
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ABNORMALITIES IN DEVELOPMENT OF FEMALE GENITALIA
Similar to ABNORMALITIES IN DEVELOPMENT OF FEMALE GENITALIA (20)
Recently uploaded
Recently uploaded (20)
ABNORMALITIES IN DEVELOPMENT OF FEMALE GENITALIA
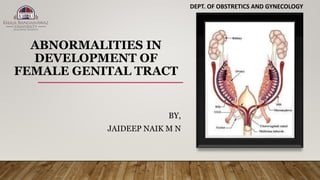
- 1. ABNORMALITIES IN DEVELOPMENT OF FEMALE GENITAL TRACT BY, JAIDEEP NAIK M N DEPT. OF OBSTRETICS AND GYNECOLOGY
- 2. Differentiation of the gonad into testes or ovary is genetically determined. Disorders of sexual differentiation and development can occur due to chromosomal abnormalities, or abnormalities in hormone production/hormone receptors. Development of the internal and external genital organs is independent of the development of the gonad, though controlled by the hormones from the gonad. Classification of developmental anomalies of genital tract • Disorders of sexual development • Developmental disorders of the vagina • Developmental disorders of the cervix and uterus
- 3. Classification of disorders of sexual development 46,XX DSD 46,XY DSD Ovo-testicular DSD
- 4. This, by definition, is female genotype, normal ovaries but with virilization of external genitalia. Exposure to endogenous androgens as in congenital adrenal hyperplasia (CAH) is the most common cause. This may be a neonatal emergency due to electrolyte disturbances. Virilization of female external genitalia in a newborn infant with congenital adrenal hyperplasia
- 5. In this condition, the genotype is male, but there is inadequate masculinization of external genitalia. This can be due to the following defects: i. Inadequate testosterone production due to enzyme defects ii. Inadequate testosterone metabolism 5a-reductase deficiency iii. Partial androgen insensitivity syndrome iv. Complete androgen insensitivity syndrome v. XY gonadal dysgenesis vi. Isolated deficiency of AMH Incomplete masculinization of male fetus. Testes are seen in the labia and the penis is underdeveloped with hypospadias- partial androgen-insensitivity syndrome.
- 6. • These children are born with testis on one side ovary on the other side or ovotestes on both sides. • Karyotyping may reveal 46,XX, 46,XY or mosaics with any combination. • Müllerian structures are generally present due to deficient AMH, and masculinization of external genitalia is not complete.
- 8. History Prenatal exposure to androgens Consanguineous marriage Clinical examination Features of Turner syndrome[45,X0] • Webbed neck • Cystic hygroma Features of hypoadrenalism • Pigmentation • Lethargy External genitalia • Microphallus • Hypospadias • Clitoromegaly • Posterior labial fusion Testes • Absent • Present in • Scrotum • Labia majora • Inguinal region Investigations • Karyotyping • Tests for congenital adrenal hyperplasia • Serum electrolytes • 17-Hydroxyprogesterone DHEA Ultrasonography • Gonads • Uterus • Vagina
- 9. Infants with CAH require immediate correction of electrolyte disturbances. Sex of rearing, genital reconstruction and psychological issues have to be decided upon in consultation with the parents. Corrective surgery, hormone therapy and gonadectomy may be required at or after puberty. The following points must be remembered: All infants with XX karyotype and CAH should be reared as girls and corrective surgery performed for clitoromegaly and labial fusion at the appropriate time. Children with complete androgen insensitivity should also be raised as females. XY chromosome will have partial development of male external genitalia and further development at puberty. These children should be raised as males.
- 10. Vaginal agenesis • Complete[failure of canalization of vagina, associated with mullerian agenesis]. • Partial[failure of canalization of the lower part of the vagina- distal to the normal uterus, cervix and upper vagina leads to this anomaly]. Imperforate hymen[Situated at the junction of sino-vaginal bulbs and urogenital sinus] Anomalies of vertical fusion • Transverse vaginal septum[Non canalization at the junction b/w the two developmental parts of vagina : Mullerian tubercle and Sino-vaginal bulbs, m/c upper 1/3rd ] Anomalies of lateral fusion • Longitudinal septum[ may be complete or partial, the uterus normally developed , or other anomalies such as septate, bicornuate uterus or uterus didelphys] • Longitudinal septum with obstructed hemi-vagina.
- 11. Evaluation of vaginal anomalies Clinical evaluation Examination of external genitalia Per rectal examination to look for hematocolpos and uterus Examination under anesthesia Investigations Ultrasonography Magnetic resonance imaging, if required Surgical management of vaginal anomalies • Imperforate hymen • Cruciate incision • Transverse vaginal septum • Excision of septum • Longitudinal septum • Excision of septum • Vaginal agenesis with hematocolpos[vaginal retention of menstrual blood at puberty] • Drainage of hematocolpos • Vaginal reconstruction • Total vaginal atresia (MRKH) • Nonsurgical • Gradual dilatation • Surgical • McIndoe vaginoplasty • Williams vulvovaginoplasty • Sigmoid vaginoplasty
- 13. These are grouped under Müllerian duct anomalies. They result from defective fusion or canalization. The defects may involve the entire length of the Müllerian ducts, but more often they are segmental. Class I anomalies include vaginal anomalies, It is important to remember that many of these anomalies produce no symptoms and go unnoticed. The most common anomaly is septate uterus. Most women with Müllerian anomalies with out- flow obstruction present with amenorrhea and abdominal pain at puberty. Total non fusion anomalies produce no symptoms; anomalies such as arcuate uterus are generally undiagnosed. Septate uterus, rudimentary horn, bicornuate uterus and uterus didelphys can give rise to problems during pregnancy.
- 14. A unicornuate uterus is a rare condition that causes a person to have only half a uterus. A bicornuate uterus is a uterine malformation that is produced due to impairment in the fusion of Mullerian ducts. Uterus didelphys is a rare condition where a person develops two uteruses. It’s also called a double uterus. A double uterus is a congenital abnormality that you are born with.
- 15. Clinical problems of Müllerian anomalies Gynecological Primary amenorrhea Outflow obstruction Dyspareunia Infertility Ectopic pregnancy Obstetric Recurrent pregnancy loss Preterm labor Malpresentations Fetal growth restriction Antepartum hemorrhage Dystocia Ruptured uterus Retained placenta Postpartum hemorrhage Management depends on the type of anomaly. In women with vaginal agenesis, vaginal reconstruction is performed. Rudimentary horn with signs of obstruction should be excised. Uterine septum can be excised hysteroscopically. Strassman metroplasty consists of wedge resection of the septum and reconstruction of the uterus and may be indicated in women with a bicornuate uterus.