Downloaded 186 times





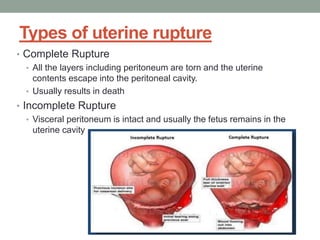







Uterine rupture is the tearing of the uterine wall during pregnancy or childbirth, with symptoms such as increased pain and bleeding not always present. It occurs after 28 weeks of gestation and is associated with risk factors like previous cesarean sections and high parity, with an incidence rate of about 0.9% in vaginal births following one prior cesarean. Key complications include high fetal mortality and the need for interventions such as laparotomy or hysterectomy in severe cases.



































































