cementum by dr. ishu singla.pptx
•
1 like•635 views

seminar on cementum for dental students

Recommended
More Related Content
What's hot
What's hot (20)
Similar to cementum by dr. ishu singla.pptx
Similar to cementum by dr. ishu singla.pptx (20)
Recently uploaded
Recently uploaded (20)
cementum by dr. ishu singla.pptx
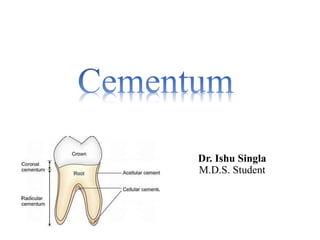
- 1. Dr. Ishu Singla M.D.S. Student
- 2. CONTENTS • INTRODUCTION • DEFINITION • PROPERTIES • BIOCHEMICAL COMPOSITION • CLASSIFICATION OF CEMENTUM • TYPES OF CEMENTUM • CELLS OF CEMENTUM • CEMENTOGENESIS • DEVELOPMENT OF CEMENTUM • CEMENTOENAMEL JUNCTION • CEMENTODENTINAL JUNCTION • FUNCTIONS • AGE CHANGES • RESORPTION & REPAIR • CLINICAL CONSIDERATIONS • CONCLUSION • REFERENCES
- 3. INTRODUCTION The Periodontium consists of the investing layer and supporting tissues of the tooth: gingiva, periodontal ligament(PDL), cementum and alveolar bone. Divided into 2 parts: • Gingiva : protects the underlying tissues • Attachment apparatus : composed of PDL, cementum and alveolar bone Cementum is considered a part of the periodontium because, with the bone it supports fibres of PDL.
- 4. • Cementum – origin from latin word “caementum” quarried stone i.e. chips of stone used in making mortar. • Least understood of all dental hard tissues. • First described in 1835 yet poorly defined at the cellular and molecular level. (Saygin et al,2000)
- 5. • Cementum was 1st demonstrated in 1835 by 2 pupils of Purkinje. • It begins at the cervical portion of tooth at cemento –enamel junction and continues to the apex.
- 6. DEFINITIONS • A thin layer of calcified tissue covering dentin of root. (Berkowitz BKB,Holland GR and Moxham ) • Cementum is the mineralized dental tissue covering the anatomic roots of human teeth. (Armitage,1977) • Cementum is the calcified, avascular mesenchymal tissue that forms the outer covering of the anatomic root. (Carranza, Newman, Takei & Klokkevold)
- 7. COMPARISON OF DENTAL HARD TISSUES ENAMEL DENTIN CEMENTUM ALVEOLAR BONE •Embryological background Enamel organ Dental papilla Dental papilla Mesoderm •Type of tissue Epithelial Connective tissue Connective tissue Connective tissue •Formative cells Ameloblasts Odontoblasts Cementoblasts Osteoblasts •Incremental lines Lines of Retzius Imbrication lines of von Ebner Arrest & reversal lines Arrest & reversal lines •Mature cells None (lost with eruption) only Dentinal tubules with processes Cementocytes Osteocytes •Resorptive cells Odontoclasts Odontoclasts Odontoclasts Osteoclasts 7
- 8. PHYSICAL PROPERTIES OF CEMENTUM (Berkowitz et al, 2002) • Pale yellow with a dull surface • Softer than dentine (Selvig and Selvig,1962) • Permeability • cellular variety more permeable as the canaliculi in some areas are contiguous with the dentinal tubuli. • decreases with age • Soft and thin cervically – readily removed by abrasion
- 9. THICKNESS OF CEMENTUM • Varies at different levels of the root • Thickest at the root apex and interradicular areas of multirooted teeth – 50-200µm (may exceed to 600µm) • Thinnest cervically – 10-15µm • Between ages 11 and 70 – thickness increases 3 fold – 95µm at 20yrs and 215µm at 60yrs. (Zander HA,Hurzeler B,1958)
- 10. • Thickest on distal side than on mesial due to mesial drift. (Rose Dastmalchi et al,1990) • Cementum is thicker in areas exposed to tensional forces. (Schroeder,1991)
- 11. BIOCHEMICAL COMPOSITION OF CEMENTUM ( Bosshardt and Selvig,1997) WEIGHT ORGANIC INORGANIC WATER 65 % VOLUME 23 % 22 % 12 % 33 % 45 %
- 12. INORGANIC COMPONENT OF CEMENTUM • Ca & P- Hydroxyapatite crystal • F- highest of all mineralised tissue • Mg- 0.5%-0.9% • S-0.1-0.3% (Bosshardt D,1997) • Cu, Zn, Na- trace amounts
- 13. COMPARISON OF DENTAL HARD TISSUES ENAMEL DENTIN CEMENTUM ALVEOLAR BONE •Mineral levels 96% 70% 65% 60% •Organic & water levels 1% & 3% respectively 20.5 & 10% respectively 23% & 12% respectively 25% & 15% respectively •Tissue formation after eruption None Possible Possible Possible •Vascularity None None None Present •Innervation None Present None Present 13
- 14. NON COLLAGENOUS COMPONENT • glycoproteins • proteoglycans • phosphoprotein (Bronckers et al,1994;MacNeil and Somerman,1993;MacNeil et al,1995;McKee et al 1996) ORGANIC COMPONENT • Type I-major(90%) (Birkedal-Hansen et al,1977) • Type III (Rao LG,Wang HM, Kalliecharan R, et al;1979) •Type XIV (Becker et al, Romanos et al,1991) •Traces of type V, type VI ,typeXII ( Nanci A.,Bosshardt D. ,2006) COLLAGEN
- 15. • Non-collagenous proteins are similar to that of bone (Bosshardt 2005) • Bone sialoprotein (typeII)and osteopontin(typeI) – both are phosphorylated and sulfated glycoproteins • Bind tightly to collagenous matrices and hydroxyapatite • Participate in mineralization process (Bronckers et al 1994;Chen et al1992;MacNeil et al;McKee et al 1996) • Acellular cementum contains much more of these than cellular cementum
- 16. Osteonectin – another glycosylated protein • Found in extracellular matrix of mineralized tissue. • Close relation between osteonectin and collagen seems to exist in mineralization process.
- 17. • Glycoproteins – fibronectin and tenascin – more widely distributed • High molecular weight and multifunctional proteins of the extracellular matrix • Fibronectin binds cells to components of extracellular matrix • During tooth development, both are present in the basement membrane of HERS at the time of odontoblast differentiation • Later, they are also found at the attachment site of PDL to cementum but not in the cementum layer itself (Lukinmaa et al 1991) •Keratin sulfate :lumican,fibroglycan (precementum) (Chenget al 1996)
- 18. • Enzyme alkaline phosphatase believed to participate in cementum mineralization (Beertsen and Everts, 1990) • Enzyme activity adjacent to cellular intrinsic fiber cementum is higher than that to acellular extrinsic fiber cementum and thickness of the latter correlates positively with the enzyme activity (Groeneveld et al, 1995) • Cementum derived growth factor- Insulin like growth factor(IGF)- like molecule that enhances proliferation of gingival fibroblasts and PDL(Cho and garant 1988’1996) • Cementum attachment protein (CAP) • Enamel derived protein-amelogenin,ameloblastin,enamelin • Glycosoaminoglycans-halyuronan, dermatin and chondroitin sulfate(Bartold et al 1998)
- 19. CLASSIFICATION OF CEMENTUM According to Gottleib (1942): 19 ACELLULAR CEMENTUM (Primary /prefunctional/coronal) CELLULAR CEMENTUM (Secondary /functional/radicular) A B
- 20. • These lines contain higher content of ground substance and mineral and lower content of collagen. • As acellular cementum is formed slowly, the incremental lines are closer together than that of cellular cementum which is deposited more rapidly. • Known as “INCREMENTAL LINES OF SALTER”
- 21. ACELLULAR CEMENTUM CELLULAR CEMENTUM First layer of cementum deposited •Formed after acellular layer No cells •Lacunae & canaliculi containing Cementocytes & their processes Sharpey’s fibers make up the bulk; are completely calcified •Sharpey’s fibers occupy a smaller portion; are partially or completely calcified At least 1 layer over all of the root, with many layers near cervical 1/3rd •Layered over acellular mainly in apical 1/3rd , especially interradicular region. Formed at a slower rate •Formed at a faster rate Precementum layer virtually absent •Precementum layer present Border with dentin not clearly demarcated •Clearly demarcated Incremental lines relatively close together •Relatively wide apart 21
- 22. Cellular cementum(B) overlying acellular(A), vice a versa or alternate
- 23. • The Sharpey's fibers constitute the extrinsicfiber system (E) of the cementum and are produced by fibroblasts in the periodontal ligament. • The intrinsic fiber system (I) is produced by cementoblasts and is composed of fibers oriented more or less parallel to the root. E I I
- 24. TYPES OF CEMENTUM According to Schroeder (1986, 1991) 24 ACELLULAR AFIBRILLAR CEMENTUM ACELLULAR EXTINSIC FIBER CEMENTUM CELLULAR MIXED STRATIFIED CEMENTUM CELLULAR INTRINSIC FIBER CEMENTUM
- 25. 1.Acellular afibrillar cementum 2.Acellular extrinsic fiber cementum 3.Cellular intrinsic fiber cementum 4.Cellular stratified mixed cementum
- 26. CEMENTUM TYPE PRODUCED BY ORIGIN OF FIBRES LOCATION FUNCTION •Acellular afibrillar (1- 15 μm) Cementoblasts - Spurs & patches over enamel & dentin along the CEJ No known function •Acellular extrinsic fibre (30- 230 μm) Fibroblasts & cementoblasts Extrinsic fibres From cervical margin to apical third Anchorage •Cellular mixed stratified (100- 1000 μm) Fibroblasts & cementoblasts Intrinsic & extrinsic fibres Apical portion & furcations Adaptation •Cellular intrinsic fibre cementum Cementoblasts Intrinsic fibres Middle to apical third & furcation & also fills resorption lacunae Adaptation & Repair
- 27. CELLS OF CEMENTUM • CEMENTOBLASTS • CEMENTOCYTES • CEMENTOCLASTS
- 28. Origin.- 1) Dental follicle cells 2) Hertwig Epithelial Root sheath Cell organelles- numerous mitochondria, a well-formed Golgi-apparatus and large amounts of granular endoplasmic reticulum Function- protein polysaccharids secretion CEMENTOBLASTS
- 29. •E- 11 antibody strongly reacts with CIFC forming cementoblast but not with cementoblasts AEFC, showing that the cementoblast forming cellular cementum and acellular cementum are different. •DENTAL FOLLICLE-CIFC •HERS-AEFC
- 30. CEMENTOCYTES • Cementocytes are found in cellular cementum. They are similar to osteocytes. • They are located within lacunae and have numerous cytoplasmic processes coursing in canaliculi that are preferentially directed towards the ligament.
- 31. • Their cytoplasmic volume and the density of organelles is markedly reduced when compared to cementoblasts. (The endoplasmic reticulum appear dilated and mitochondria are sparse) • While these cells remain vital, their metabolic activity is low.
- 32. CEMENTOCLASTS • Cementum resorbing cells. • Resembles osteoclast. • Found in normal functioning PDL • Resorption of cementum can occur under certain circumstances. • In these instances mononuclear cementoclasts or multinucleated giant cells, located in Howship’s lacunae, are found on the surface of the cementum.
- 33. After completion of crown formation , the cells from the inner and outer enamel epithelium(OEE) form the bilayer of cells known as Hertwig’s epithelial root sheath(HERS) The cells of inner enamel epithelium induce adjacent Cells in the Dental papilla to differentiate into odontoblasts and subsequently deposit the root dentin The HERS consists of IEE & OEE disintegrates & Following the fragmentation of Hertwig’s epithelial root sheath , cells from the dental follicle attach and align onto the matrix coating the dentin surface , and these subsequently differentiate into cementoblast and form the root cementum CEMENTOGENESIS
- 34. The fragmented epithelial cells of the Hertwigs,s epithelial root sheath never completely disappear and persist in small clusters known as epithelial cell rests of malassez. Cementum may be deposited on the root surface either during tooth development, or subsequent to eruption of the tooth during normal function.
- 35. CEMENTOGENESIS 1-differentiation of odontoblast 2-fragmentation of HERS and formation ERM 3- differentiation of cementoblast
- 36. • Prefunctional stage : root development (3.5 - 7.5 year) • Functional stage : occlusal level associated with attachment of root to bone continues throughout life - adaptive and reparative processes are carried out by the biological responsiveness of cementum influences the alterations in the distribution and appearance of the cementum varieties on the root surface with time STAGES OF CEMENTOGENESIS (Bosshardt and Selvig,1997)
- 37. There are several fundamental issues that need to be resolved to devise targeted therapeutic approaches for the prevention and treatment of periodontal diseases. These include determining the following: Precursors of cementoblasts Whether cementoblasts are a distinct cell population that expresses unique gene products Whether acellular & cellular cementum are distinct tissues Factors that promote cementoblast differentiation What regulates the formation & maintainence of PDL v/s Cementum, thus preventing fusion of root to the alveolar bone (Ankylosis)
- 38. ENAMEL ORGAN Epithelial Root SheathCells Specific Factors Mesenchymal Cells Apoptosis Follicle Cell Differentiation Cementoblasts Cementoblasts Induction of Mesenchymal cells Cementoblasts PRECURSORS OF CEMNTOBLAST
- 39. • These cells play indirect role by producing necessary signalling molecules for cell recruitment & differentiation. Whether cementoblasts are a distinct cell population that expresses unique gene products • Bosshardt (2005) proposed a new theory that cells derived form HERS play an essential role in tissue development & maintenance & that periodontal regeneration is possible. •Bosshardt (2005) supports the concept that cementoblasts producing both acellular extrinsic fibre cementum and cellular intrinsic fibre cementum are unique phenotypes that differ from osteoblasts
- 40. • A possibility has been raised that acellular extrinsic fibre cementum is formed by HERS derived cells, whereas, cellular intrinsic fibre cementum is formed by cells that derive from dental follicle. (Zeichner etal. 2003) . Whether acellular & cellular cementum are distinct tissues
- 41. ACELLULAR CELLULAR Identifiable for only a short time Identifiable for longer period Fibroblast-like morphology Osteoblast-like morphology Derived from epithelial root sheath Derived from mesenchyme Express cytokeratin Do not express cytokeratin Do not express osteocalcin Express osteocalcin Do not express receptors for parathormone,TGF and IGF Express receptors for parathormone,TGF and IGF Phenotypical differences between cementoblasts associated with acellular and cellular cementum
- 42. Morphogenes & Growth factors Suggested Functions related to CEMENTOGENESIS Growth factors •Transforming growth factor (including Bone morphogenic proteins) Promotes cell differentiation & subsequently cementogenesis during development & regeneration. •Platelet derived growth factor & insulin like growth factor Promotes cementum formation by altering cell cycle activities. •Fibroblast growth factor Promotes cell proliferation & migration & also vasculogenesis – all key events for formation & regeneration of periodontal tissues. Adhesion molecules •Bone Sialoprotein & Osteopontin Promotes adhesion of selected cells to the newly formed root. Bone sialoprotein may be involved in promoting mineralization, whereas Osteopontin may regulate the extent of crystal growth
- 43. Morphogenes & Growth factors Suggested Functions related to CEMENTOGENESIS Epithelial / Enamel like factors Epithelial – mesenchymal interactions may be involved in promoting follicle cells along cementoblast pathway. Some epithelial molecules may promote periodontal repair directly or indirectly. Collagens Type I & III collagens play key roles in regulating periodontal tissues during development & regeneration. In addition, type XII may assist in maintaining PDL space v/s continuous formation of cementum. Gla proteins •Matrix Gla protein & Bone Gla protein (Osteocalcin) These proteins contain γ-caboxyglutamic acid, hence the name Gla proteins. Osteocalcin is a marker for cells associated with mineralisation & is also considered to be a regulator for crystal growth. Matrix Gla protein prevents abnormal ectopic calcification. Key Proteins Prosposed to Regulate Cementogenesis
- 44. What regulates the formation & maintainence of PDL v/s Cementum, thus preventing fusion of root to the alveolar bone (Ankylosis) type XII along with typeI may assist in formation of cementum and maintaining of PDL space thereby preventing ankylosis . (Karimbux1995, MacNeil et al,1998)
- 45. • During root development in human teeth, the first cells that align along the newly formed, but not yet mineralized mantle dentin surface, exhibit Fibroblast characteristics. • These cells deposit collagen within the unmineralized dentin matrix so that fibrils from both the matrices interdigitate. • Mineralization of the mantle dentin starts internally and does not reach surface until blending of collagen fibrils from both the layers has occurred. It then spreads across into cementum matrix, thereby establishing dentin-cementum junction. DEVELOPMENT OF ACELLULAR CEMENTUM
- 46. • The cells on the root surface continue to deposit collagen so that fiber fringe lengthens and thickens. At the same time, they also secrete non- collagenous matrix proteins that fill in spaces between collagen fibres and regulate mineralization of the forming cementum layer. • This activity continue until about 15- 20 μm of cementum has been formed, the intrinsic fibre fringe becomes connected to the developing PDL fibre bundles. • Initial acellular cementum thus consists of a thin mineralized layer with a short fringe of collagen fibres implanted perpendicular to the root surface.
- 47. A-Acellular cementum B-Hyaline layer of Hopewell-Smith C-granular layer of Tomes D-radicular dentin • Thereafter, acellular cementum formative cells will be essentially engaged in synthesis of non- collagenous matrix proteins; collagen fibres that embed in it will be formed by PDL fibroblasts. .
- 48. • AEFC – principal tissue of attachment • Formation commences shortly after crown formation is completed and always before CIFC starts to form on more apical root portions. • The cementoblasts begin differentiation in closest proximity to the advancing root edge i.e. 20- 30um coronal to the first deposited dentinal matrix ACELLULAR EXTRINSIC FIBER CEMENTUM
- 49. These cells resemble fibroblasts, and commence to produce and attach the collagenous cementum matrix as close as 50 um coronal to the root edge Further collagen deposition results in a complete covering of the not yet mineralized dentinal matrix along the next 100 um of the root surface About 200 to 300 um coronal to the advancing root edge, the initial AEFC matrix is established on the dentinal matrix
- 50. AEFC matrix consists of a dense fringe of short collagenous fibers implanted into the dentinal matrix and oriented perpendicular to the root surface The outwardly progressing mineralization front in dentin does not reach the future CDJ until the collagenous interdigitation of the two fibril populations is established Mineralization of the mantle dentin seems apparently delayed With the onset of cementum mineralization, AEFC begins to grow in thickness slowly and constantly
- 51. • After atleast half of the root has been formed, cementoblast start forming a less mineralized variety of cementum that is distinctive in that its constituent collagen fibrils are produced by the cementoblasts themselves. • In all cases, first collagen is deposited onto the unmineralized dentin surface such that fibrils from the layers intermingle. • Like acellular cementum, cellular cementum forming cementoblasts also manufacture a no. of non- collagenous matrix proteins that fill in spaces between the collagen fibrils, regulate mineral deposition & impart cohesion to the mineralised layer. . DEVELOPMENT OF CELLULAR CEMENTUM
- 52. • A layer of unmineralised matrix called Cementoid is established at the surface of the mineralised cementum matrix. • As the process proceeds, some cementoblasts become trapped in the matrix they form. These are called Cementocytes .
- 53. • Initially deposited on root surface areas where no AEFC has been laid down on the dentin thus confined to apical and inter-radicular regions of tooth • Also found in resorption lacunae • Layer of cementoid present • cementoblasts deposit on organic matrix which becomes mineralised CELLULAR INTRINSIC FIBER CEMENTUM
- 54. • Following loss of continuity of the HERS, large basophilic cells are seen to differentiate from adjacent cells of the dental follicle against the surface of the root dentine – form a distinct layer of cementoblasts • These cementoblasts possess more cytoplasm and cytoplasmic processes than the cells associated with acellular cementum
- 55. • These fibers are oriented parallel to root surface • Due to increased rate of formation, thin unmineralized precementum layer (about 5 µm thick) will be present on the surface of cellular cementum • Precementum is less mineralized than primary cementum • Basophilia is due to roughened endoplasmic reticulum – their presence suggests that cementoblasts secrete the collagen (together with ground substance) that forms the intrinsic fibers of secondary, cellular cementum
- 56. CIFC less mineralised than AEFC due to following reasons: - heterogenous collagen organisation - rapid speed of formation - presence of cells and lacunae
- 57. • Not previously classified • Collagenous matrix of first formed cementum result of cementoblast activity and elaborated before PDL forms. • After first 15-20um of intrinsic fibre cementum has formed the fibrous fringe becomes connected to PDL fibre bundles. ACELLULAR INTRINSIC FIBER CEMENTUM
- 58. • Forms bulk of secondary cementum • When organisation of PDL takes place further deposition of cellular cementum incorporates PDL fiber bundles creating CMSC • Includes cementocytes within lacunae with canaliculi towards PDL, its laminated structure and cementoid • Cementocyte incorporation haphazard with cells widely dispersed. CELLULAR MIXED STRATIFIED CEMENTUM
- 59. CELLULAR MIXED STRATIFIED CEMENTUM
- 60. • Intrinsic fibres uniformly mineralised whereas extrinsic fibres variably mineralised with many having central unmineralised core • Layered arrangement of apical cementum with alternate layers of AEFC and CIFC CMSC CIFC AEFC (intrinsic part) (extrinsic part)
- 61. • The areas and location vary from tooth to tooth and along the CEJ of the same tooth. • No role in tooth attachment • Only mineralised ground substance present with absence of cells and collagen fibrils ACELLULAR AFBRILLAR CEMENTUM • Considered to be developmental anomaly due to local disruption of REE that permits follicular cells to come in contact with enamel surface
- 62. CELLULAR AFIBRILLAR CEMENTUM • Silness et al. (1976) observed mineralized tissue in the fissures of unerupted human third molars. The tissue had morphological features characteristic of afibrillar coronal cementum. • In addition, lacunae with canaliculi were contained in the tissue. • They suggested that the tissue is a cellular, afibrillar variety of coronal cementum produced by connective tissue cells which have transformed into cementoblasts after the disappearance of the reduced enamel epithelium from the fissures of the unerupted teeth.
- 63. • Hyaline Layer Of Hopewell Smith • Described by Hopewell Smith in 1903. • Also called as inner most cementum layer/ Superficial layer of root dentin / intermediate layer. • An ill-defined zone near the CDJ, predominantly in the apical 2/3rds of roots of molars & premolars INTERMEDIATE CEMENTUM
- 64. • It appears to contain cellular remnants of Hertwig’s sheath embedded in calcified ground substance. (EI Mostehy MR, Stallard RE,1969). • The collagen within the AEFC layer intermingles with the dentin matrix, there is no sialoprotein and osteopontin, and no obvious zone between dentin and cementum Functions Of Intermediate Cementum – • As a Permeability Barrier. • It Is a Precursor For Cementogenesis In Wound Healing
- 65. CEMENTOENAMEL JUNCTION(CEJ) OVERLAP-60% (Noyes FB,Schour I,Noyes HJ,1938)
- 66. END-TO-END-30%
- 67. GAP-10%
- 68. Teeth Edge to edge (%) Cementum overlap (%) Dentin exposure (%) Incisors/ Canines 58 17 25 Premolars 65 31 04 Molars 46 42 12 DISTRIBUTION OF CEJ Muller & Van Wyk (1984) showed the distribution of 3 types of CEJ:
- 69. • According to Schroeder HE & Scherle WF (1988): • In third molars, cementum overlap occurs in about 50% of the CEJ, the rest showing either edge-to-edge contact or exposed dentine. • Dentine exposure occurs more frequently on buccal but also on distal surfaces, at least in maxillary and mandibular (exclusively on buccal surfaces) molars. • The type of cementum which usually overlaps the enamel has been shown to be the Acellular, afibrillar variety (Schroeder 1986).
- 70. ENAMELOCEMENTAL JUNCTION • Neuvald L & Consolaro A (2000) observed a 4th type of CEJ i.e. cementum overlapped by enamel, on buccal & lingual side of specimens in 1.8 % of the specimens • Enamel overlapping cementum E-enamel C- cementum
- 71. • The terminal apical area of the cementum where it joins the internal root canal dentin is known as the cementodentinal junction. • The CDJ consists large quantities of collagen associated with glycosaminoglycans like chondrointin sulfate and dermatan sulfate resulting in increased water content and contributes to the stiffness. • This reduction in its mechanical property, helps it to redistribute occlusal loads to the alveolar bone. CEMENTODENTINAL JUNCTION(CDJ)
- 72. • In permanent teeth CDJ is smooth • Sometimes presence of intermediate cementum layer mainly seen in apical 2/3 of roots of molars and premolars • Rarely seen in incisors or deciduous teeth • Neither resembles cementum nor dentin
- 73. • Cemental fibres intermingle with the dentinal fibers at the CDJ more in cellular cementum than in acellular cementum. • This aids in attachment of cementum to the dentin, the presence of proteoglycans is the major factor for this attachment.
- 74. 1.Anchorage The primary function of cementum is to furnish a medium for the attachment of collegen fibers that bind the tooth to alveolar bone. FUNCTIONS OF CEMENTUM 2. Adaptation Deposition of cementum in an apical area can compensate for loss of tooth substance from occlusal wear. 3. Relief from Hypersensitivity Cementum covers the dentinal surface of root portion of tooth. 4. Repair Damage to roots such as fractures and resorptions can be repaired by the deposition of new cementum.
- 75. • A linear relationship between the thickness of cementum and age is seen apically > cervically. Thick - root grooves and furcation • Continual reapposition of new layer ageing of tooth as an organ maintains the attachment complex intact. • Cellular cementum exhibits degeneration & death of cementocytes. Empty lacunae are eventually observed • Permeability of cementum diminishes with age AGE CHANGES IN CEMENTUM
- 76. • Physiological root resorption : normal phenomenon of deciduous teeth during tooth shedding • Causes for resorption in permanent teeth- local like trauma from occlusion, orthodontic movement, periapical and periodontal diseases • systemic diseases like calcium deficiency, hypothyroidism, hereditary fibrous osteodystrophy and Paget’s disease or tumors • Idiopathic • Root resorption : A) Internal B) External RESORPTION OF CEMENTUM
- 77. • According to degree of persistence A)Transient B)Progressive • Root surface more resistant to resorption than bone • No. of teeth resorbed and severity of resorption are markedly increased by orthodontic treatment
- 78. • Appears microscopically as bay like concavities in the root surface • Multinucleated giant cells and large mononuclear macrophages are generally found adjacent to cementum • May extend into underlying dentin • Not necessarily continuous, may alternate with periods of repair and deposition of new cementum, new cementum is demarcated from the root by a deeply staining irregular line - reversal line
- 79. • Following detachment of odontoclasts from the root surface, cementogenic cells repopulate the Howship’s lacunae and attach the initial repair matrix to a thin decalcified layer of residual and exposed collagen fibrils • Basophilic and electron dense reversal line forms at the fibrillar junction • Deposited repair matrix resembles cellular intrinsic fiber cementum • Cementum repair requires viable connective tissue • Can occur in devitalized and in vital teeth REPAIR OF CEMENTUM
- 80. Repair of cementum , Reversal Lines in cementum with embedded cementocytes (white arrows) & cementoblast on surface of cementum (dark arrows), PDL (P) , alveolar bone (B)
- 81. TYPES OF REPAIR • ANATOMIC REPAIR -re-establish the former outline of root • FUNCTIONAL REPAIR if a thin layer of cementum is deposited on surface of deep resorption,the root outline is not reconstructed and a bay like recess remains . • In such areas the periodontal space is restored to its normal width by formation of a bony projection, so that a proper functional relationship will result, the outline of alveolar bone follows that of the root surface.
- 82. CLINICAL CONSIDERATIONS • HYPERTROPHY • HYERPLASIA • CEMENTICLES • CONCRESENCE • ENAMEL PEARL • CERVICAL ENAMEL PROJECTIONS • SYSTEMIC DISEASES AND ITS INFLUENCE ON CEMENTUM • GROWTH FACTOR AND CEMENTOGENESIS
- 83. • Hypercementosis refers to increase in growth of Cementum as a result of increased functional demand. • Hence Hypercementosis can be categorized as Cemental hypertrophy. • It is an age-related phenomenon, and it may localized to one tooth or affect the entire dentition. HYPERCEMENTOSIS
- 84. • Etiology of hypercementosis varies and is not completely understood. • In teeth without antagonist, hypercementosis is interpreted as an effort to keep pace with excessive tooth eruption. • In teeth subject to low grade periapical irritation arising from pulp disease, it is considered as a compensation for the destroyed fibrous attachment of the tooth. The cemnetum is deposited adjacent to the inflamed periapical tissue.
- 85. Diseases where hypercementosis can be seen as generalized with nodular enlargement of the apical third of the root - - Pagets disease, (Rushton MA,1938). -Other systemic disturbances that may be asssociated are acromegaly, arthritis, calcinosis, rheumatic fever and thyroid goiter. -(Leider AS, Garbarino VE, 1987).
- 86. • If the overgrowth improves functional qualities of the cementum, it is termed as cementum hypertrophy • If the overgrowth occurs in non-functional teeth or if it is not correlated with increased function, its termed hyperplasia. • Extensive hyperplasia of cementum is occasionally associated with chronic periapical inflammation • Hyperplasia of cementum in non-functioning teeth is characterised by a reduction in the number of Sharpey’s fibers embedded in root • Spur or prong like extension of cementum is found in teeth that are exposed to great stress. • Knob like projections are designated as excementosis HYPERPLASIA OF CEMENTUM
- 87. CEMENTICLES • Calcified ovoid or round nodule found in the PDL. • Single or multiple near the cemental surface. • Free in ligament; attached or embedded in cementum. • Aging and at sites of trauma. • Origin: Remnants of Herwig’s epithelial cell i.e. epithelial cell rests of Malassez, in the periodontal ligament. • These bodies arise by deposition of calcium salts in the adjacent surrounding connective tissue
- 88. • Fusion which occurs after root formation. • Teeth are united by cementum only. • Believed to arise as a result of traumatic injury or crowding of teeth resulting into resorption of interdental bone, so that two roots are in approximate contact and become fused by deposition of cementum. CONCRESENCE
- 89. Enamel Pearl / Enamel Drop/ Enamel Nodule/ Enameloma • Hemispheric structures consisting entirely of enamel or may contain. dentin and pulp tissue within. • Project from surface of root, more in maxillary molars. Common in CEJ and furcation area • Believed to arise from localized bulging of odontoblastic layer – bulge may provide prolonged contact between HERS and developing dentin, triggering induction of enamel formation.
- 90. CERVICAL ENAMEL PROJECTIONS (CEP) • Occur along surface of dental roots • Represent dipping of enamel from CEJ toward the bifurcation of molar teeth. • It forms triangular extension of coronal enamel that develops on buccal surface of root overlying bifurcation. • More in mandibular molars & maxillary second molars. CEP CEP
- 91. SYSTEMIC DISEASES AND ITS INFLUENCE ON CEMENTUM (Shafer et al, 2006) • CLEIDOCRANIAL DYSPLASIA-absensce of cellular cementum on erupted teeth in both dentition with no increased thickening of primary acellular cementum. • HYPOPHOSPHATASIA- absence of alkaline phosphatase enzyme, charecterized by absence of cementum, premature exfoliation(incisors)
- 92. • HYPERPITUTARISM- hypercementosis due to structural and Functional demands ,supraeruption of posterior teeth • HYPOTHYROIDISM- teeth my fail to erupt if developed during childhood, in adults external resorption of roots may occur • PAGET’S DISEASE-Loss of lamina dura and root resorption. Generalized hypercementosis sometimes • HYPERPARATHYROIDISM- loss of lamina dura around teeth and root resorption.
- 93. GROWTH FACTORS AND CEMENTOGENESIS • growth factors common to both cementum and bone include members of the TGF-beta superfamily, such as the BMPs, as well as IGF-I and IGF-II, platelet-derived growth factors (PDGFs), epidermal growth factor (EGF), and the fibroblast growth factors (FGFs). In addition, cementum-derived growth factor (CGF), an isoform of IGF-I, appears to be cementum-specific • Emdogain™ (Strauman AG, Basel, Switzerland), a mixture of enamel matrix proteins, primarily amelogenins, isolated from developing porcine teeth, has been approved by the U.S. Food and Drug Administration (FDA) for regeneration of angular intrabony periodontal defects
- 94. •Cementum by virtue of its structural and dynamic qualities, provides tooth attachment and maintenance of occlusal relationship. These multiple functions are fulfilled by the biological activity and reactivity of cementoblast, which deposit two collagen – containing varieties of cementum with completely different properties. •The discovery of variety of non collagenous proteins in cementum has opened a new research area of great therapeutic potential by virtue of periodontal regenerative tissue. CONCLUSION
- 95. •Bartold and Narayan.Biology of the periodontal connective tissue ,1988 •Berkowitz BKB ,Holland GR and Moxham BJ.Oral Anatomy embryology & histology-3rd ed,2002 •Orban cited in Bhaskar’s SN.Oral histology and embroyology -11th ed,199 •Nanci A.Ten Cate’s Oral Histology -6th ed,2003 •Lindhe J.Clinical periodontology and Implant Dentistry- 4th ed 2003 •Carranza & Newman.Clinical Periodontology-8th,10th ed REFERENCES
- 96. • Nazan E.Saygin,William V.Giannobile & Martha J.Somerman:Molecular & cell biology of Cementum, Periodontology 2000,Vol 24:73-98,2000 • Bosshardt D.,Selvig K. Dental cementum: the dynamic tissue covering of the root,Periodontology 2000, Vol 13:41- 75,1997 • Nanci A.,Bosshardt D: Structure of periodontal tissues in health and disease ,Periodontology 2000,Vol 40;11- 28, 2006: • Shafer,Hine and Levy.Shafers textbook of oral pathology 5th ed,1993 & 2006