 16, 2017 Revision received February 3, 2018 Accepted February 7, 2018 � 534 SELBY-NELSON ET AL. T hi s do cu m en t is co py
- 54. http://dx.doi.org/10.1097/PSY.0b013e3181e2c4a0 http://dx.doi.org/10.1097/PSY.0b013e3181e2c4a0 http://dx.doi.org/10.1037/a0011918 http://dx.doi.org/10.1037/a0011918 http://dx.doi.org/10.1007/978-1-4614-6889-9_5 http://dx.doi.org/10.1007/978-1-4614-6889-9_5 http://dx.doi.org/10.1007/s10865-005-9019-2 http://dx.doi.org/10.1007/s10865-005-9019-2 http://dx.doi.org/10.1037/fsh0000196 http://dx.doi.org/10.1037/fsh0000196 http://dx.doi.org/10.1176/ps.50.4.497 http://dx.doi.org/10.1176/ps.50.4.497 http://dx.doi.org/10.1136/ewjm.173.5.348 http://dx.doi.org/10.1136/ewjm.173.5.348 http://dx.doi.org/10.1177/1077558702059003001 http://dx.doi.org/10.1177/1077558702059003001 http://dx.doi.org/10.1037/11379-000 http://dx.doi.org/10.1037/11379-000 http://dx.doi.org/10.1037/10489-002 http://dx.doi.org/10.1037/10489-002Primary Care Integration in Rural Areas: A Community-Focused ApproachRural CommunitiesVulnerabilitiesAvailabilityAccessibilityAcceptabili tyRural Integrated Primary CareCommunity-Focused Practice ImplicationsRatio of BHP to Medical Provider in Rural PracticeSustainability of IntegrationGeneralist Practice and Ethical ConsiderationsTechnological Bridges to Specialty CareFrequency and Structure of Behavioral Health ServicesConclusionReferences Truman Doctrine Discussion 75 words when you are replying to another student and you must reply to at least one student. SHELIA’S POST: Truman Doctrine Discussion Truman announced that the United States must support Greece and Turkey in order to prevent them from becoming communist.
- 55. He said we must do this not because it would be nice for them, but because it was in the national security interest of the United States. What is the logic behind his argument? Do you find Truman's argument persuasive? Why or why not? The logic behind Truman's argument is support for anti- communist regimes was the primary reason of the foreign policy of the United States and other nations will be able to work free from coercion. Countries tried to impose their will and their way of life upon other nations. I find Truman's argument to be persuasive the U. S. took a leading part in establishing the United Nations to ensure peaceful development of lasting freedom and independence for all nations. Brown v. Board of Education Discussion 75 words when you are replying to another student and you must reply to at least one student. KIMBERLY’S POST: The Browns received a unanimous 9–0 decision from the Supreme Court in May 1954."Separate educational facilities are inherently unequal," the Supreme Court ruled, implying that laws imposing them violate the Equal Protection Clause of the United States Constitution. However, the Court's second decision in Brown II (349 U.S. 294 (1955)) only ordered states to desegregate "with all deliberate speed," and the 14 pages of the decision did not outline any method for ending racial segregation in schools. State-sanctioned segregation of public schools was a violation of the 14th Amendment and was therefore unconstitutional. This historic decision marked the end of the "separate but equal" precedent set by the Supreme Court nearly 60 years earlier and served as a catalyst for the expanding civil rights movement. It will still be unconstitutional because new research showed that segregating students by "race" was harmful to them, even if facilities were equal, "separate but equal" facilities were found to be unconstitutional in a series of Supreme Court decisions under Chief Justice Earl Warren, starting with Brown v. Board of
- 56. Education of 1954. Week 11 Assignment 2: DISCUSSION 2 What role has the arts (print and electronic media, including the movies and other forms of art played in advancing or reducing racist attitudes against people of color in America. Your responses must be no less that 200 words. Respond to at least two (2) of your classmates in no less than 100 words. KIMBERLIY’S POST: During the beginning stages of film and media, African Americans struggled to represent their own stories, beliefs, opinions, and identities because White people controlled the entertainment industry and chose what images of Black people to portray. Bias, disempowerment, and discrimination in regard to race have been longstanding issues within several aspects of mainstream media, including television news, entertainment, and advertising. During this beginning era of television, the population of those who worked in advertising, news and entertainment was predominantly White. As in most other non-menial employment in the United States, and likewise the perceptions and values held by this influential population, were reflected in produced media. How media content was formed, selected, and presented was heavily subjected to the opinions of those involved in the industry. Advertisements for products that were being marketed universally to the American public would still depict Caucasian people, leaving only the advertisements for products marketed for Black Americans to depict people of color. Since the early utilization of media, the impacts on how people are represented are imperative to understand how racism is perpetuated within our society. The media provides a greater understanding of historical context as well as patterns, influences, and beliefs around
- 57. generational media impacts: Throughout history, the mass media, in various forms, have tended to support the power of the dominant group by presenting to the general public highly negative, emotion- evoking images of minority groups. (Luther et al., 2012, p. 322) Luther, C., Ringer Lepre, C., & Clark, N. (2012). Diversity in U.S. Mass Media. Malden: Wiley- Blackwell. DONNA’S POST: I don't feel like it advance or reduce the attitudes against people of color in America. They bring awareness to racist but reducing it no, because it's too deep for most white people. As long as white people raised their children to continued to be racist against other races racist will continue. The white race is very strong and is built on a strong foundation. The media and the movies industry create movies about racist every year and it still exist. This will be a on going conversation until the end. The white and black race have been in conflict for many years and nothing has really change. The media are always having topic of racist against black people and also have events to encourage white policemen to come out and support and to get to know the black in the community that they patrol. There are white policemen that come out to support but only because they have to. These are the same white policemen that will kill a black person without any hesitation. When the black artist get involved it's a responses from the white community that they kill their own people and nothing is done, but when a white man kills a black man they come out and try do everything they can to bring it to the media. Week 11 Assignment 3: Short Essay The concept of the aesthetic. "The concept of the aesthetic descends from the concept of taste." In a short essay explain how the concept of taste affects how we view beauty? (300 words) Truman Doctrine Discussion All primary discussion posts must be 100 words or more and at
- 58. least 75 words when you are replying to another student and you must reply to at least one student. Truman announced that the United States must support Greece and Turkey in order to prevent them from becoming communist. He said we must do this not because it would be nice for them, but because it was in the national security interest of the United States. What is the logic behind his argument? Do you find Truman's argument persuasive? Why or why not? *Will post peer posts once the original is posted. Cannot see until initial post is made* Brown v. Board of Education Discussion All primary discussion posts must be 100 words or more and at least 75 words when you are replying to another student and you must reply to at least one student. In the Supreme Court's Brown v. Board of Education opinion, the court dealt with whether or not separate could ever be equal (in other words, they pretended for the sake of argument that segregated facilities in the South were actually equal). Why would perfectly equal accommodations still be unconstitutional? *Will post peer posts once the original is posted. Cannot see until initial post is made*