Climate Change Impacts on Terrestrial and Aquatic Ecosystems.pptx
Chronic Pancreatitis.pdf
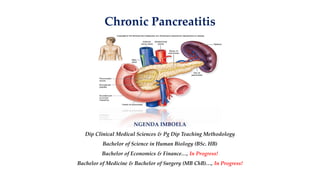
1. Chronic Pancreatitis
NGENDA IMBOELA
Dip Clinical Medical Sciences & Pg Dip Teaching Methodology
Bachelor of Science in Human Biology (BSc. HB)
Bachelor of Economics & Finance…, In Progress!
Bachelor of Medicine & Bachelor of Surgery (MB ChB)…, In Progress!
2. Chronic Pancreatitis
❑ It is persistent progressive irreversible damage of the
pancreas due to chronic inflammation. Chronic pancreatitis is
more common in males
❑It can either be
1. Chronic relapsing pancreatitis
2. Chronic pancreatitis (persistent)
1. Chronic non-calcifying
2. Calcifying pancreatitis pancreatitis
3. Key Facts
❑Characterized by recurrent or persistent abdominal pain
arising from the pancreas.
❑Often associated with exocrine or endocrine pancreatic
insufficiency.
❑Characterized by irreversible destruction and fibrosis of
pancreatic parenchyma.
❑May arise following one or more episodes of acute
pancreatitis or may be a chronic progressive process de novo
4. Pathological Features
❑Alcohol reduces pancreatic blood flow, alters cell viability,
releases the free radicals, creates pancreatic ischaemia, and
activates the pancreatic stellate cells which produce abundant
extracellular matrix and collagen.
❑Genetic predisposition may be the cause of idiopathic
pancreatitis. Mutation in pancreatic secretory trypsin
inhibitor causes activation of trypsin causing pancreatitis
❑The process may affect the whole or part of the gland (focal).
5. Pathological Features
❑The head tends to be the most severely involved part in
chronic alcohol disease.
❑Features of acute pancreatitis may occur—oedema, acute
inflammatory infiltrate, focal necrosis, intraparenchymal
haemorrhage.
❑Chronic inflammatory changes cause progressive
disorganization of the pancreas:
❑Glandular atrophy and duct ectasia.
❑Microcalcification and intraductal stone formation with cystic
changes secondary to duct occlusion.
6. Causes and Clinical Features
❑Recurrent acute pancreatitis of any cause, especially alcohol.
❑Secondary to pancreatic ductal obstruction:
❑Pancreatic head cysts, tumours.
❑Pancreatic duct strictures—post-surgery, ERCP, parasitic infestation.
❑Congenital pancreatic abnormalities (pancreas divisum, annular
pancreas).
❑Cystic fibrosis.
❑Associated with autoimmune diseases (primary biliary
cirrhosis, primary sclerosing cholangitis).
❑Congenital idiopathic chronic pancreatitis
7. Features of Chronic Inflammation
❑Recurrent or chronic abdominal pain:
❑Typically epigastric, radiating to the back and requiring
opiates.
❑Worse with food, alcohol.
8. Features of Exocrine Failure
❑Anorexia and weight loss (due to protein malabsorption).
❑Steatorrhoea (due to fat malabsorption); soft, greasy, foul-
smelling stools that typically float on water.
❑Features of endocrine failure Insulin-dependent diabetes
mellitus (due to loss of β islet cells).
9. Diagnosis and Investigations
❑Plain abdominal X-ray may show pancreatic calcification.
❑Abdominal ultrasound may show cystic change and duct
dilatation within the pancreas.
❑Pancreatic CT scan: May identify a cause, e.g. anatomical
variants, tumours, cysts.
❑May show extent of disease. Pancreatic atrophy,
disorganization of pancreatic ducts, altered acinar pattern
with fibrosis, calcification, and cystic change.
10. Diagnosis and Investigations
❑MRI scan. May show the same changes as CT.
❑Endoscopic Retrograde Cholangio-Pancreatograghy (ERCP).
Demonstrates irregularity of the pancreatic duct strictures,
calculi, dilated segments (‘chain of lakes’), and changes in
first and second order branches and cyst formation;
❑A secondary effect from involvement of the head is stricture
of the bile duct, leading to an ‘obstructive’ pattern of LFTs.
11. Treatment
❑Prevention of cause/progressive damage.
❑Stop alcohol, deal with gallstones, treat autoimmune
disease.
❑Encourage a diet rich in antioxidants (vitamins A, C, E,
selenium).
12. Treatment
❑Control symptoms/complications.
❑Dietary modifications. Adequate carbohydrates and
protein, reduced fat.
❑Pancreatic exocrine enzyme supplements (e.g. Creon®).
❑Analgesia. May require opiates (e.g. MST) or coeliac
plexus block.
❑Control of diabetes mellitus often requires insulin; control
is often difficult due to variable pancreatic function
13. Surgical Treatment
❑Indications include the following.
❑Treatment of reversible cause (anatomical abnormalities,
tumours, cysts, ductal strictures and stones). Operations used
include those to remove causes and those to drain an
obstructed pancreatic duct:
❑Pancreaticoduodenectomy (Whipple procedure).
❑Partial pancreatectomy of the head (Frey procedure) or tail
(distal pancreatectomy).
❑Pancreaticojejunostomy (Peustow or Duval procedure).
14. Surgical Treatment
❑Indications include the following.
❑Treatment of severe intractable pain or multiple relapses.
Operations are usually to resect affected portion:
❑Partial pancreatectomy of the head (Frey procedure) or tail
(distal pancreatectomy).
❑Total pancreatectomy
❑Complications (pseudocyst, obstruction, fistula, infections,
portal hypertension).
15. Outcome
❑Resectional surgery is associated with increasing risk of
exocrine and endocrine pancreatic failure and high risk of
complications.
❑All surgery is associated with a risk of symptom recurrence
due to recurrent or progressive disease.