1. Khade Grant EGRB 421 Final Project 11/30/2015
EGRB 421 Final Design Project
A Prosthetic Device Design Providing Natural Gait Movement for
Patients in Full-Leg Casts
Khade Grant
11/30/2015
2. Khade Grant EGRB 421 Final Project 11/30/2015
Abstract:
A fracture isa breakinthe continuityof abone.The tibiaisthe most commonly fracturedlong
bone inthe body (33% of all fracturesin the body).Afterafracture,the legisusuallyputina cast
dependingonthe type of tibial fracture.There are three kindsof tibial fractures:Tibial shaftfractures,
tibial plateaufractures,andtibial plafondfractures.Tibial shaftfractures,whichare the mostcommon
tibial fracture (93%of tibial fractures),occurbetweenthe knee andthe ankle.These fracturesrequire
the legto be put ina full-legcastforrecovery.Unsurprisingly,duringrecovery,mobilityisanissue for
those whohave fracturedtheirtibia.There are some currentsolutions;suchascrutches,knee-scooters,
or the iWalk 2.0; that have beenproposed toaddressthe mobilityissue,butthese fall shortof providing
those infull-legcastswitha natural walkingmotion orsufficientmaneuverability.Also,the requireduse
of handsheavilylimitsthe activitiesthe usercanperform duringmovementwhileusingmanyof these
mobilityaids. The proposeddesignsolutionconsists of anelectromechanical prostheticdevice which
consistsof twotitaniumalloypylons(rods) onthe leftandrightof the injuredleg.Bothrodsattach to a
mechanical knee oneachside andcontinue pastthe kneesandcome togethertoformone rod beneath
the patient’sfoot.The footportionof the device hasrubberonthe end topromote some ankle flexion
motion.The patientissupportedwithneoprenestraps.The device consistsof angularsensorsand
microprocessorsthatrelate the hipflexionangleduringeachstage of the humangait cycle to the knee
flexionangleatthe correspondingstage inthe gaitcycle.The outputsignal producedfromthe hip
flexionangleiscalibratedtoproduce the correspondingkneeflexionangle. First,anthropometricdata
was collectedfromthe CenterforDisease Control(CDC) formenandwomentodetermine the required
sizesanddimensionsof the device.Next,the material propertiesforvariousmaterialswereevaluated
and the optimummaterialswere selectedforuse inthe design.The requiredelectrical properties of the
mechanical knee were thenincorporatedintothe physical device.Afterfinalizingadesignmodel,the
device will undergostrengthtestingaswell asmotiontestingtodetermineif the model isasufficient
design.The final prototype will be able tosufficientlyprovide normal humangaitmovementtopeople
whoare confinedtofull legcasts.
3. Khade Grant EGRB 421 Final Project 11/30/2015
Introduction
A fracture isa breakinthe continuityof abone.Fracturesto the legare a verycommoninjury.
The tibiais the mostcommonly fracturedlongbone inthe body.Almost500,000 people fracture their
tibiaeachyear,makingup around33% of all fracturesin the body (Fields,2015). These fracturesare
oftenexpensiveasthe healthcare costfortibial fracturesrange from$11,686 to $25,556 perpatient
dependingonthe locationandseverityof fracture (Antonovaetal.2013). Aftera fracture,the legis
usuallyputina cast dependingonthe type of tibial fracture.There are three kindsof tibial fractures:
Tibial shaftfractures,tibial plateaufractures,andtibial plafondfractures.Tibial shaftfractures,which
are the mostcommon tibial fracture,occurbetweenthe kneeandthe ankle.These fracturesrequire the
legto be put ina full-legcastforrecovery.Tibial plateaufracturesoccurjustbelow the knee joint.These
require at-leastafull-legcastfor recoveryandare usuallythe worstkindof fracturesas theycan leadto
problemssuchasknee arthritisevenafterrecovery.Tibial plafondfracturesoccurat the bottomof the
shinaroundthe ankle joint.These fracturesare perhapsthe leastsevere,astheyonlyrequire alower
legcast.
Unsurprisingly,duringrecovery,mobilityisabigissue forthose whohave fracturedtheirtibia.
There are some currentsolutionstoaddressthe mobilityissue. These mainlyincludecrutches,knee-
scooters,andwheel chairs.These mobilityaidsoftendonotprovide sufficientmobilitytoitsusers. One
wayto ergonomicallymeasure the effectivenessof mobilityaidsistolookat if theyallow itsusersto
adequatelyperformthe instrumental activitiesof dailyliving(IADLs) andthe basicactivitiesof daily
living(BADLs).The IADLsare the complex skillsrequiredtolive independently.These include:shopping,
preparingmeals,usingthe telephone,home maintenance,managingmedications,driving,and
managingfinances:Crutchesare the mostcommonmobilityaid.Crutches,however,don’tgive the user
a natural walkingmotionorsufficientmaneuverability.The requireduse of handsheavilylimitsthe
typesof activitiesthe usercando duringmovement. Usingcurrentmobilityaids,aroundtwo-thirdsof
usershave significantlimitationsinone ormore of the IADLs (NCHS,1998). BADLs, such as walking,
climbingstairs,eating,puttingonclothes, andgroomingare alsosignificantlylimitedunderthe current
mobilityaids.Approximatelyone-thirdof the peoplewhouse mobilityaiddevicesneedassistance from
anotherpersoninperformingthe BADLscomparedtolessthan1% innon-users(NCHS,1998).
There isa needfora designthatprovidesenhanced mobility,ishands-free duringmotion,and
providesanatural walkingmotionduringrecovery.One recentinvention,the iWALK2.0,takesa stepin
the right direction.The userrestshis/herknee onapad whichisattachedto a mechanical legandhasa
strap on the thighto make itsecure.Thisallowsamore natural walkingmotionthananydevice
currentlyonthe market.However,there are some shortcomings.There isnoflexioninthe knee of the
mechanical leg,sothe walkingmotionisnotnatural.More importantly,since the kneemustbe bentin
orderto use the device,itcanonlybe usedbypatientswithlowerlegcasts.Onlytibial plafondfractures,
whichmake up onlyabout7% of tibial fractures,canbe treatedwitha lowerlegcast.Thisdevice cannot
be usedby 93% of the tibial fracture population.
The designsolutionshouldbe amechanical device that allowsnatural walkingmovementby
providingfull knee flexionandsufficientankleflexionfor patientsinfull-legcasts.The device shouldbe
hands-free andshouldallowfornormal walkingspeedsonrelativelyflatsurfaces.Inadditiontoa
natural walkingmotion,the device shouldprovidesufficientmobility,stability,andsafetytoitsusers.
The deliverablesforthisdevice are asfollows:
1. Electromechanical HingedKneeJoint:The knee-jointwill be microprocessorcontrolled.The
microprocessorwill analyze andinterpretsignalsfromknee-anglesensorsandmomentsensors.
4. Khade Grant EGRB 421 Final Project 11/30/2015
It will alsobe controlledusingpositionsensorsinthe knee usingsignalsfromanangularposition
sensoronthe hip.The knee jointwill produce the requiredknee flexionof the device.
(Calibratedspecificallytothe userpriorto injury,orcalibratedusingaverage gaitdatafrom a
storeddatabase obtainedduringtesting).
2. Rotary encoder:The rotaryencodermustaccuratelymeasure hipflexionangles.
3. Footstructure capable of plantar/dorsi ankle flexion:The mechanical ankle will furtherallowfor
betterapproximationof normal humangaitmovement.
4. Normal humangaitmovement data:Data consistingof natural humangaitmovement,including
hipand knee flexionanglesduringeachstage of gaitmovement.Thisdatawill be usedto
calibrate the device.
5. Final Prototype:A final prototype will be designedaftervariousalternative designsare
consideredandrigoroustestsare conducted.
Descriptionof Approach and Methods
DesignandSelectionCriteria
The firststepin the designprocesswastouse anthropometricdatatofithuman lowerlimbdimensions
to the design.Thismainlyincludedlookingatanthropometricdata.The productdesignisgenerallyfor
bothmenand women.Inorderto take intoaccount the varioussize differencesbetweenthe
population,aswell asthe differences betweenmenandwomen,the anthropometricdata
measurementsforthe 5th
,10th
, 15th
, 25th
, 50th
, 75th
, 85th
, 90th
, and 95th
percentilesforbothmenand
womenwere tabulatedandusedtodetermine the variousdimensionsof the designproduct.There
were three keymeasurementsusedinthissection.The firstwasthe upperleglengthincentimetersfor
malesandfemales20 yearsof age and older.The secondkeymeasurementwasthe knee heightin
centimetersformalesandfemales20yearsof age and older.The lastkeymeasurementwasthe mid-
thighcircumference incentimetersformalesandfemales20 yearsof age and older.Thisdimensionwas
usedforthe innercircumference of the topringof the mechanical legthatwouldfitaroundthe thighof
the user.The knee heightdimensionswere usedtodetermine where onthe mechanical legtoplace the
artificial knee thatwouldallowforrotation. Thisdatawasobtainedfromresourcessuchas the Centers
for Disease Control andPrevention(CDC).Additionally,itcould be experimentallyobtainedbythe
designers. The followingtable wasasample of the measurementsused.
Table 1. Anthropometric data in centimeters for relevant measures. Obtained from CDC (2008)
The anthropometricdatawas used todetermine the lengthsof the upperandlowerpylons,aswell as
the circumference of the legstrap.The 10th
, 50th
, and 95th
percentileswere usedtodeterminethe
dimensionsof three differentsizesforthe device.The upperpylonlengthwascalculatedusing
5. Khade Grant EGRB 421 Final Project 11/30/2015
approximatelythree-fourthsthe lengthof the upperleg.The lowerpylonlengthwasdeterminedusinga
measurementslightlylargerthanthe knee heightmeasurement.The strapdimensionswere determined
usinga measurementslightlysmallerthan the thighcircumference measurements.The dimensionsof
the device are shownin the final designsectionin table 3.
There were variousmaterialsthatwere consideredforthe designof the mechanical leg.Forthe
dual-pylons,aluminum, titanium,andsteel werethe materialsconsidered.Titanium(Ti-6Al-4V) was
chosenas the material because itisverystrongyetlightweight.The material propertiesof Titaniumare
providedbelow inFigure1.
Figure 1. Material Properties of Ti-6Al-4V (ASM, 1996)
Basedon the fatigue strengthof 240 MPa and the Shear Strengthof 550 MPa, andincludinga
safetyfactorof 5 as well asdesigningtothe 95th
percentile intermsof knee heightandbodymass,the
minimuminnerradiusdimensionforacylindrical pylonwithanouterradiusof 2 cm was determinedto
6. Khade Grant EGRB 421 Final Project 11/30/2015
be 1.61 cm. The calculationsof the dimensionsare shown inAppendix I. The sole of the device will be
fittedwithrubbertoprovide some natural ankle flexionduringmovement. A preliminarystresstestwas
conductedonthe device made of Ti-6AL-4V.The results (shownin Appendix III) confirmthatthe
selected materialissufficientforthisdesign.
The strappingon the upperlegismade from non-flexible vinyl linedwithneoprene.Neoprene is
a syntheticrubberthatpreventsslippageof the strapon the legandprovidessufficientbreathability
(Smith,1985). Use of non-flexible vinyl preventsthe strapfromstretching,thusholdingthe patientin
place.
Comparisonof Solutions
Three designconceptswere consideredforthisdevice.Allof the designsconsistedof arotary
encoderonthe hip.The rotary encoderdetectedthe angulardisplacementandsentthe resultingsignal
to a circuit inthe mechanical knee thatproducedacorrespondingoutputsignal.Thatoutputsignal was
usedas the inputto produce the desiredangularrotation.The firstconsidereddesignwasAlternative 1.
It useda single-turnpotentiometerasthe rotary encoder.Alternative 2wassimilartoAlternative1
exceptitusedan optical rotaryencoderinplace of the single-turnpotentiometer.Anoptical rotary
encoderusesa lightshiningontoa photodiode throughslitsinmetal todetectangulardisplacement.
Thisrotary encoderprovidesaveryslightincrease inaccuracybuta substantial increaseincost.Itis also
difficulttomaintainbecauseitisverysensitive todust. Alternative3,usedan OnAxisMagneticrotary
encoder.Thisencoderemploysthe use of a 2 pole neodymiummagnetrotatingoverthe centerof the
encoder.Thisencodercanbe veryinaccurate and was thusinsufficientforuse inthisapplication.The
alternative solutionswere scoredbasedonvariouscategories.The followingscoringchartwasusedto
selectthe bestalternative.The maximumpossiblescoresforeachcategoryrangedfrom3 (little
importance) to9 (maximumimportance). The designalternative withthe highestscore wasselected.
Table 2. Scoring Chart of DesignAlternatives
Specifications(possible points) Alternative1 Alternative2 Alternative3
Function(9) 9 9 9
Features(9) 9 9 8
Noveltyandcommercial potential (6) 6 6 6
Safety(9) 9 9 5
Human factors(9) 7 7 4
Maintenance (6) 6 4 5
Reliability(9) 8 9 4
Manufacturability(6) 5 5 5
7. Khade Grant EGRB 421 Final Project 11/30/2015
Regulatoryrequirements(9) 9 9 9
Cost (6) 6 2 6
Ease of use (9) 9 8 6
Comfort(6) 5 5 5
Lifetime (3) 3 2 2
Total (96) 91 84 74
Final Design
The final designconsistsof two titaniumalloypylons (rods) onthe leftandrightof the injured
leg.Bothrods attach to a mechanical knee oneachside.The pylonscontinue pastthe mechanical knees
and come togethertoform one rod beneaththe patient’sfoot.The footportionof the device has
rubberon the endto promote some ankle flexionmotion. The device hasmultiplestrapsmade of
neoprene aroundthe patient’s thighforsupport. The device consistsof sensorsthatrelate the hip
flexionangleduringeachstage of the humangaitcycle to the knee flexionangleatthe corresponding
stage in the gaitcycle.The final designhasarotary encoderattachedtothe patient’ship.A single-turn
potentiometerisusedasthe rotaryencoder.Itproducesan outputsignal correspondingtothe hip
flexionangle. The mechanical knee rotatesthe legsof the device usinggears.These gearsare
microprocessorcontrolled.The microprocessortakesaninputsignal producedfromthe single-turn
potentiometerandproducesanoutputsignal thatcausesthe gearsto rotate the legto the determined
angularposition. The outputsignal producedfromthe hipflexionangle iscalibratedtoproduce the
correspondingknee flexionangle. Inadditiontoknee flexion, the designalsogivesthe userthe option
to lockthe mechanical kneesin the anatomical positioninordertoallow users toclimbstairs.The
motiondesignsystemis onlybe forrelativelyflatsurfaces.Inordertoaccount forthe heightdifference
producedbythe mechanical leg,anelevatedshoe isprovidedandshouldbe wornbythe user. During
motionthe device willbe hands-free.
Belowisa model of the final device design,aswell asthe device onthe humanleginvariousstagesof
the gait cycle.
8. Khade Grant EGRB 421 Final Project 11/30/2015
Figure 2. SolidWorks Model of Prosthetic Design. (a) Isometric View. (b) Frontal View. (c) Sagittal View. (d) Isometric w/ person
model.
Figure 3. SolidWorks Motion Model of Prosthetic Device in Main Stages of the Human Gait Cycle
9. Khade Grant EGRB 421 Final Project 11/30/2015
As statedinthe methods,titanium alloy (Ti-6Al-4V) isthe material usedforthe pylons, andnon-flexible
vinyl linedwith neoprene isthe strappingmaterial forthe upperleg.
The dimensions andmeasurements of the device componentsare listedbelow intable 3.
Table 3. Dimensions and weight of major device components (from 50th percentile)
Length
(cm)
Outer Radius
(cm)
Inner Radius
(cm)
Weight
(lbs)
Upper
Pylon 38 1.5 0.875 1.73
Lower
Pylon 54.1 1.5 0.875 2.46
Foot
Section 8 N/A N/A 1.54
Straps 50 N/A N/A 0.5
The total weightof the device isestimatedtobe 10.5 lbs.The determination/calculationof the
dimensionsandweightof the majorcomponentsare shownin Appendix I.A materialspartslistisalso
shownin Appendix I.The strap issufficienttohold the weightof amale inthe 95th
percentile.The
minimumsurface areaof the strap was determinedusingthe weightand the ultimate stressof skin.The
ultimate stressof skinisaround20 MPa (Gallagher,2012). The area of the straps wasover800 timesthe
minimumrequiredarea. The calculationsare shownin Appendix I. Since the cross-sectional areaof the
thighincreaseswithheight,the non-flexible vinyl strapswon’tslipupthe thighwhenanupward
reactionforce isappliedtoitduringwalking.
The initial designdrawingsare shownin Appendix II.The drawingsconsistof the frontal and
lateral viewinthe anatomical position,andthe lateral viewof the device inthe middleof the gaitcycle.
Electrical Properties
The device consistsof a sensorplacedonthe hip.The sensorplacedonthe hipwill be arotary
encoder(angularpositionsensor).There are varioustypesof angularpositionsensorsthatcouldbe
used,butfor thisapplicationasingle turnpotentiometer (resistiverotaryencoder) shouldbe sufficient.
10. Khade Grant EGRB 421 Final Project 11/30/2015
Figure 4. Single turn potentiometer (Webster, 2009)
A single turnpotentiometer consistsof astationaryresistive andpowerelement andamovable
wiper.Itusesthe conceptof voltage divisiontoproduce varyingoutputvoltagesasa wipermovesalong
the resistor. Usingvoltage division,the outputvoltage Vo producedfromaconstantinputvoltage Vi is
givenby:
𝑽 𝒐 =
𝑹 𝟐
𝑹 𝟏+𝑹 𝟐
× 𝑽 𝒊 =
𝑹 𝟐
𝑹 𝒕𝒐𝒕𝒂𝒍
× 𝑽 𝒊.
As the wiperturnscounter-clockwiseR2 decreasesandthe outputvoltage decreases
proportionally.Forthe single-turnpotentiometerthe powerandresistive elementwillremainstationary
as it will be attachedtothe hipof the patient.The wiperwill be directlycontrolledbythe movementof
the femur.Thusas the hipflexesorextendsduringmovement,the wiperwillrotate andproduce a
correspondingvoltage change.Therefore,eachhipflexionangle willhave acorrespondingoutput
voltage.
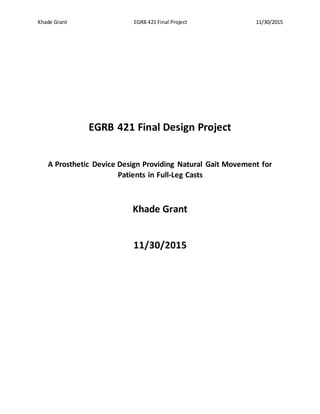
Duringthe human gaitcycle,hipflexionanglescorrespondtoknee flexionangles.Forexample,
inhealthyindividuals, when70%of the gait cycle iscomplete,the hipflexionangle isapproximately12°.
Thiscorrespondstoa knee flexionangleof 64°. The correspondinghipandknee flexionanglesare
showninFigure 5.
11. Khade Grant EGRB 421 Final Project 11/30/2015
Figure 5. Trajectories of hip and knee angles during human gait cycle (Colombo et al., 2000)
The voltage producedfroma hipflexionanglewouldcause the mechanical kneetorotate to the
correspondingknee flexionangle.
Sample Calculation:Vi = 20mV. At 0° hipflexionthe wiperisat180°. ThusR2 = Rtotal/2. Thisimplies0°hip
flexioncorrespondstoV0 = 10mV.
At 12° hipflexion,the wiperisat192°. Thus R2 =
192
360
× 𝑅total. 𝑉𝑜 =
192
360
×𝑅 𝑡𝑜𝑡𝑎𝑙
𝑅 𝑡𝑜𝑡𝑎𝑙
× 20𝑚𝑉 = 10.67𝑚𝑉.
10.67mV will thenbe calibratedtoproduce aknee flexionangle of 64°.
The mechanical knee consistsof amicrochipcircuit, ananalog to digital (A/D) converter, adigital
to analog(D/A) converter, amicroprocessor,anelectricsteppingmotor,andgears. The microchipcircuit
will transferthe electricenergyproducedbythe single-turnpotentiometertothe A/Dconverter.
Varyinghipflexionangleswillproduce voltages(andthuscurrent) atvaryingamplitudes.The varying
amountof electricenergy producedwillbe passed tothe A/Dconverter.The signal will thenbe
convertedtoa digital signal.Thissignal will thenbe passed tothe microprocessorwhichwill processthe
digital dataaccordingto the preprogrammed instructionsgiventoit.The microprocessorwillthen
outputa digital signal tothe D/A converterwhichwill produce andpassan electricsignal tothe electric
steppingmotor.The specificelectricsignal fromthe D/A converterwill cause the electricsteppingmotor
12. Khade Grant EGRB 421 Final Project 11/30/2015
to provide the mechanical energynecessaryto rotate the gearsto an absolute angle.The mechanical
legswhichare attachedto the mechanical knee will thusbe forcedtorotate to thatangle.
The electricsignal producedbya specifichipflexionangle will be convertedintoaspecificdigital
signal correspondingtothe inputtedelectricsignal.The microprocessorwill be preprogrammedto
convertthat digital signal toa newdigital signal thatwill correspondto the absolute angle rotationin
the mechanical knee.The newdigitalsignal will be convertedtoanelectricsignal (bythe D/A converter)
of the magnitude requiredto cause the electricsteppingmotorto produce a rotation of the gearsinthe
mechanical knee tothe absolute angularpositiondesired. The signal processingflowchartinthe
mechanical knee is showninfigure 6.
Figure 6. Signal Processing Flowchart of Mechanical Knee
In orderto ensure the knee flexestothe appropriate angleandtopreventover-rotation,one of
the gears will containaHigh-Resolution MagnetostrictivePositionSensor.These are positionsensors
producedbyMTS and usesthe same technologyasthe MTS testingsystemsusedinDr.Wayne’s
BiomechanicsLab.The inside of the mechanical kneewillhave these positionsensorsaswell locatedat
variousangularpositions.The positionsensoronthe gearwill remainactivated,butonlythe position
sensorsaroundthe inside of the mechanical knee atthe correctangularknee positon(correspondingto
the hipangular position) willbe activated.Whentwoactivatedpositionsensorscome incontact,the
rotationstopsat that position.
13. Khade Grant EGRB 421 Final Project 11/30/2015
The microprocessorwill allow the calibrationof the mechanical knee tobe veryrobust.A
microprocessorisa programmable device thatacceptsdigital dataas input,processesthatdata
accordingto preprogrammedinstructionsstoredinitsmemory,andoutputsdigital data.A computer
program will needtobe writteninthe future forthe microprocessortoproduce the requiredelectric
signal.The programwill have torelate the electricsignal producedbyhipflexiontoacorresponding
signal thatproducesthe requiredabsolute anglerotation. Sincea12° hipflexionangleproduces
10.67mV, and assumingan electricsignal of 15mV appliedtothe electricsteppingmotorwill cause a
rotationto the 64° position,the followingsamplecode shownin Figure 7couldbe used.
Figure 7. Sample Code for microprocessor
One potential problemisthe factthat some hipflexionanglesoccurtwice inthe gaitcycle,and
thushave two differentcorrespondingkneeflexionangles.Thisproblemissolvedbyaddingan
additional wiper(offset90°clockwise fromthe firstwiper),adifferentiator,anothermicroprocessor,
A/D andD/A converter,anda single-poledouble-throw (SPDT) switch. Sincehipflexionanglesonly
occur once whenthe hipisflexing,andthenagainwhenthe hipextends,the voltage producedfromthe
firstwipercanbe usedwhenthe hipisflexing,andthe voltage producedfromthe secondwiper
(producesdifferentvaluesbecause of the 90° offset) canbe usedwhenthe hipisextending.While the
hipis flexing,the outputvoltagewouldbe increasing.Thusthe differentiator( 𝑖 = 𝐶 ×
𝑑𝑣
𝑑𝑡
) would
produce a positive current.Whenthe microprocessorreceivesapositivecurrentsignal itwill cause the
switchto connectto the firstwiper.However,whenthe hipisextending,andanegative currentis
producedfromthe differentiator,the microprocessorwill cause the switchtoconnecttothe second
wiper. The signal processingflowchartforthe entire device isshownbelow infigure 8:
14. Khade Grant EGRB 421 Final Project 11/30/2015
Figure 8. Signal Processing Flowchart for Entire Device
Testing/EvaluationMethods
The device will undergotwomajor testingmethods:strengthtestingand motiontesting;aswell aspost-
productionevaluation.
StrengthTesting:The methodsrequiredfortestingpylonstrengthbefore use are compressive loading
and bendingtests. These testswillconsistof applying normal andcycliccompressiveloads,aswell as
bendingloadstothe device until failure todeterminethe maximumloadsthe device canbear.
Furthermore,beforethe designcanbe usedinthe market,itmustfirstundergotrialsbyhealthyhuman
subjects.These testswillconsistof performingwalkingmovementsatvariousspeeds;namely,walking
at 60% normal walkingspeed,walkingatnormal walkingspeed(5.0km/hor3.1 mph),anda brisk
16. Khade Grant EGRB 421 Final Project 11/30/2015
recoveringfromtibial fractureswithahands-freedevice thatallowsforanatural walkingmotionby
providingknee flexion.The designsolutionconsistsof amechanical prostheticlegapparatus which
providesknee flexionthroughamechanical knee.The device consistsof angularsensorsand
microprocessorsthatrelate the hipflexionangleduringeachstage of the humangait cycle to the knee
flexionangleatthe correspondingstage inthe gaitcycle.The outputsignal producedfromthe hip
flexionangleiscalibratedtoproduce the correspondingkneeflexionangle.Thishands-free device
providespeople withtibial fractureswhoare subjectedtorehabilitationinfull-legcastswiththe ability
to move naturally.
18. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix I – Calculation/Validation of Dimensions and Materials List
Supplementary Figure 1. Calculation/Validation of Dimensions and Material Parts List
19. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix I (continued)
Supplementary Figure 2. Calculation/Validation of Dimensions
20. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix II – Initial Drawings
Supplementary Figure 3. Initial Drawings. (a) Frontal View. (b) Sagittal View. (c) Sagittal View during Gait Cycle
21. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix III – Preliminary Test Results
CompressionTest Results
Name Type Min Max
Stress1 VON: von Mises Stress 0 N/m^2
Node: 50455
2.45758e+006 N/m^2
Node: 83321
iKhade-Static 1-Stress-Stress1
Supplementary Figure 4. Compression Test Results: Stress Analysis
22. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix III (continued)
Name Type Min Max
Displacement1 URES: Resultant Displacement 0 mm
Node: 50455
0.00288903 mm
Node: 80672
iKhade-Static 1-Displacement-Displacement1
Supplementary Figure 5. Compression Test Results: Deformation Analysis
23. Khade Grant EGRB 421 Final Project 11/30/2015
Appendix III (continued)
Name Type Min Max
Strain1 ESTRN: EquivalentStrain 0
Element: 29414
1.75294e-005
Element: 54094
iKhade-Static 1-Strain-Strain1
Supplementary Figure 6. Compression Test Results: Strain Analysis