2. Bilirubin
Bilirubin is the yellow breakdown
product of normal Heme
catabolism taking place
Reticuloendothelial system in liver
and spleen
3. Degradation (Breakdown) of Hemoglobin is
Part of Normal Catabolism in Human Body
HemoglobinGlobin
Heme
Iron
Biliverdin
Bilirubin
Amino acid Pool
ExcretionRecycle
4. Degradation of Hb in RE cells leads to
formation of Bilirubin
Bilirubin released in blood
and bound to Albumin
Bilirubin taken by liver
(Dissociates from Albumin)
Bilirubin is conjugated
and excreted in bile and then intestine
In intestine, Bilirubin is
converted to Urobilinogen
5. Types of Bilirubin
• Unconjugated bilirubin:
– Insoluble in water.
– Indirect bilirubin travels through the bloodstream
to the liver, where it is changed into a soluble
form (direct or conjugated).
• Conjugated bilirubin:
– Soluble in water and is made by the liver from
indirect bilirubin.
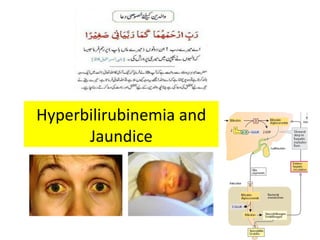
7. Hyperbilirubinemia Causes Jaundice
• Hyperbilirubinemia is said when bilirubin in
the blood exceeds 1 mg/dL.
• Bilirubin accumulates in the blood, and when
it reaches a certain concentration
(approximately 2–2.5 mg/dL), it diffuses into
the tissues, which then become yellow. That
condition is called jaundice or icterus.
8. Jaundice is a yellowish pigmentation
of the skin and conjunctiva caused by
hyperbilirubinemia
• Jaundice, (also known as icterus)
is a yellowish pigmentation of
the skin, conjunctiva and other
mucous membranes caused by
hyperbilirubinemia
9. In clinical studies of jaundice,
measurement of bile pigments
is of great value
• Total bilirubin in serum.
• Conjugated bilirubin in serum.
• Unconjugated bilirubin in serum.
• Urobilinogen in urine.
• Stercobilinogen in feaces.
10. Bile Pigments in blood
Under Normal Conditions
• Total bilirubin:
–5.1–17.0μmol/L (0.3–1.0,mg/dL)
• Conjugated" or "Direct bilirubin
–1.0–5.1μmol/L (0.1–0.3mg/dl)
• Unconjugated" or "Indirect bilirubin
–4-12 μmol/L (0.2-.7mg/dL)
11. Conjugated Vs Un-Conjugated Bilirubin
• Van den Bergh reaction:
–The measurement of bilirubin depends on
its reaction with diazosulfanilic acid to
create azobilirubin.
• Conjugated Bilirubin:
–Water soluble reacts quickly with reagent.
• Un-conjugated Bilirubin:
–Insoluble in water Reacts less quickly with
reagent.
12. URINARY EXCRETION OF BILIRUBIN
• Under normal circumstances, a little amount of
urobilinogen is excreted via the kidneys.
• If the liver's function is impaired or when biliary
drainage is blocked, some of the conjugated
bilirubin leaks out of the hepatocytes and appears
in the urine, turning it dark amber.
• In conditions where unconjugated bilirubin is
raised, urobilinogen will not appear In urine.
14. Serum Bilirubin as diagnostic parameter
• Elevated levels may indicate certain diseases.
–Jaundice >2 mg/dl
• Hemolytic
–Both, depending upon hemolysis
–Mostly Uncojugated
• Hepatic
–Both, depending upon tissue damage
• Post hepatic or obstructive
–Mostly Conjugated
15. Prehepatic (hemolytic) jaundice
• Excess hemolysis:
–High serum concentrations of
unconjugated bilirubin
• Causes:
•Autoimmune disease.
•Hemolytic disease of the newborn
(Rh - or ABO- incompatibility)
•Mismatch Blood Transfusion.
•Abnormal RBCs (Sickle cell disease)
•G6PD deficiency
16. Hemolytic Jaundice Symptoms
• Yellow or discoloration of skin and mucous
membrane
• Normal /Dark colored stools
• Dark yellow or brown colored urine
• Increased bilirubin level
• Anemia
• Weakness
17. Intrahepatic (Hepato-Cellular) jaundice
• Failure in the function of hepatocytes to take up,
conjugation or excrete bilirubin.
• Causes:
–Hepatitis (commonly viral or alcohol related)
–Cirrohsis
–Drugs or other toxins (Acetaminophen, alcohol,
estrogens, etc)
–Genetic:
• Gilberts syndrome
• Crigler-Najjar Syndrome
–Hepatic cancer
18. Symptoms of Hepatic Jaundice
• Yellow discoloration of eye ,skin and mucous
membrane.
• Light colored stools & dark yellow or brown
colored urine.
• Nausea and vomiting.
• Loss of Appetite
• Abdominal pain.
• Fever.
• Weakness.
19. Gilbert’s Syndrome
• Mild Genetic liver disorder.
• Deficiency of enzyme glucuronyl transferase.
• Decreased ability of the liver to conjugate
bilirubin.
• Characterized by mild, increases in
unconjugated bilirubin.
20. Crigler-Najjar Syndrome
• Severe Genetic disorder
• Deficiency of enzyme glucuronyl transferase.
• Complete absence or marked decrease in
bilirubin conjugation.
• Severe unconjugated hyperbilirubinemia that
usually presents at birth
• Type 1 is more severe and fatal.
21. Obstructive (Post hepatic) jaundice
is Caused by an obstruction
of the biliary tree
–Gall Stones
–Hepatitis
–Pancreatic cancer
–Liver Cancer
–Cystic Fibrosis
–Genetic (Dubin-Johnson and Rotor’s
Syndromes).
22. Obstructive (Post hepatic) jaundice
is Characterized by
• Serum bilirubin is conjugated, and other
biliary metabolites, such as bile acids
accumulate in the plasma.
• Clay white colored stools (absence of fecal
bilirubin or urobilin)
• Dark urine (increased conjugated bilirubin)
• In a complete obstruction, urobilin is absent
from the urine.
23. Obstructive jaundice Symptoms
• Yellow discoloration of eye, skin and mucus
membrane.
• Dark yellow or brown colored urine and Clay
white stools.
• Enlarged liver / spleen.
• Itching
• Nausea
• Fever
• Weight loss
• Diarrhea Upper abdominal pain
24. Dubin-Johnson and Rotor’s Syndromes
• Genetic
• Characterized by impaired biliary secretion of
conjugated bilirubin.
• The hyperbilirubinemia is caused by mutation
in the gene encoding, the protein involved in
the secretion of congugated bilirubin into the
bile.
25. NEONATAL PHYSIOLOGIC JAUNDICE
• Lack of the intestinal bacteria that facilitate
the breakdown and excretion of conjugated
bilirubin in the feces (this is largely why the
feces of a neonate are paler than those of an
adult).
–Instead the conjugated bilirubin is
converted back into the unconjugated
form by the enzyme β-glucuronidase
and a large proportion is reabsorbed
through the enterohepatic circulation.
• Premature Enzyme system
26. Toxicity of Bilirubinin a new-born
(Kernicterus)
• Hyperbilirubinaemia in a new-born can lead to
accumulation of bilirubin in certain brain
regions.
– Consequent irreversible damage to brain
manifesting as various neurological deficits.
• Seizures, abnormal reflexes and eye
movements.
• The neurotoxicity of neonatal
hyperbilirubinemia is because of the
incompletely developed blood–brain
barrier.
28. Differentiate between
Pre-hepatic, Hepatic & Post-hepatic jaundice
Test Pre Hep Post
Urobilinogen (Urine) ↑ ↓ Neg
Urine Color N Dark Dark
Stool Color N Light Clay
Urine Bilirubin (Conj) - + +
30. Bilirubin Lab Values
• Normal 0.1 – 1mg/dl
• Hyperbilirubinemia 1 – 2 mg/dl
• Jaundice >2 mg/dl
– Hemolytic
• Both, depending upon hemolysis
• Mostly Uncojugated
– Hepatic
• Conjugated
• Both, depending upon tissue damage
– Post hepatic or obstructive
• Mostly cojugated
Editor's Notes
Heme catalyzed by heme oxygenase green pigment biliverdine is formed biliverdine is further reduced by reductase and forms bilirubin.
After 120 days rbc are taken up and degraded by RE system in spleen and liver
In the intestine glucoronic acid is removed by bacteria n urobilinogen is formed some of it reabsorbed in the gut and enter into the portal circulation a portion of it participate in enterohepatic urobilinogen cycle. The remainder is transported by the blood to the kidney converted to yellow urobilin and excreted giving urine its yellow coior.
The hyperbilirubinemia is caused by mutation in the gene encoding, the protein involved in the secretion of congugated bilirubin into the bile.