
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dental Charting, Color Coding and Symbols: Class Activity
Similar to Dental Charting, Color Coding and Symbols: Class Activity (20)
More from HeatherSeghi
More from HeatherSeghi (20)
Recently uploaded
Recently uploaded (20)
Dental Charting, Color Coding and Symbols: Class Activity
- 2. Key Terms ◦ furcation – Area where the root portion of a tooth divides. ◦ gingivitis – Inflammation of the gingiva. ◦ morphology – Study of the structure and form of living organisms. ◦ periodontal disease – Site-specific infection of the dental supporting structures. ◦ periodontal probe – Hand instrument with millimeter calibrations used to measure pocket depth, attachment width, and size of soft tissue lesions. ◦ periodontitis – Inflammation of the periodontium that extends beyond the gingiva.
- 3. Key Terms ◦ periodontium – Tissues that surround and support the teeth, i.e., the gingiva, cementum, periodontal ligament, alveolar bone, and supporting bone. ◦ pocket depth – Distance in millimeters from the gingival margin to the base of the pocket. ◦ prognosis – Foretelling the probable course of a disease, as well as forecasting the outcome of a disease or regimen of treatment. ◦ recession – Loss of part or all of the gingiva covering the root of a tooth. ◦ treatment plan – Sequence of procedures planned for the treatment of a patient.
- 4. Charting Colors and Systems ◦ Colors (red/blue) and symbols are used in charting to indicate the condition of the patient’s teeth and surrounding tissues and the restorative services required. ◦ In some cases, it may be appropriate to use either color. ◦ An example would be that a patient has a fracture (red), but no discomfort or appearance issues(blue); therefore, a notation is made on the chart that nothing is to be done at this time and charted in either color.
- 5. Charting Colors and Systems ◦Red ◦Indicates work to be completed ◦Blue ◦Indicates completed work ◦Lines and fill-ins ◦Indicate restoration type
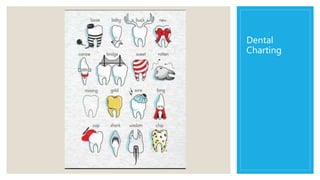
- 6. Charting (completed work) ◦ Amalgam restoration (outlined and filled solid blue when complete or red when to be done) ◦ Composite restoration (outlined in red when to be done or blue when complete) ◦ Gold restoration (area outlined with diagonal lines, red when to be done or blue when complete) ◦ Porcelain restoration (outlined with red when to be done or blue when complete and/or P inside the outline) ◦ Sealant (S on occlusal surface, red when to be done or blue when complete) ◦ Stainless steel (outlined with swervy lines through it or two Ss inside it, red when to be done or blue when complete).
- 7. Charting
- 8. Charting
- 9. Charting
- 10. Charting
- 15. Charting
- 17. Charting
- 19. #1 Impacted #2 Class II DO amalgam restoration present #4 Class II MOD amalgam restoration present #6 Class III M composite restoration present #8 Class IV MIFL composite restoration present #8 #9 Diastema present #9 Class III M decay #13 Class II MOD amalgam restoration with recurrent decay #14 Class II MO amalgam restoration present; food impaction between 13 and 14 #16 Has been removed
- 20. #17 Partially impacted and must be removed #19 Bridge present, abutment full gold crown #20 Bridge present, pontic porcelain with gold #21 Bridge present, abutment porcelain with gold #24 Mobility of III, periodontal pocket on M and D of 4 mm each, heavy calculus from mandibular left cuspid to mandibular right cuspid #25 Periodontal pocket on M and D of 3 mm each #28 Needs a full gold crown with a porcelain facing #28 Has a completed root canal #30 Class I O decay #31 Class II MO amalgam restoration present #32 Has been removed
- 21. Computer programs ◦ The computerized systems of today work wonderfully. ◦ Although there are many dental software programs, they are easily learned. ◦ You can use voice-activated systems, light pen systems, or use a covered keyboard (to keep it sanitary). ◦ Dental assistants can become very proficient at computer charting. ◦ The software programs can handle periodontics, conditions of dentition, tissue, occlusion, or any notations the dentist or auxiliary would like. ◦ We will learn how to use Eaglesoft for paperless charting.
- 26. Can you chart these conditions?
- 27. Bridge ◦A fixed prosthetic device placed in the mouth to replace missing teeth
- 28. Abutment ◦A tooth, a root, or an implant for retaining a fixed or removable prosthesis; the teeth adjacent to a pontic in a bridge ◦Which is the abutment?
- 29. Pontic ◦ Portion of the bridge that replaces the missing teeth
- 30. What does this mean?
- 31. Maryland Bridge ◦A resin-retained, fixed bridge that replaces one tooth
- 32. Can you chart this condition?
- 33. Inlay, Onlay
- 34. What is the difference?
- 35. Cantilever bridge ◦Prosthetic device in mouth attached at only one side; useful in area with little stress such as a missing lateral
- 36. Fractured tooth or root
- 37. Can you chart these conditions?
- 38. Can you chart these conditions?
- 39. Veneer
- 40. How can you tell? ◦What’s the difference between a crown and a veneer?
- 41. Dental Implant • Used to replace a missing tooth or teeth. • There are different types • You can use in conjunction with a crown, or use to support a partial or complete denture
- 42. Can you chart these conditions?
- 43. Incipient ◦Beginning tooth decay that has no broken through the enamel into the dentin
- 44. Denture ◦A prosthesis that replaces missing teeth in the same arch ◦Partial ◦Full
- 45. Mobility ◦Tooth movement in the socket; may be due to periodontal disease or trauma
- 46. Mobility ◦ Mobility is an indicator of bone loss around the tooth. ◦ In order to accurately evaluate mobility, two non-working ends of the dental instruments (i.e., the mirror handle and the probe handle) are pressed on the buccal and lingual surfaces of the tooth.
- 47. Mobility Classification Class O Complete tooth stability. Class I Tooth moves ½ mm buccally and ½ mm lingually. Class II All degrees between Class I and Class III mobility of up to 1 mm in any direction. Class III Tooth is terminally mobile; movement is greater than 1 mm in any direction and is depressible in the socket.
- 48. Drifting ◦Moving a tooth into the space created by a missing tooth
- 49. Can you chart these conditions?
- 50. Diastema ◦Space between maxillary central incisors in humans; can also be used to denote a space between two adjacent teeth in the same arch
- 51. Can you chart this condition?
- 52. Overhang ◦Excess restorative material projecting over the cavity margin
- 53. Can you Chart these conditions?
- 54. Partial Dentures ◦Prosthetic devices containing artificial teeth supported on metal frameworks and attached by clasps to natural teeth
- 55. Root Canal ◦Where the pulp is removed and replaced with a filling material
- 56. Can you chart these conditions?
- 57. Abscess ◦Local Area of pus and infection ◦Caused by?
- 58. Can you chart these conditions?
- 59. Gingival Recession ◦ Gingival recession is important to the periodontal examination because it accurately indicates the total amount of attachment loss. ◦ Attachment loss can vary from tooth to tooth. A tooth can have attachment loss without having a pocket. ◦ The amount of attached gingiva can be calculated by subtracting the probing depth from the width of the keratinized gingiva. ◦ Tissue appearance for keratinized tissue is lighter pink with a stippled appearance.
- 60. Can you chart these conditions?
- 61. Periodontal Pocket ◦ Space in the gingival sulcus (beyond the normal 1-3mm) created by periodontal disease
- 63. How to read a perio probe:
- 65. Periodontal Probing Disadvantages ◦Even though periodontal probing is one of the best diagnostic tools to assess periodontal disease, there are also certain pitfalls to avoid: ◦ subgingival calculus can interfere with accurate readings ◦ in an area with elevated inflammation, the attachment is easily perforated ◦ the pocket may be too tight to probe ◦ the patient may present with hypersensitivity making accurate probing difficult
- 66. Periodontal Disease Type I Gingivitis No loss of attachment Bleeding on probing may be present Type II Early Periodontitis Pocket depth or attachment loss: 3-4mm Bleeding on probing may be present Localized area of gingival recession Possible grade I furcation involvement Type III Moderate Periodontitis Pocket depths or attachment loss 4-6 mm Bleeding on probing Grade I or II furcation involvement Class I mobility Type IV Advanced Periodontitis Pocket depths or attachment loss >6 mm Bleeding on probing Grade II or III furcation involvement Class II or III mobility Type V Refractory & Juvenile Periodontitis Periodontitis not responding to conventional therapy or which recurs soon after treatment. Juvenile forms of periodontitis.
- 67. Furcation Classification ◦Furcation involvement indicates a serious periodontal condition that can affect multi-rooted teeth. ◦If it is detected early, it is treatable with guided tissue regeneration. ◦Frequently, the areas that are most vulnerable to furcation involvement (the posterior areas of the mouth) are difficult to access. ◦As a result, abscesses, progressive attachment loss, and deep periodontal pockets may develop and be undetected.
- 68. The four classes of furcation involvement that are identified with the Naber’s probe are: Class I The furcation can be probed to a depth of 3 mm. Using the probe, the anatomic fluting between the roots can be felt, but cannot engage the roof of the furcation. Class II The furcation can be probed to a depth greater than 3 mm, but not through and through. Class III The furcation can be completely probed through and through subgingivally. Class III+ Naber’s probe can go halfway across the tooth. Class IV The probe goes completely through the furcation and is supragingival.
- 69. Can we identify?
- 70. Sealant ◦ Enamel sealant is a resin material used to seal pits and fissures to prevent future decay
- 71. Restoration ◦Process of replacing missing tooth structure; results in “fillings”
- 72. Charting ◦If an anterior tooth is fractured and needs to be restored, which color would it be charted in and why? ◦What if its fractured, but not causing pain, and the dentist doesn’t feel its necessary to repair at this time?
- 73. Charting ◦What are the five surfaces on an anterior tooth? ◦Which of these surfaces is the same for both anterior and posterior?
- 74. Charting ◦Why do we use F for facial instead of L for labial, even though they are the same surface?
- 75. Charting ◦A young adult broke his upper teeth at a drinking fountain, from the middle of the biting edge to the middle of each front tooth in an upside-down V pattern. ◦Which surfaces, classifications, and teeth numbers would be involved if using the: ◦Universal System for numbering? ◦The FDI system? ◦The Palmer System?
- 77. Answer key ◦ Tooth #1 is missing (charted in blue) with retained root tip (charted in red) ◦ Tooth #2 existing MOD amalgam (charted in blue) with mesial overhang (charted in red) ◦ Tooth #3 gingival recession with furcation involvement (charted in red) ◦ Tooth #4 existing porcelain fused-to-metal crown (charted in blue) ◦ Tooth #5 existing sealant (charted in blue) ◦ Tooth #6 existing implant (charted in blue), needs porcelain fused to HNM crown (charted in red) ◦ Tooth #7 existing DF composite (charted in blue) ◦ Tooth #8 has a MI fracture or MI caries (charted in red) ◦ Tooth #9 has an all ceramic or all porcelain crown (charted in blue) ◦ Tooth #10 has a DI composite (charted in blue) ◦ Between tooth numbers 11-12 there is an open contact or diastema (charted in blue) ◦ Tooth #11 is sound ◦ Tooth #12 existing DO amalgam with recurrent caries (charted in blue, outlined in red) ◦ Tooth #13 has MOD caries, composite treatment planned (charted in red) ◦ Tooth #14 existing porcelain fused to HNM crown - three-unit bridge (charted in blue) ◦ Tooth #15 existing HNM crown (pontic) - three-unit bridge (charted in blue) ◦ Tooth #16 existing HNM crown (abutment) - three-unit bridge (charted in blue) Maxillary
- 78. Answer Key ◦ Tooth #17 fully erupted, to be extracted (charted in red) ◦ Tooth #18 existing stainless steel crown (charted in blue) ◦ Between 18-19 food impaction (charted in red) ◦ Tooth #19 existing MODFL amalgam (charted in blue) ◦ Tooth #20 endontically treated with post and core (charted in blue) ◦ Tooth #21 rotated to the distal (charted in red) ◦ Tooth #22 existing lingual amalgam (charted in blue) ◦ Tooth #23 existing porcelain veneer (charted in blue) ◦ Tooth #24 existing retainer for Maryland bridge (charted in blue) ◦ Tooth #25 existing Maryland pontic (charted in blue) ◦ Tooth #26 existing retainer for Maryland bridge (charted in blue) ◦ Tooth #27 existing F composite (charted in blue) ◦ Tooth numbers 27 – 30 existing lingual tori (charted in blue) ◦ Tooth #28 is sound ◦ Tooth #29 existing periapical abscess; tooth is extruded (charted in red) ◦ Tooth #30 needs an occlusal sealant; tooth has drifted medially; has class V buccal caries (charted in red) ◦ Tooth #31 missing (charted in blue) ◦ Tooth #32 is impacted and horizontal (charted in red) Mandibular
- 79. Eaglesoft Perio Probe FINDINGS USE BUTTON DISPLAY Mobility Grade MOB MOB Pocket Depth Measurement PD PD Gingival Margin Measurement GM GM Clinical Attachment Level Automatically Calculated CAL Mucogingival Junction MGJ MGJ Furcation Grade FG FG Bleeding Bleeding Colors Site Dot Bleeding All Bleeding all pockets Colors Site Dot Suppuration Suppuration Colors Site Dot Suppuration All Suppuration all pockets Colors Site Dot Bleeding and Suppuration Bleeding and Suppuration Colors Site Dot Definitions
- 80. Suppuration ◦The process of pus formation, called suppuration, occurs when the agent that provoked the inflammation is difficult to eliminate. ◦Pus is a viscous liquid that consists mostly of dead and dying neutrophils and bacteria, cellular debris, and fluid leaked from blood vessels.
- 81. SOAP notes ◦ The patient chart is a legal record of dental services. Information noted must be accurate, comprehensive, concise and current. ◦ During an initial oral exam, data recorded includes conditions present and any previous dental treatment provided. ◦ Dental SOAP notes are written to improve communication among all those caring for the patient by standardizing evaluation entries made in dental charts. ◦ Each letter in “SOAP” is a specific heading in the notes.
- 82. SOAP notes ◦ S – refers to subjective, the purpose of the patient’s dental visit. This section also includes the description of symptoms in the patient’s own words including: pain, what triggers the discomfort, what causes the discomfort to disappear and the length of time these symptoms have been occurring. ◦ O – refers to objective, unbiased observations by the dental team. Included under this heading would be things that can actually be felt, heard, measured, seen, smelled and touched. ◦ A– refers to assessment, the diagnosis of the patient’s condition done by the dentist. The diagnosis may be clear or there may be several diagnostic possibilities. ◦ P – refers to the plan or proposed treatment, and is decided upon by the patient and the dentist. ◦ The plan may include radiographs, medications prescribed, dental procedures, patient referral to specialists and patient follow-up care instructions.
- 83. SOAP notes ◦ A SOAP notation is not supposed to be as detailed as a progress report and the usage of abbreviations is standard. ◦ Abbreviations will vary slightly from one practice to another, so it is important to use notations commonly used within the practice. ◦ It is imperative that the individual making the notation sign their name and list their credentials so that those reading the record know who was responsible for the notes. ◦ Notes should be free from scribbles and whiteout errors. ◦ If an error is made, a single line should be drawn through the error, dated and initialed, and the correction written. ◦ Corrections in computerized formats will vary according to dental software. ◦ Notations should be written fluently and without blank lines between the entries. ◦ This will prevent additional information being added without the writer’s knowledge.