Downloaded 175 times








1) The document discusses several theories of aging at the biological, psychological, and social levels. It covers theories such as lifespan development theory, selective optimization with compensation theory, and socioemotional selectivity theory. 2) Cognitive theories of aging propose that fluid abilities decline with age while crystallized abilities remain more stable or increase. Changes in processing speed, working memory, and sensory perception are well documented in aging. 3) Personality theories focus on stability of traits over the lifespan as well as changes in goals, values, and coping styles. Core personality remains stable in aging while priorities and coping strategies may subtly change.










































































































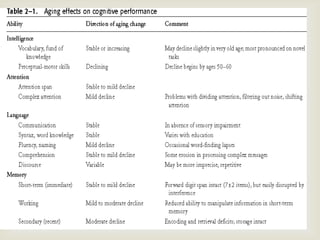
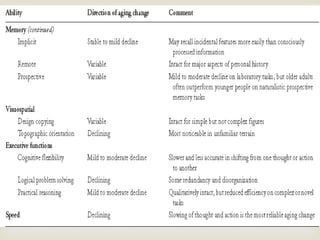
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
